
IMCI
IMCI
You might also like
- Nurse Deployment Program (NDP) Examination NotesDocument44 pagesNurse Deployment Program (NDP) Examination Notesdeeday echavez93% (27)
- Medical-Surgical Nursing ReviewDocument90 pagesMedical-Surgical Nursing Reviewɹǝʍdןnos99% (316)
- Pathognomonic SignsDocument3 pagesPathognomonic Signsɹǝʍdןnos100% (21)
- Community Health Nursing Examination Part IDocument17 pagesCommunity Health Nursing Examination Part Iɹǝʍdןnos97% (64)
- ABG InterpretationDocument31 pagesABG Interpretationɹǝʍdןnos100% (12)
- Nursing Research ReviewDocument13 pagesNursing Research Reviewɹǝʍdןnos96% (50)
- The 3D Printing Handbook - Technologies, Design and ApplicationsDocument347 pagesThe 3D Printing Handbook - Technologies, Design and ApplicationsJuan Bernardo Gallardo100% (7)
- Nursing Practice 1Document62 pagesNursing Practice 1ɹǝʍdןnos100% (2)
- NLE Compilation 1Document67 pagesNLE Compilation 1blazegomez91% (34)
- Pediatric Nursing ReviewDocument45 pagesPediatric Nursing Reviewɹǝʍdןnos98% (87)
- Nursing Jurisprudence ReviewDocument6 pagesNursing Jurisprudence Reviewɹǝʍdןnos96% (28)
- Practice Test Community Health Nursing Set: CDocument8 pagesPractice Test Community Health Nursing Set: CAngelica Kaye BuanNo ratings yet
- Doh Health Programs MaternalDocument82 pagesDoh Health Programs MaternalWilma Nierva Beralde100% (1)
- NDP HandoutsDocument2 pagesNDP Handoutscurly perkyNo ratings yet
- IMCI Orientation Powerpoint PresentationDocument45 pagesIMCI Orientation Powerpoint Presentationboynegro100% (18)
- Maternal & Child Care Nursing ReviewDocument37 pagesMaternal & Child Care Nursing Reviewɹǝʍdןnos98% (130)
- Field Health Services and Information System 1Document8 pagesField Health Services and Information System 1Vhince PiscoNo ratings yet
- IMCI AnswerDocument8 pagesIMCI AnswerQuia Benjch Uayan100% (4)
- Pedia 3.2 - IMCI (Vision) PDFDocument14 pagesPedia 3.2 - IMCI (Vision) PDFKaren ValdezNo ratings yet
- Epi PowerpointDocument29 pagesEpi PowerpointFelisa Lacsamana Gregorio100% (4)
- MCN Test BankDocument10 pagesMCN Test BankMho Pimentel Vanguardia100% (1)
- Exam FamilyDocument2 pagesExam FamilyJonaPhieDomingoMonteroIINo ratings yet
- IMCIDocument124 pagesIMCIRaquel Monsalve100% (1)
- Psychiatric Nursing ReviewDocument16 pagesPsychiatric Nursing Reviewɹǝʍdןnos97% (63)
- June 2009 Nurse Licensure Exam ResultDocument656 pagesJune 2009 Nurse Licensure Exam ResultRay Andrew del RosarioNo ratings yet
- Spring House NCLEX PN 755 Board Style Question TrainerDocument190 pagesSpring House NCLEX PN 755 Board Style Question Trainerɹǝʍdןnos100% (15)
- Module 7 - DOH ProgramDocument32 pagesModule 7 - DOH Programmirai desuNo ratings yet
- National Immunization Program: Manual of Procedures Booklet 4Document32 pagesNational Immunization Program: Manual of Procedures Booklet 4Blue Pielago100% (1)
- Department of Health Programs Related To Family HealthDocument62 pagesDepartment of Health Programs Related To Family HealthBea Bianca CruzNo ratings yet
- Mandatory Infants and Children Health Immunization Act of 2011 Compulsory ImmunizationDocument3 pagesMandatory Infants and Children Health Immunization Act of 2011 Compulsory Immunizationbunso padilla100% (2)
- Imci QuestionDocument21 pagesImci Questionmesdejen75% (12)
- Baguio Central University College of Nursing Comprehensive Exam.-ChnDocument9 pagesBaguio Central University College of Nursing Comprehensive Exam.-ChnKristian Karl Bautista Kiw-isNo ratings yet
