Download as ppt, pdf, or txt
You might also like
- Karyotypes Diagnosing Chromosome AbnormalitiesDocument8 pagesKaryotypes Diagnosing Chromosome AbnormalitiesKennedy HammondNo ratings yet
- 03 Bone Non-Neoplastic Part-1Document52 pages03 Bone Non-Neoplastic Part-1dryunusaqNo ratings yet
- Hydrocephalus IDocument52 pagesHydrocephalus IVlad Alexandra50% (2)
- Digeorge Syndrome Research PaperDocument5 pagesDigeorge Syndrome Research Paperapi-386698528No ratings yet
- Spina BifidaDocument27 pagesSpina BifidaSandy VillarNo ratings yet
- Chromosomal DisordersDocument4 pagesChromosomal DisordersYoussry JaranillaNo ratings yet
- Genetics: B.Sc. NursingDocument199 pagesGenetics: B.Sc. NursingRohini Keshava100% (1)
- 3 Neonatal InfectionDocument56 pages3 Neonatal InfectiondindaamalaNo ratings yet
- Edward Syndrome: Submitted byDocument11 pagesEdward Syndrome: Submitted byFrancine RoxasNo ratings yet
- Ch15 Chromosomal AbnormalitiesDocument17 pagesCh15 Chromosomal AbnormalitiesMaduranga Jayasundara100% (1)
- Congenital Anomalies: Pooja K MenonDocument73 pagesCongenital Anomalies: Pooja K Menonpujitha2002100% (2)
- 14 - Complex Pattern of Inheritance Notes PPT Part 2Document24 pages14 - Complex Pattern of Inheritance Notes PPT Part 2api-3752850210% (1)
- Neuropathology: FK UisuDocument28 pagesNeuropathology: FK UisuAnggi WahyuNo ratings yet
- Pathology of Blood VesselsDocument28 pagesPathology of Blood Vesselsdhainey100% (1)
- Ch13 ChromosomesDocument61 pagesCh13 ChromosomesJJ Almagro100% (1)
- Cellinjury 151004125508 Lva1 App6892Document147 pagesCellinjury 151004125508 Lva1 App6892Ajmal RockzzNo ratings yet
- S.Y.B.Sc Semester III Botany Paper II Unit II:CytogeneticsDocument95 pagesS.Y.B.Sc Semester III Botany Paper II Unit II:CytogeneticsQueen1982 K100% (1)
- Psych - Elimination DisordersDocument17 pagesPsych - Elimination Disordersapi-3856051No ratings yet
- Genetic and Pediatric DiseasesDocument88 pagesGenetic and Pediatric DiseasesJaneNo ratings yet
- Anatomy of The Parotid GlandDocument28 pagesAnatomy of The Parotid GlandHossam NawaraNo ratings yet
- Population DynamicsDocument25 pagesPopulation Dynamicsapi-375285021No ratings yet
- Calcium Metabolism & Calcium Metabolism DisordersDocument45 pagesCalcium Metabolism & Calcium Metabolism Disorderstrisya arthaputriNo ratings yet
- HypoglycemiaDocument34 pagesHypoglycemiaPrince Mendel100% (1)
- Cytogenetics: Chromosome Banding & Barr Body DR Charu Khosla, 24/4/20, 10.45-11.45 AmDocument90 pagesCytogenetics: Chromosome Banding & Barr Body DR Charu Khosla, 24/4/20, 10.45-11.45 Amsonal aranha100% (2)
- Gyne - Case 15 Benign Lesions of The Vulva & VaginaDocument2 pagesGyne - Case 15 Benign Lesions of The Vulva & Vaginacbac1990No ratings yet
- 4 Pedigree AnalysisDocument48 pages4 Pedigree AnalysisBiologistAhmedNo ratings yet
- Central Nervous System AbnormalitiesDocument56 pagesCentral Nervous System AbnormalitiesApin PokhrelNo ratings yet
- Cyclic NeutropeniaDocument9 pagesCyclic Neutropeniawafae moutanaNo ratings yet
- Lecture 16 IEN of The Lower Genital TractDocument16 pagesLecture 16 IEN of The Lower Genital TractCharisse Angelica MacedaNo ratings yet
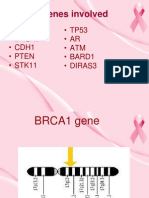
