Download as doc, pdf, or txt
You might also like
- Drug Discovery and DevelopmentDocument341 pagesDrug Discovery and DevelopmentJosa Camille Bungay100% (1)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- List of Importers of Medicines/Pharmaceuticals in Addis AbabaDocument4 pagesList of Importers of Medicines/Pharmaceuticals in Addis AbabaCE CERTIFICATE67% (3)
- EthicsDocument16 pagesEthicsjennessvillanuevaNo ratings yet
- Chemistry of Opioids JakiDocument3 pagesChemistry of Opioids Jakidrugdrug0% (1)
- Chapter 8 - Individual Variation in Drug ResponsesDocument3 pagesChapter 8 - Individual Variation in Drug Responsesdlneisha61100% (3)
- Chapter 5 - PharmacodynamicsDocument7 pagesChapter 5 - Pharmacodynamicsdlneisha61100% (1)
- Chapter 10 - Drug Therapy in PediatricsDocument4 pagesChapter 10 - Drug Therapy in Pediatricsdlneisha61No ratings yet
- Chapter 1 - Orientation To PharmacologyDocument4 pagesChapter 1 - Orientation To Pharmacologydlneisha61No ratings yet
- Trend 2Document24 pagesTrend 2TUTIK SISWATINo ratings yet
- Top 21 Pharmacist Interview QuestionsDocument4 pagesTop 21 Pharmacist Interview QuestionsRaluca Maria DragomirNo ratings yet
- Suppositories Phardose LectureDocument41 pagesSuppositories Phardose LecturePeter Paul RecaboNo ratings yet
- Aseptic Techniques (Free One)Document39 pagesAseptic Techniques (Free One)api-19641337No ratings yet
- Perioperative Nursing Care 1Document17 pagesPerioperative Nursing Care 1Ardi CrisnaNo ratings yet
- SuppositoriesDocument21 pagesSuppositoriesMyzhel InumerableNo ratings yet
- Ilegal DrugsDocument40 pagesIlegal DrugsCabagan IsabelaNo ratings yet
- Nupc 113 Module IDocument110 pagesNupc 113 Module IAthena PasabingNo ratings yet
- Application of Pharmacology in NursingDocument7 pagesApplication of Pharmacology in Nursingrlinao100% (1)
- Aseptic TechniquesDocument6 pagesAseptic TechniquesAinun MokhtarNo ratings yet
- Einc Lecture Notes Module 2Document5 pagesEinc Lecture Notes Module 2fallen100% (1)
- National Medical PolicyDocument11 pagesNational Medical PolicySyifa MunawarahNo ratings yet
- Concepts in Community Development 2021Document24 pagesConcepts in Community Development 2021Given MsombaNo ratings yet
- Nursing Code of EthicsDocument28 pagesNursing Code of EthicsHans TrishaNo ratings yet
- Pharmacology ReviewerDocument14 pagesPharmacology ReviewerJacqueline Mañago CalaycayNo ratings yet
- Career Planning: Beginning A Job Search, Sources of Job Leads, Developing A ResumeDocument26 pagesCareer Planning: Beginning A Job Search, Sources of Job Leads, Developing A ResumeJustine May GervacioNo ratings yet
- Legal Foundations of Nursing EducationDocument9 pagesLegal Foundations of Nursing EducationtruebluepawNo ratings yet
- Community Health NursingDocument93 pagesCommunity Health NursingKristaMaeC.LazoNo ratings yet
- Nursing As A Profession: Dr. Thelma C. de Mesa RN, Man, Usrn, PHDDocument126 pagesNursing As A Profession: Dr. Thelma C. de Mesa RN, Man, Usrn, PHDChristian Clyde Noel JakosalemNo ratings yet
- Healthcare EthicsDocument6 pagesHealthcare EthicsBagsit Angelique Khryztelle G.No ratings yet
- Aquino vs. Heirs of Raymunda CalayagDocument4 pagesAquino vs. Heirs of Raymunda CalayagJenny ButacanNo ratings yet