- IMCIDocument27 pagesIMCImesdejen100% (6)
- MNCHN MopDocument68 pagesMNCHN Mopmbs_md100% (1)
- Handouts IMCIDocument5 pagesHandouts IMCIseigelystic100% (20)
- Doh Health Programs (Maternal)Document47 pagesDoh Health Programs (Maternal)Wilma Nierva Beralde100% (1)
- Nurse Deployment ProjectDocument6 pagesNurse Deployment ProjectAngel022150% (2)
- Maternal and Child NCLEX Questions Part2Document4 pagesMaternal and Child NCLEX Questions Part2Shengxy Ferrer50% (2)
- Doh Formula 1Document4 pagesDoh Formula 1HEALTH_AMBASSADORS75% (4)
- Ob Post TestDocument30 pagesOb Post TestSaybel Mediana0% (1)
- CHN Post TestDocument10 pagesCHN Post TestJune DumdumayaNo ratings yet
- CHNDocument49 pagesCHNAlbert Remollo Jr100% (2)
- Quiz Integrated Management of Childhood Illness Name: Date: Year & Section: ScoreDocument4 pagesQuiz Integrated Management of Childhood Illness Name: Date: Year & Section: ScoreSteve100% (2)
- CHN - ExamDocument7 pagesCHN - ExamAllyza Jane SartigaNo ratings yet
- CHN Post Test 1Document9 pagesCHN Post Test 1quidditch07No ratings yet
- IMCI Chart BookletDocument66 pagesIMCI Chart Bookletnorwin_033875No ratings yet
- The Field Health Service Information System (FHSIS)Document22 pagesThe Field Health Service Information System (FHSIS)i_love_quinn86% (56)
- Community Organizing Participatory Action Research (COPAR)Document22 pagesCommunity Organizing Participatory Action Research (COPAR)Evelyn F. Tadena100% (1)
- FHSISDocument20 pagesFHSISRosauro Cruz Briones100% (1)
- Essential Newborn Care: The DOH/WHO ProtocolDocument21 pagesEssential Newborn Care: The DOH/WHO ProtocolfelicitycherubNo ratings yet
- Pre TestDocument4 pagesPre TestEnzoNo ratings yet
- CA 2 - CHN Review 50 Items PretestDocument10 pagesCA 2 - CHN Review 50 Items PretestAlibasher Macalnas100% (1)
- IMCIDocument3 pagesIMCIwordlife360No ratings yet
- Pedia Post Test PDFDocument5 pagesPedia Post Test PDFBrian Montales BaggayanNo ratings yet
- IMCIDocument148 pagesIMCILloyd Rafael EstabilloNo ratings yet
- MNCHNDocument45 pagesMNCHNAnn Margareth Salazar-ManaloNo ratings yet
- Competency Appraisal Imci Set BDocument5 pagesCompetency Appraisal Imci Set BEden Marie FranciscoNo ratings yet
- Roles of Community Health NurseDocument12 pagesRoles of Community Health NurseEDz Delica SandovalNo ratings yet
- Practice Questions of CHNDocument41 pagesPractice Questions of CHNApril Gae TilacasNo ratings yet
- Exam RationalizationDocument73 pagesExam RationalizationPrince Jhessie L. AbellaNo ratings yet
- IMCI Sudan Chartbooklet 2017Document55 pagesIMCI Sudan Chartbooklet 2017zidabyNo ratings yet
- Integrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsDocument79 pagesIntegrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsAudrey C. JunsayNo ratings yet
- Integrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsDocument79 pagesIntegrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsGejehNo ratings yet
- Integrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsDocument78 pagesIntegrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsWendy EscalanteNo ratings yet
- CHART BOOKLET Integrated Management of Childhood IllnessDocument79 pagesCHART BOOKLET Integrated Management of Childhood Illnessbonjh0eNo ratings yet
- IMCI Chart 2014 EditionDocument80 pagesIMCI Chart 2014 EditionHarold DiasanaNo ratings yet