- Genetics of Breast CancerDocument29 pagesGenetics of Breast CancersbsiansNo ratings yet
- Cyanotic CHDDocument64 pagesCyanotic CHDKUMARAVELNo ratings yet
- Genetic DiseasesDocument15 pagesGenetic DiseasesSelena Spears100% (1)
- SEX-LINKED Inheritance - 6 PDFDocument36 pagesSEX-LINKED Inheritance - 6 PDFMikko Cagnayo0% (1)
- Acute Bacterial MeningitisDocument49 pagesAcute Bacterial MeningitisKumara GuruNo ratings yet
- Overview of Pediatric GeneticsDocument12 pagesOverview of Pediatric Geneticsnicdeep100% (1)
- Gene Therapy For CancerDocument7 pagesGene Therapy For Canceresraa elsharkawyNo ratings yet
- 2 - Modes of InheritanceDocument42 pages2 - Modes of InheritanceSimon Grant100% (1)
- Notes - Human GeneticsDocument68 pagesNotes - Human GeneticsiwennieNo ratings yet
- Chapter 5 - Displacement of UterusDocument25 pagesChapter 5 - Displacement of Uterusاسامة محمد السيد رمضانNo ratings yet
- Krizia Joy Borromeo-Galve, MD: Bulacan Medical Center, Department of PediatricsDocument84 pagesKrizia Joy Borromeo-Galve, MD: Bulacan Medical Center, Department of PediatricsTara Oliveros Dela CruzNo ratings yet
- Edwards Down SyndromeDocument5 pagesEdwards Down Syndromeapi-346355246No ratings yet
- Sry Sex DeterminationDocument15 pagesSry Sex Determinationapi-528179516100% (1)
- LEC 05 - Growth - Puberty DisordersDocument58 pagesLEC 05 - Growth - Puberty DisordersIoana CozmaNo ratings yet
- Brain AbscessDocument25 pagesBrain AbscessprembarnabasNo ratings yet
- Vasculitis ReviewDocument132 pagesVasculitis Reviewajmal_rashid@hotmail.com100% (2)
- 050 PPT - RetinoblastomaDocument61 pages050 PPT - RetinoblastomaAnastasia TjanNo ratings yet
- Caserian SectionDocument100 pagesCaserian SectionsindhujojoNo ratings yet
- Salivary GlandsDocument36 pagesSalivary GlandsNithish Reddy100% (1)
- Endocrine System Pathology 2009Document195 pagesEndocrine System Pathology 2009SofiaemanginteNo ratings yet
- Cancer EpigeneticsDocument48 pagesCancer EpigeneticsIqra SultanNo ratings yet
- Birth Defects and Prenatal DiagnosisDocument137 pagesBirth Defects and Prenatal DiagnosisSohera Nadeem100% (1)
- Developmental Anomalies of Spinal CordDocument41 pagesDevelopmental Anomalies of Spinal Cordhamza_shoaib99No ratings yet
- Common Childhood Skin Diseases PowerPointDocument51 pagesCommon Childhood Skin Diseases PowerPointNagulan Nagul100% (1)
- Kaposis Sarcoma: Denis NahabweDocument32 pagesKaposis Sarcoma: Denis NahabwexilcomNo ratings yet
- Hemolytic Disease of The NewbornDocument14 pagesHemolytic Disease of The Newbornapi-441635248No ratings yet
- Genetic Basis of Disease PMDocument79 pagesGenetic Basis of Disease PMsunday daniel100% (1)
- Graft Versus Host DiseaseDocument14 pagesGraft Versus Host DiseaseBoutheyna MahmoudNo ratings yet
- Toxic Epidermal NecrolysisDocument13 pagesToxic Epidermal NecrolysisHend AbdallaNo ratings yet
- Chromosome Nactivation: Babak Nami Department of Medical Genetics Selçuk UniversityDocument19 pagesChromosome Nactivation: Babak Nami Department of Medical Genetics Selçuk UniversityBabak Nami100% (1)
- Chromosome Abnormalities and Sex DeterminationDocument43 pagesChromosome Abnormalities and Sex DeterminationprasadbheemNo ratings yet