- Staff Development in NursingDocument52 pagesStaff Development in NursingMaricris Tac-an Calising-PallarNo ratings yet
- Nurse As EducatorDocument28 pagesNurse As Educatornaelnael chaaNo ratings yet
- 2019 IMCI A4 Book FinalDocument80 pages2019 IMCI A4 Book Finalkeyden adoNo ratings yet
- A Project Proposal On Case Study and Management of A Type 1 Diabetes Mellitus ClientDocument6 pagesA Project Proposal On Case Study and Management of A Type 1 Diabetes Mellitus ClientMichael Kivumbi100% (3)
- Drug Therapy Considerations Across The LifespanDocument43 pagesDrug Therapy Considerations Across The LifespanhealingnurseNo ratings yet
- Strategies of Health Education: Mr. Jhessie L. Abella, RN, RM, MANDocument178 pagesStrategies of Health Education: Mr. Jhessie L. Abella, RN, RM, MANPrince Jhessie L. Abella100% (1)
- Health Assessment 1.0Document11 pagesHealth Assessment 1.0Nathalie CaracaNo ratings yet
- Suppository, Insert & StickDocument3 pagesSuppository, Insert & StickCorina Faye RosarioNo ratings yet
- Imci UpdatesDocument37 pagesImci UpdateskristiandiorcapiliNo ratings yet
- WHO Surgical Safety ChecklistDocument1 pageWHO Surgical Safety ChecklistneculavNo ratings yet
- NCM 106 IntroductionDocument126 pagesNCM 106 IntroductionYra JhaneNo ratings yet
- 2022 MEDICATION ERROR Without ReferenceDocument133 pages2022 MEDICATION ERROR Without ReferenceSuhaime UEMNo ratings yet
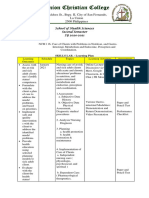
- Widdoes ST., Brgy. II, City of San Fernando, La Union 2500 PhilippinesDocument7 pagesWiddoes ST., Brgy. II, City of San Fernando, La Union 2500 Philippinesricky torresNo ratings yet
- Elective I: Hospice Palliative CareDocument3 pagesElective I: Hospice Palliative Carelemuel_que50% (2)
- Graduate School of NursingDocument11 pagesGraduate School of NursingpwunewsNo ratings yet
- Professional Development PlanDocument17 pagesProfessional Development Planapi-235633705100% (1)
- B. Maternal and Child Health Goals and StandardsDocument13 pagesB. Maternal and Child Health Goals and StandardsJayp TupasNo ratings yet
- NCM107 PlanningDocument59 pagesNCM107 Planningebtg_f100% (1)
- Medication FlashcardsDocument10 pagesMedication FlashcardsSilvio PerezNo ratings yet
- College: Program: Course Code: Credits: Class Days: Room: InstructorDocument9 pagesCollege: Program: Course Code: Credits: Class Days: Room: InstructorFranco RazonNo ratings yet
- Cmo 27 98Document3 pagesCmo 27 98Jemai O. Bico ÜNo ratings yet
- Principles of Surgical Asepsis: Rationale: Microorganisms TravelDocument13 pagesPrinciples of Surgical Asepsis: Rationale: Microorganisms TravelCharina Aubrey RiodilNo ratings yet
- Common Medical AbbreviationsDocument1 pageCommon Medical Abbreviationskedwards108No ratings yet
- Chapter 7 - Adverse Drug Reaction and Medication ErrorsDocument6 pagesChapter 7 - Adverse Drug Reaction and Medication Errorsdlneisha61No ratings yet
- NCM 103 SyllabusDocument10 pagesNCM 103 SyllabuslouradelNo ratings yet
- The Role of Nurse As Educator: - Remedios H. Fernando, RN MANDocument23 pagesThe Role of Nurse As Educator: - Remedios H. Fernando, RN MANfleur harrisonNo ratings yet
- Wcms 316218 PDFDocument446 pagesWcms 316218 PDFRosemarieFigueroa100% (2)