- IMNCIDocument84 pagesIMNCIAyenew100% (1)
- Imci BookletDocument79 pagesImci BookletLevi AckerManNo ratings yet
- ChartDocument75 pagesChartxalwoqaali2018No ratings yet
- IMNCI Chart Booklet Medical Officer 2023Document50 pagesIMNCI Chart Booklet Medical Officer 2023AbcNo ratings yet
- IMNCI Cahrtbooklet 2016-1Document82 pagesIMNCI Cahrtbooklet 2016-1AyenewNo ratings yet
- S3 - Under 2 MonthDocument45 pagesS3 - Under 2 MonthBelay GezahegnNo ratings yet
- Management of Sick Young Infant Aged 1 Week - 2 MonthsDocument2 pagesManagement of Sick Young Infant Aged 1 Week - 2 MonthsChielee Anne PayongayongNo ratings yet
- 06 - Summary Treatment Follow UpDocument15 pages06 - Summary Treatment Follow UpSweet Zhel NarretoNo ratings yet
- Performance of School July 2011 Nursing Board Exam ResultsDocument20 pagesPerformance of School July 2011 Nursing Board Exam ResultsjuancristoNo ratings yet
- July 2011 Nursing Board Exam Top 10 Successful ExamineesDocument2 pagesJuly 2011 Nursing Board Exam Top 10 Successful ExamineesPhilippineNursingDirectory.comNo ratings yet
- List of PassersDocument751 pagesList of PassersJeanhel AuditorNo ratings yet
- PINOYBSNJuly 2011 Nursing Board Exam Result Top Performing SchoolsDocument19 pagesPINOYBSNJuly 2011 Nursing Board Exam Result Top Performing Schoolspinoybsn1192No ratings yet
- Maternal & Child Care Nursing Table of ContentsDocument2 pagesMaternal & Child Care Nursing Table of Contentsɹǝʍdןnos100% (4)
- Nursing Practice 5 (Dec 2006)Document10 pagesNursing Practice 5 (Dec 2006)ɹǝʍdןnos50% (2)
- Munting Buhangin Beach Camp (Pricing Schedules 2011)Document2 pagesMunting Buhangin Beach Camp (Pricing Schedules 2011)ɹǝʍdןnos0% (1)
- Nursing Practice 4 (Dec 2006)Document11 pagesNursing Practice 4 (Dec 2006)ɹǝʍdןnosNo ratings yet
- Nursing Practice 3 (Dec 2006)Document11 pagesNursing Practice 3 (Dec 2006)ɹǝʍdןnosNo ratings yet
- Professional Adjustment in NursingDocument17 pagesProfessional Adjustment in Nursingɹǝʍdןnos100% (17)
- Nursing Practice 1 (Dec 2006)Document12 pagesNursing Practice 1 (Dec 2006)ɹǝʍdןnos100% (1)
- Set A: Community Health Nursing and Care of Mother and ChildDocument11 pagesSet A: Community Health Nursing and Care of Mother and ChildAldrin NavarroNo ratings yet
- Medical-Surgical Nursing Table of ContentsDocument2 pagesMedical-Surgical Nursing Table of Contentsɹǝʍdןnos0% (1)
- Surgical InstrumentsDocument8 pagesSurgical InstrumentsSharmaine Simon91% (11)
- Nursing ProcessDocument118 pagesNursing Processɹǝʍdןnos100% (30)
- PsychopharmacologyDocument31 pagesPsychopharmacologyɹǝʍdןnos100% (8)
- 50 Item Psychiatric Nursing Exam IDocument11 pages50 Item Psychiatric Nursing Exam Iɹǝʍdןnos98% (41)
- Indian Income Tax Return Acknowledgement: Name of Premises/Building/VillageDocument1 pageIndian Income Tax Return Acknowledgement: Name of Premises/Building/Villagehealth with wealthNo ratings yet
- Chapter 14 NotesDocument21 pagesChapter 14 NotesnightdazeNo ratings yet
- Guide For Applications of Life Insurance: Key For Associateship ExaminationDocument17 pagesGuide For Applications of Life Insurance: Key For Associateship ExaminationDebmalya DasNo ratings yet
- BH6 EngDocument99 pagesBH6 EngmnbvqwertNo ratings yet
- Wilhoit, Summary PDFDocument5 pagesWilhoit, Summary PDFJake SimonsNo ratings yet
- Technical Data: Protective Grease For Overhead Line ConductorsDocument3 pagesTechnical Data: Protective Grease For Overhead Line ConductorssreedharNo ratings yet