- Turner Syndrome, Klinefelter Syndrome, Down SyndromeDocument78 pagesTurner Syndrome, Klinefelter Syndrome, Down SyndromeTasya100% (3)
- PCPNDT ActDocument25 pagesPCPNDT ActHema Anand100% (1)
- Gastroschisis Final PresentationDocument43 pagesGastroschisis Final PresentationlhedavenNo ratings yet
- The Development of The Study of DermatoglyphicsDocument7 pagesThe Development of The Study of DermatoglyphicsHomework PingNo ratings yet
- Maternal and ChildDocument45 pagesMaternal and ChildShiela Joy DuquezNo ratings yet
- Sle-Cad Module 11Document4 pagesSle-Cad Module 11vanalloutNo ratings yet
- Laboratory Test During PregnancyDocument10 pagesLaboratory Test During PregnancyJoan Venida100% (1)
- Trisomie 21 AnglaisDocument34 pagesTrisomie 21 AnglaisKatia Hareb-CherfaouiNo ratings yet
- Rajiv Gandhi University Thesis Topics in PeriodonticsDocument4 pagesRajiv Gandhi University Thesis Topics in Periodonticsafcnoxdhv100% (1)
- Internship Report WritingDocument6 pagesInternship Report WritingDeekshitha RaNo ratings yet
- R V Giesbrecht, 2019 MBCA 35Document79 pagesR V Giesbrecht, 2019 MBCA 35ElishaDaceyNo ratings yet
- The Neonatal Intubation Causes Defects in PrimaryDocument9 pagesThe Neonatal Intubation Causes Defects in PrimaryfatimahNo ratings yet
- Assessment of Fetal G&DDocument75 pagesAssessment of Fetal G&DHillary Praise AquinoNo ratings yet
- Hydrops Fetalis With Septated Cystic Hygroma: Case ReportDocument3 pagesHydrops Fetalis With Septated Cystic Hygroma: Case ReportYosita AuroraNo ratings yet
- Applied Pathophysiology A Conceptual Approach To The Mechanisms of Disease 3rd Edition Braun TEST BADocument105 pagesApplied Pathophysiology A Conceptual Approach To The Mechanisms of Disease 3rd Edition Braun TEST BAmary011danielNo ratings yet
- Chih-Ping ChenDocument4 pagesChih-Ping ChenWill Hans YuliusNo ratings yet
- Acog Practice Bulletin: Pregestational Diabetes MellitusDocument21 pagesAcog Practice Bulletin: Pregestational Diabetes MellitusGia DuyNo ratings yet
- HDFC IpaDocument16 pagesHDFC IpaFarshid BokdawallaNo ratings yet
- Junior Assistant Syllabus PDFDocument29 pagesJunior Assistant Syllabus PDFAnil SharmaNo ratings yet
- Group PolicyDocument14 pagesGroup PolicyMahesh DivakarNo ratings yet
- Birth DefectsDocument36 pagesBirth DefectsSohera NadeemNo ratings yet
- Anorectal Malformations HandoutDocument4 pagesAnorectal Malformations HandoutShikha Acharya100% (2)
- Developmental Disabilities Lecture 1Document13 pagesDevelopmental Disabilities Lecture 1Dr Muhammad NadeemNo ratings yet
- Introduction To Modern Concept of Childcare & History, Principles & Scope of Child Health NursingDocument17 pagesIntroduction To Modern Concept of Childcare & History, Principles & Scope of Child Health Nursingsuper cool100% (2)
- Prenatal DevelopmentDocument33 pagesPrenatal DevelopmentDexter Nario0% (1)
- High Risk PregnancyDocument8 pagesHigh Risk PregnancyIbrahim AdnanNo ratings yet
- WwerDocument2 pagesWwerMahdi AlattasNo ratings yet
- Medical MnemonicsDocument15 pagesMedical MnemonicsPrashantVedwanNo ratings yet
- 14 Congenital Anomalies of CNSDocument5 pages14 Congenital Anomalies of CNSBella DonnaNo ratings yet
- Preventive ObstetricsDocument57 pagesPreventive ObstetricsGunaNo ratings yet