- Health Education TransDocument10 pagesHealth Education TransPia Gabrielle Cabatana100% (1)
- Test Drills TwoDocument15 pagesTest Drills TwoSeanmarie CabralesNo ratings yet
- NCM 102 Health EducationDocument13 pagesNCM 102 Health EducationMargarette AfanNo ratings yet
- Inshare: C Hapter 11D Rug T Herapy in G Eriatric P AtientsDocument6 pagesInshare: C Hapter 11D Rug T Herapy in G Eriatric P AtientsHakim KhiljiNo ratings yet
- Outline Drug Therapy in Older AdultsDocument4 pagesOutline Drug Therapy in Older Adultsswillis1No ratings yet
- Amien GPP 6 MedDocument25 pagesAmien GPP 6 MedAmanuel MaruNo ratings yet
- PLB 1 B 8 Rianti NovalianaDocument21 pagesPLB 1 B 8 Rianti NovalianavikaseptideyaniNo ratings yet
- Human Immunodeficiency Virus: Transmission of HIVDocument15 pagesHuman Immunodeficiency Virus: Transmission of HIVdlneisha61No ratings yet
- Nursing 304 Nursing Care of The Client/Family With Select Sensory Health DeviationsDocument8 pagesNursing 304 Nursing Care of The Client/Family With Select Sensory Health Deviationsdlneisha61No ratings yet
- Impaired Skin Integrity and ConstipationDocument6 pagesImpaired Skin Integrity and Constipationdlneisha61100% (1)
- Mental Health Outline1Document25 pagesMental Health Outline1dlneisha61No ratings yet
- Nursing 304 Nursing Care of The Client/Family With Select Sensory Health DeviationsDocument8 pagesNursing 304 Nursing Care of The Client/Family With Select Sensory Health Deviationsdlneisha61No ratings yet
- Hiv Study GuideDocument3 pagesHiv Study Guidedlneisha61No ratings yet
- Mental Health NursingDocument10 pagesMental Health Nursingdlneisha61100% (4)
- Mental Health AssessmentDocument12 pagesMental Health Assessmentdlneisha61100% (4)
- Sexual Contact (Anal, Vaginal, Oral) With An HIV-infected PartnerDocument17 pagesSexual Contact (Anal, Vaginal, Oral) With An HIV-infected Partnerdlneisha61No ratings yet
- Hematology Outline For Blackboard Revised CDocument22 pagesHematology Outline For Blackboard Revised Cdlneisha61No ratings yet
- GU Blackboard OutlineDocument15 pagesGU Blackboard Outlinedlneisha61No ratings yet
- Diabetes Mellitus Outline For BBDocument10 pagesDiabetes Mellitus Outline For BBdlneisha61No ratings yet
- GU Lisa RetypedDocument15 pagesGU Lisa Retypeddlneisha61No ratings yet
- Hematology Outline For Blackboard Revised CDocument22 pagesHematology Outline For Blackboard Revised Cdlneisha61No ratings yet
- Concepts, Constructs, Variables and TheoryDocument6 pagesConcepts, Constructs, Variables and Theorydlneisha61100% (2)
- Urinary System: TH RDDocument13 pagesUrinary System: TH RDdlneisha61No ratings yet
- Dosage Practice Problem GuideDocument20 pagesDosage Practice Problem Guidedlneisha6171% (7)
- Fluids and Electrolytes Lesson Outline For BBDocument14 pagesFluids and Electrolytes Lesson Outline For BBdlneisha61100% (1)
- Mental Health NursingDocument10 pagesMental Health Nursingdlneisha61100% (4)
- Poison Prevention Packaging Act Guide For Healthcare ProfessionalsDocument23 pagesPoison Prevention Packaging Act Guide For Healthcare ProfessionalsNasru DiinNo ratings yet
- Liquid Dosage Forms-76382Document14 pagesLiquid Dosage Forms-76382Ilie GlаvanNo ratings yet