- Football g.9 s.2Document51 pagesFootball g.9 s.2apNo ratings yet
- Medicinal Plants MasterDocument490 pagesMedicinal Plants MasterNguyen Le Xuan BachNo ratings yet
- CESPL - Profile1Document93 pagesCESPL - Profile1Satvinder Deep SinghNo ratings yet
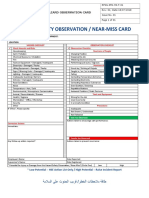
- RPSG-IMS-HS-F - 01 - Hazard Observation CardDocument2 pagesRPSG-IMS-HS-F - 01 - Hazard Observation CardRocky BisNo ratings yet
- SENEPOL1Document36 pagesSENEPOL1JuanNo ratings yet
- Chap 4 Section 3 Review Q&A'sDocument3 pagesChap 4 Section 3 Review Q&A'sAashi PatelNo ratings yet
- Operating, Maintenance & Parts Manual: Rated LoadsDocument48 pagesOperating, Maintenance & Parts Manual: Rated LoadsAmanNo ratings yet
- Statements of Financial Position As at 31 December 2009 and 2010Document3 pagesStatements of Financial Position As at 31 December 2009 and 2010mohitgaba19No ratings yet
- Rogalsky - The Working Poor and What GIS Reveals About The Possibilities of Public Transit PDFDocument12 pagesRogalsky - The Working Poor and What GIS Reveals About The Possibilities of Public Transit PDFMiaNo ratings yet
- Bulacan MTC: Notifiable Diseases Law Can't Be Used Against People Without Quarantine Pass, ButDocument7 pagesBulacan MTC: Notifiable Diseases Law Can't Be Used Against People Without Quarantine Pass, ButYNNA DERAYNo ratings yet
- Dufaycolor Book: Dufay-Chromex LimitedDocument60 pagesDufaycolor Book: Dufay-Chromex LimitedSergey PopovNo ratings yet
- WRITING NewDocument21 pagesWRITING Newtini cushingNo ratings yet
- A Preliminary Geo Seismological Report On Kashmir Earthquake of 8th Oct 2005Document13 pagesA Preliminary Geo Seismological Report On Kashmir Earthquake of 8th Oct 2005Abdul HafeezNo ratings yet
- Errata Sheet 1.7 - Dropzone Commander Official Update: NEW ADDITIONS/ CHANGES FROM VERSION 1.6 Highlighted in RedDocument2 pagesErrata Sheet 1.7 - Dropzone Commander Official Update: NEW ADDITIONS/ CHANGES FROM VERSION 1.6 Highlighted in RedTecnocastoroNo ratings yet
- Philippine National Philippine National Philippine National Philippine National Standard Standard Standard StandardDocument14 pagesPhilippine National Philippine National Philippine National Philippine National Standard Standard Standard StandardBernard Karlo BuduanNo ratings yet
- Prof Ed Final Drill EditedDocument13 pagesProf Ed Final Drill EditedChaoryl Ross EsperaNo ratings yet
- Computer EducationDocument4 pagesComputer Educationjonny talacayNo ratings yet
- Case 1Document2 pagesCase 1Wanda Marie SingletaryNo ratings yet
- Internal Motivation Infographics by SlidesgoDocument34 pagesInternal Motivation Infographics by Slidesgoyosua tafulyNo ratings yet
- Topic 6 - Part 2 - Week 4Document40 pagesTopic 6 - Part 2 - Week 4Teo Khim SiangNo ratings yet
- The National Policy On Education (1981) : Problems of Implementation and The Way ForwardDocument8 pagesThe National Policy On Education (1981) : Problems of Implementation and The Way ForwardSaidu abuNo ratings yet
- B. SC Nursing: Medical Surgical Nursing Unit V - Disorders of The Cardio Vascular SystemDocument31 pagesB. SC Nursing: Medical Surgical Nursing Unit V - Disorders of The Cardio Vascular SystemPoova Ragavan100% (1)
- Wedding Wedding Wedding Wedding WeddingDocument10 pagesWedding Wedding Wedding Wedding WeddingtharinduNo ratings yet






















































































































