Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Mercy Obstetric Triage OTDA A Standardised Approach To Care CHA SlidesDocument28 pagesMercy Obstetric Triage OTDA A Standardised Approach To Care CHA Slidessaepulloh bin amingNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Trends and Issues in MSNDocument26 pagesTrends and Issues in MSNAmmineni Syam Prasad100% (8)
- Trauma Scoring System: Edi MustamsirDocument28 pagesTrauma Scoring System: Edi Mustamsireka_wahyuningsih100% (1)
- Continuous Integrated TriageDocument4 pagesContinuous Integrated TriagemisanthropoNo ratings yet
- Summary of Primary Survey ATLS Bahan AjarDocument141 pagesSummary of Primary Survey ATLS Bahan AjarJohannes CordeNo ratings yet
- NABH 5th Edition - COP - Emergency ServicesDocument14 pagesNABH 5th Edition - COP - Emergency ServicesanithaNo ratings yet
- Quick Healthcare Stencil: SketchDocument2 pagesQuick Healthcare Stencil: SketchNafiz Hannan NabilNo ratings yet
- Emergency MedicineDocument141 pagesEmergency Medicinenasibdin100% (9)
- Fitriani, Et AlDocument14 pagesFitriani, Et AlwidyadariNo ratings yet
- Roberto Padlan (Resume)Document5 pagesRoberto Padlan (Resume)Merian PadlanNo ratings yet
- Acute Care For Burn Patients Fluids, Surgery, and What ElseDocument6 pagesAcute Care For Burn Patients Fluids, Surgery, and What ElseReywersonNo ratings yet
- Emergency Nursing Post TestDocument25 pagesEmergency Nursing Post TestAngie RelosNo ratings yet
- Simulation BasicsDocument94 pagesSimulation Basicspammy313100% (1)
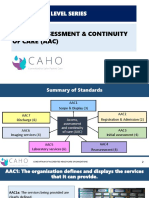
- AAC-Entry Level SeriesDocument51 pagesAAC-Entry Level SeriesPallavi Deepak DongreNo ratings yet
- Fung Et - Al.Document6 pagesFung Et - Al.Noi Mae NebreaNo ratings yet
- Malaysia ICU Protocol Management 2019 PDFDocument94 pagesMalaysia ICU Protocol Management 2019 PDFNokoline HuNo ratings yet
- Homework Task 1Document10 pagesHomework Task 1Alyxen PelingenNo ratings yet
- Triage Protocols For Aging Adults First Edition Ebook PDF VersionDocument61 pagesTriage Protocols For Aging Adults First Edition Ebook PDF Versionbetty.washington515100% (39)
- Assessment of The Trauma Patient PDFDocument25 pagesAssessment of The Trauma Patient PDFcotovairinax100% (1)
- Hospital Disaster Management Guidelines: Directorate of Health Services, KeralaDocument56 pagesHospital Disaster Management Guidelines: Directorate of Health Services, KeralaPrasetya PerwiraNo ratings yet
- Module1 Emergency BasicDocument3 pagesModule1 Emergency Basicmitchie riveraNo ratings yet
- Comm ProcDocument20 pagesComm ProccarolNo ratings yet
- Curiculum Vitae Djohansjah MarzoekiDocument25 pagesCuriculum Vitae Djohansjah Marzoekiwidya novianiNo ratings yet
- Disaster Management and Nurses RoleDocument34 pagesDisaster Management and Nurses RoleMebin NinanNo ratings yet
- Care Planning Practice Guide (Modul 9)Document44 pagesCare Planning Practice Guide (Modul 9)diankristianaNo ratings yet
- DR Mohd Suhaimi Tajudin Overview TriageDocument39 pagesDR Mohd Suhaimi Tajudin Overview Triageshinichi kudoNo ratings yet
- Trauma Protocol Manual Final 2012 WordDocument250 pagesTrauma Protocol Manual Final 2012 WordelaNo ratings yet
- Eac 139-24 (4-2021Document80 pagesEac 139-24 (4-2021Sherief ArafatNo ratings yet
- Lunch Symposium Dr. Fanny Indarto, SPB - Multiple vs. Mass Casualties ManagementDocument17 pagesLunch Symposium Dr. Fanny Indarto, SPB - Multiple vs. Mass Casualties ManagementThomas Kwee100% (1)
- Epidemiology of Traumatic Spinal Cord Injury: A SAARC PerspectiveDocument14 pagesEpidemiology of Traumatic Spinal Cord Injury: A SAARC PerspectivejazelNo ratings yet