- Canadian Drug Names: Appendix EDocument9 pagesCanadian Drug Names: Appendix EEmmanuel GaliciaNo ratings yet
- Active Metabolites As Antidepressant Drugs: The Role of Norquetiapine in The Mechanism of Action of Quetiapine in The Treatment of Mood DisordersDocument8 pagesActive Metabolites As Antidepressant Drugs: The Role of Norquetiapine in The Mechanism of Action of Quetiapine in The Treatment of Mood DisordersNath miaounNo ratings yet
- Analgesics Presentation-1Document36 pagesAnalgesics Presentation-1Tatenda SibandaNo ratings yet
- Notes File - MergedDocument99 pagesNotes File - MergedMian. Shoaib.No ratings yet
- The Relation Between The Blood Benzodiazepine Concentration and Performance in Suspected Impaired DriversDocument6 pagesThe Relation Between The Blood Benzodiazepine Concentration and Performance in Suspected Impaired DriversBurca LarisaNo ratings yet
- 10 1136@vr 147 25 709Document5 pages10 1136@vr 147 25 709Erick ManosalvasNo ratings yet
- International Business Assignment Indian Companies Going GlobalDocument25 pagesInternational Business Assignment Indian Companies Going GlobalRony MaxNo ratings yet
- Pupuk PT SSA PDFDocument2 pagesPupuk PT SSA PDFNurul HardiyantiNo ratings yet
- Calculations in Toxicology and Determination of Median Effective and Median Lethal DosesDocument3 pagesCalculations in Toxicology and Determination of Median Effective and Median Lethal DosesHammad KingNo ratings yet
- 23 Perhitungan Farmakokinetika KlinikDocument3 pages23 Perhitungan Farmakokinetika KlinikMila Dwi Putri UtamiNo ratings yet
- Analgesics and Pain Control in DentistryDocument51 pagesAnalgesics and Pain Control in DentistryIyad Abou-Rabii0% (1)
- Design, Development and in Vitro Evaluation of Transdermal Patches Containing Domperidone MaleateDocument8 pagesDesign, Development and in Vitro Evaluation of Transdermal Patches Containing Domperidone MaleateIrfan N KhanNo ratings yet
- Stenorol® Crypto - OS - Brochure - EN - v01 - 1020Document2 pagesStenorol® Crypto - OS - Brochure - EN - v01 - 1020DrivailaNo ratings yet
- Antibiotics PDFDocument4 pagesAntibiotics PDFNilamdeen Mohamed ZamilNo ratings yet
- Match The Following. (Each 1 Mark) : A' B' (Feb, 2018)Document3 pagesMatch The Following. (Each 1 Mark) : A' B' (Feb, 2018)bettykoshyNo ratings yet
- 10.dissolution Comparison As Per IpbpuspepDocument5 pages10.dissolution Comparison As Per IpbpuspepNitinPrachiJainNo ratings yet
- Assessment Report On Valeriana Officinalis L., Radix andDocument67 pagesAssessment Report On Valeriana Officinalis L., Radix andAleks JosifovNo ratings yet
- Group-23 V.L.D.A.Document3 pagesGroup-23 V.L.D.A.Sahil KunduNo ratings yet
- Py 18Document9 pagesPy 18uvesh shaikhNo ratings yet
- Tamiflu PrescribingDocument26 pagesTamiflu PrescribingStacey WoodsNo ratings yet
- 2020 ImpactFactorsDocument28 pages2020 ImpactFactorsKondreddy Nageswara ReddyNo ratings yet
- No Nama Obat Ven Sediaan Harga SatuanjumlahDocument2 pagesNo Nama Obat Ven Sediaan Harga SatuanjumlahCINDYAH ANASTASIA CLARITANo ratings yet
- Obat-Obat AntiboitikDocument5 pagesObat-Obat AntiboitikAbdul ChristopherNo ratings yet
- DapusDocument3 pagesDapusWina Laili MNo ratings yet
- Pharma Past PaperDocument11 pagesPharma Past PaperMasood MughalNo ratings yet