Download as pdf or txt
You might also like
- Nurse Deployment Program (NDP) Examination NotesDocument44 pagesNurse Deployment Program (NDP) Examination Notesdeeday echavez93% (27)
- Medical-Surgical Nursing ReviewDocument90 pagesMedical-Surgical Nursing Reviewɹǝʍdןnos99% (316)
- Pathognomonic SignsDocument3 pagesPathognomonic Signsɹǝʍdןnos100% (21)
- Community Health Nursing Examination Part IDocument17 pagesCommunity Health Nursing Examination Part Iɹǝʍdןnos97% (64)
- ABG InterpretationDocument31 pagesABG Interpretationɹǝʍdןnos100% (12)
- Nursing Research ReviewDocument13 pagesNursing Research Reviewɹǝʍdןnos96% (50)
- The 3D Printing Handbook - Technologies, Design and ApplicationsDocument347 pagesThe 3D Printing Handbook - Technologies, Design and ApplicationsJuan Bernardo Gallardo100% (7)
- Nursing Practice 1Document62 pagesNursing Practice 1ɹǝʍdןnos100% (2)
- NLE Compilation 1Document67 pagesNLE Compilation 1blazegomez91% (34)
- Pediatric Nursing ReviewDocument45 pagesPediatric Nursing Reviewɹǝʍdןnos98% (87)
- Nursing Jurisprudence ReviewDocument6 pagesNursing Jurisprudence Reviewɹǝʍdןnos96% (28)
- Practice Test Community Health Nursing Set: CDocument8 pagesPractice Test Community Health Nursing Set: CAngelica Kaye BuanNo ratings yet
- Doh Health Programs MaternalDocument82 pagesDoh Health Programs MaternalWilma Nierva Beralde100% (1)
- NDP HandoutsDocument2 pagesNDP Handoutscurly perkyNo ratings yet
- IMCI Orientation Powerpoint PresentationDocument45 pagesIMCI Orientation Powerpoint Presentationboynegro100% (18)
- Maternal & Child Care Nursing ReviewDocument37 pagesMaternal & Child Care Nursing Reviewɹǝʍdןnos98% (130)
- Field Health Services and Information System 1Document8 pagesField Health Services and Information System 1Vhince PiscoNo ratings yet
- IMCI AnswerDocument8 pagesIMCI AnswerQuia Benjch Uayan100% (4)
- Pedia 3.2 - IMCI (Vision) PDFDocument14 pagesPedia 3.2 - IMCI (Vision) PDFKaren ValdezNo ratings yet
- Epi PowerpointDocument29 pagesEpi PowerpointFelisa Lacsamana Gregorio100% (4)
- MCN Test BankDocument10 pagesMCN Test BankMho Pimentel Vanguardia100% (1)
- Exam FamilyDocument2 pagesExam FamilyJonaPhieDomingoMonteroIINo ratings yet
- IMCIDocument124 pagesIMCIRaquel Monsalve100% (1)
- Psychiatric Nursing ReviewDocument16 pagesPsychiatric Nursing Reviewɹǝʍdןnos97% (63)
- June 2009 Nurse Licensure Exam ResultDocument656 pagesJune 2009 Nurse Licensure Exam ResultRay Andrew del RosarioNo ratings yet
- Spring House NCLEX PN 755 Board Style Question TrainerDocument190 pagesSpring House NCLEX PN 755 Board Style Question Trainerɹǝʍdןnos100% (15)
- Module 7 - DOH ProgramDocument32 pagesModule 7 - DOH Programmirai desuNo ratings yet
- National Immunization Program: Manual of Procedures Booklet 4Document32 pagesNational Immunization Program: Manual of Procedures Booklet 4Blue Pielago100% (1)
- Department of Health Programs Related To Family HealthDocument62 pagesDepartment of Health Programs Related To Family HealthBea Bianca CruzNo ratings yet
- Mandatory Infants and Children Health Immunization Act of 2011 Compulsory ImmunizationDocument3 pagesMandatory Infants and Children Health Immunization Act of 2011 Compulsory Immunizationbunso padilla100% (2)
- Imci QuestionDocument21 pagesImci Questionmesdejen75% (12)
- Baguio Central University College of Nursing Comprehensive Exam.-ChnDocument9 pagesBaguio Central University College of Nursing Comprehensive Exam.-ChnKristian Karl Bautista Kiw-isNo ratings yet
- IMCIDocument27 pagesIMCImesdejen100% (6)
- MNCHN MopDocument68 pagesMNCHN Mopmbs_md100% (1)
- Handouts IMCIDocument5 pagesHandouts IMCIseigelystic100% (20)
- Doh Health Programs (Maternal)Document47 pagesDoh Health Programs (Maternal)Wilma Nierva Beralde100% (1)
- Nurse Deployment ProjectDocument6 pagesNurse Deployment ProjectAngel022150% (2)
- Maternal and Child NCLEX Questions Part2Document4 pagesMaternal and Child NCLEX Questions Part2Shengxy Ferrer50% (2)
- Doh Formula 1Document4 pagesDoh Formula 1HEALTH_AMBASSADORS75% (4)
- Ob Post TestDocument30 pagesOb Post TestSaybel Mediana0% (1)
- CHN Post TestDocument10 pagesCHN Post TestJune DumdumayaNo ratings yet
- CHNDocument49 pagesCHNAlbert Remollo Jr100% (2)
- Quiz Integrated Management of Childhood Illness Name: Date: Year & Section: ScoreDocument4 pagesQuiz Integrated Management of Childhood Illness Name: Date: Year & Section: ScoreSteve100% (2)
- CHN - ExamDocument7 pagesCHN - ExamAllyza Jane SartigaNo ratings yet
- CHN Post Test 1Document9 pagesCHN Post Test 1quidditch07No ratings yet
- IMCI Chart BookletDocument66 pagesIMCI Chart Bookletnorwin_033875No ratings yet
- The Field Health Service Information System (FHSIS)Document22 pagesThe Field Health Service Information System (FHSIS)i_love_quinn86% (56)
- Community Organizing Participatory Action Research (COPAR)Document22 pagesCommunity Organizing Participatory Action Research (COPAR)Evelyn F. Tadena100% (1)
- FHSISDocument20 pagesFHSISRosauro Cruz Briones100% (1)
- Essential Newborn Care: The DOH/WHO ProtocolDocument21 pagesEssential Newborn Care: The DOH/WHO ProtocolfelicitycherubNo ratings yet
- Pre TestDocument4 pagesPre TestEnzoNo ratings yet
- CA 2 - CHN Review 50 Items PretestDocument10 pagesCA 2 - CHN Review 50 Items PretestAlibasher Macalnas100% (1)
- IMCIDocument3 pagesIMCIwordlife360No ratings yet
- Pedia Post Test PDFDocument5 pagesPedia Post Test PDFBrian Montales BaggayanNo ratings yet
- IMCIDocument148 pagesIMCILloyd Rafael EstabilloNo ratings yet
- MNCHNDocument45 pagesMNCHNAnn Margareth Salazar-ManaloNo ratings yet
- Competency Appraisal Imci Set BDocument5 pagesCompetency Appraisal Imci Set BEden Marie FranciscoNo ratings yet
- Roles of Community Health NurseDocument12 pagesRoles of Community Health NurseEDz Delica SandovalNo ratings yet
- Practice Questions of CHNDocument41 pagesPractice Questions of CHNApril Gae TilacasNo ratings yet
- Exam RationalizationDocument73 pagesExam RationalizationPrince Jhessie L. AbellaNo ratings yet
- IMCI Sudan Chartbooklet 2017Document55 pagesIMCI Sudan Chartbooklet 2017zidabyNo ratings yet
- Integrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsDocument79 pagesIntegrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsAudrey C. JunsayNo ratings yet
- Integrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsDocument79 pagesIntegrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsGejehNo ratings yet
- Integrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsDocument78 pagesIntegrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsWendy EscalanteNo ratings yet
- CHART BOOKLET Integrated Management of Childhood IllnessDocument79 pagesCHART BOOKLET Integrated Management of Childhood Illnessbonjh0eNo ratings yet
- IMCI Chart 2014 EditionDocument80 pagesIMCI Chart 2014 EditionHarold DiasanaNo ratings yet
- IMNCIDocument84 pagesIMNCIAyenew100% (1)
- Imci BookletDocument79 pagesImci BookletLevi AckerManNo ratings yet
- ChartDocument75 pagesChartxalwoqaali2018No ratings yet
- IMNCI Chart Booklet Medical Officer 2023Document50 pagesIMNCI Chart Booklet Medical Officer 2023AbcNo ratings yet
- IMNCI Cahrtbooklet 2016-1Document82 pagesIMNCI Cahrtbooklet 2016-1AyenewNo ratings yet
- S3 - Under 2 MonthDocument45 pagesS3 - Under 2 MonthBelay GezahegnNo ratings yet
- Management of Sick Young Infant Aged 1 Week - 2 MonthsDocument2 pagesManagement of Sick Young Infant Aged 1 Week - 2 MonthsChielee Anne PayongayongNo ratings yet
- 06 - Summary Treatment Follow UpDocument15 pages06 - Summary Treatment Follow UpSweet Zhel NarretoNo ratings yet
- Performance of School July 2011 Nursing Board Exam ResultsDocument20 pagesPerformance of School July 2011 Nursing Board Exam ResultsjuancristoNo ratings yet
- July 2011 Nursing Board Exam Top 10 Successful ExamineesDocument2 pagesJuly 2011 Nursing Board Exam Top 10 Successful ExamineesPhilippineNursingDirectory.comNo ratings yet
- List of PassersDocument751 pagesList of PassersJeanhel AuditorNo ratings yet
- PINOYBSNJuly 2011 Nursing Board Exam Result Top Performing SchoolsDocument19 pagesPINOYBSNJuly 2011 Nursing Board Exam Result Top Performing Schoolspinoybsn1192No ratings yet
- Maternal & Child Care Nursing Table of ContentsDocument2 pagesMaternal & Child Care Nursing Table of Contentsɹǝʍdןnos100% (4)
- Nursing Practice 5 (Dec 2006)Document10 pagesNursing Practice 5 (Dec 2006)ɹǝʍdןnos50% (2)
- Munting Buhangin Beach Camp (Pricing Schedules 2011)Document2 pagesMunting Buhangin Beach Camp (Pricing Schedules 2011)ɹǝʍdןnos0% (1)
- Nursing Practice 4 (Dec 2006)Document11 pagesNursing Practice 4 (Dec 2006)ɹǝʍdןnosNo ratings yet
- Nursing Practice 3 (Dec 2006)Document11 pagesNursing Practice 3 (Dec 2006)ɹǝʍdןnosNo ratings yet
- Professional Adjustment in NursingDocument17 pagesProfessional Adjustment in Nursingɹǝʍdןnos100% (17)
- Nursing Practice 1 (Dec 2006)Document12 pagesNursing Practice 1 (Dec 2006)ɹǝʍdןnos100% (1)
- Set A: Community Health Nursing and Care of Mother and ChildDocument11 pagesSet A: Community Health Nursing and Care of Mother and ChildAldrin NavarroNo ratings yet
- Medical-Surgical Nursing Table of ContentsDocument2 pagesMedical-Surgical Nursing Table of Contentsɹǝʍdןnos0% (1)
- Surgical InstrumentsDocument8 pagesSurgical InstrumentsSharmaine Simon91% (11)
- Nursing ProcessDocument118 pagesNursing Processɹǝʍdןnos100% (30)
- PsychopharmacologyDocument31 pagesPsychopharmacologyɹǝʍdןnos100% (8)
- 50 Item Psychiatric Nursing Exam IDocument11 pages50 Item Psychiatric Nursing Exam Iɹǝʍdןnos98% (41)
- Indian Income Tax Return Acknowledgement: Name of Premises/Building/VillageDocument1 pageIndian Income Tax Return Acknowledgement: Name of Premises/Building/Villagehealth with wealthNo ratings yet
- Chapter 14 NotesDocument21 pagesChapter 14 NotesnightdazeNo ratings yet
- Guide For Applications of Life Insurance: Key For Associateship ExaminationDocument17 pagesGuide For Applications of Life Insurance: Key For Associateship ExaminationDebmalya DasNo ratings yet
- BH6 EngDocument99 pagesBH6 EngmnbvqwertNo ratings yet
- Wilhoit, Summary PDFDocument5 pagesWilhoit, Summary PDFJake SimonsNo ratings yet
- Technical Data: Protective Grease For Overhead Line ConductorsDocument3 pagesTechnical Data: Protective Grease For Overhead Line ConductorssreedharNo ratings yet
- Football g.9 s.2Document51 pagesFootball g.9 s.2apNo ratings yet
- Medicinal Plants MasterDocument490 pagesMedicinal Plants MasterNguyen Le Xuan BachNo ratings yet
- CESPL - Profile1Document93 pagesCESPL - Profile1Satvinder Deep SinghNo ratings yet
- RPSG-IMS-HS-F - 01 - Hazard Observation CardDocument2 pagesRPSG-IMS-HS-F - 01 - Hazard Observation CardRocky BisNo ratings yet
- SENEPOL1Document36 pagesSENEPOL1JuanNo ratings yet
- Chap 4 Section 3 Review Q&A'sDocument3 pagesChap 4 Section 3 Review Q&A'sAashi PatelNo ratings yet
- Operating, Maintenance & Parts Manual: Rated LoadsDocument48 pagesOperating, Maintenance & Parts Manual: Rated LoadsAmanNo ratings yet
- Statements of Financial Position As at 31 December 2009 and 2010Document3 pagesStatements of Financial Position As at 31 December 2009 and 2010mohitgaba19No ratings yet
- Rogalsky - The Working Poor and What GIS Reveals About The Possibilities of Public Transit PDFDocument12 pagesRogalsky - The Working Poor and What GIS Reveals About The Possibilities of Public Transit PDFMiaNo ratings yet
- Bulacan MTC: Notifiable Diseases Law Can't Be Used Against People Without Quarantine Pass, ButDocument7 pagesBulacan MTC: Notifiable Diseases Law Can't Be Used Against People Without Quarantine Pass, ButYNNA DERAYNo ratings yet
- Dufaycolor Book: Dufay-Chromex LimitedDocument60 pagesDufaycolor Book: Dufay-Chromex LimitedSergey PopovNo ratings yet
- WRITING NewDocument21 pagesWRITING Newtini cushingNo ratings yet
- A Preliminary Geo Seismological Report On Kashmir Earthquake of 8th Oct 2005Document13 pagesA Preliminary Geo Seismological Report On Kashmir Earthquake of 8th Oct 2005Abdul HafeezNo ratings yet
- Errata Sheet 1.7 - Dropzone Commander Official Update: NEW ADDITIONS/ CHANGES FROM VERSION 1.6 Highlighted in RedDocument2 pagesErrata Sheet 1.7 - Dropzone Commander Official Update: NEW ADDITIONS/ CHANGES FROM VERSION 1.6 Highlighted in RedTecnocastoroNo ratings yet
- Philippine National Philippine National Philippine National Philippine National Standard Standard Standard StandardDocument14 pagesPhilippine National Philippine National Philippine National Philippine National Standard Standard Standard StandardBernard Karlo BuduanNo ratings yet
- Prof Ed Final Drill EditedDocument13 pagesProf Ed Final Drill EditedChaoryl Ross EsperaNo ratings yet
- Computer EducationDocument4 pagesComputer Educationjonny talacayNo ratings yet
- Case 1Document2 pagesCase 1Wanda Marie SingletaryNo ratings yet
- Internal Motivation Infographics by SlidesgoDocument34 pagesInternal Motivation Infographics by Slidesgoyosua tafulyNo ratings yet
- Topic 6 - Part 2 - Week 4Document40 pagesTopic 6 - Part 2 - Week 4Teo Khim SiangNo ratings yet
- The National Policy On Education (1981) : Problems of Implementation and The Way ForwardDocument8 pagesThe National Policy On Education (1981) : Problems of Implementation and The Way ForwardSaidu abuNo ratings yet
- B. SC Nursing: Medical Surgical Nursing Unit V - Disorders of The Cardio Vascular SystemDocument31 pagesB. SC Nursing: Medical Surgical Nursing Unit V - Disorders of The Cardio Vascular SystemPoova Ragavan100% (1)
- Wedding Wedding Wedding Wedding WeddingDocument10 pagesWedding Wedding Wedding Wedding WeddingtharinduNo ratings yet