Download as ppt, pdf, or txt
You might also like
- PATHO LEC WBC Lymph Nodes Spleen Thymus Part1 CompressedDocument84 pagesPATHO LEC WBC Lymph Nodes Spleen Thymus Part1 CompressedAngelo HinonNo ratings yet
- Intersex/ambiguous GenitaliaDocument22 pagesIntersex/ambiguous GenitalianoviNo ratings yet
- Acute Lymphoblastic LeukemiaDocument22 pagesAcute Lymphoblastic Leukemiaحسن محمدNo ratings yet
- Leukemia in ChildrenDocument44 pagesLeukemia in ChildrenSami ShouraNo ratings yet
- Acute Lymphoblastic LeukemiaDocument34 pagesAcute Lymphoblastic LeukemiamtyboyNo ratings yet
- Acute Lymphoblastic Leukemia: Muhammad Fadhel 1410311044Document21 pagesAcute Lymphoblastic Leukemia: Muhammad Fadhel 1410311044Alvin ArifNo ratings yet
- HaematologyDocument25 pagesHaematologyMenziPhiwokuhleSukatiNo ratings yet
- Acute Lymphoblastic LeukemiaDocument9 pagesAcute Lymphoblastic LeukemiaAdamant Al Johani Gangis100% (1)
- Adult Acute Lymphoblastic Leukemia: Concepts and StrategiesDocument12 pagesAdult Acute Lymphoblastic Leukemia: Concepts and StrategiesdrravesNo ratings yet
- Acute Lymphoblastic LeukemiaDocument19 pagesAcute Lymphoblastic LeukemiaNeng AyuRati50% (2)
- Acute Lymphoblastic Leukemia: Differential DiagnosisDocument6 pagesAcute Lymphoblastic Leukemia: Differential DiagnosisIma OhwNo ratings yet
- Acute Lymphoblastic LeukemiaDocument5 pagesAcute Lymphoblastic LeukemiavnykumalasariNo ratings yet
- All Aml NCCN 2023 HamidahDocument45 pagesAll Aml NCCN 2023 HamidahPPDS IPD ULMNo ratings yet
- Histiocytic Disorders Diagnosis and Treatment: Resident Education Lecture SeriesDocument41 pagesHistiocytic Disorders Diagnosis and Treatment: Resident Education Lecture SeriesChetan SekhriNo ratings yet
- Pediatric Acute Lymphoblastic LeukemiaDocument9 pagesPediatric Acute Lymphoblastic LeukemiaAlvin PratamaNo ratings yet
- Module 13.3 CA in ChildrenDocument27 pagesModule 13.3 CA in ChildrenkirstenNo ratings yet
- Acute Myelogenous Leukemia-Aml Acute Lymphoblastic Leukemia - AllDocument64 pagesAcute Myelogenous Leukemia-Aml Acute Lymphoblastic Leukemia - AllSiraj ShiferawNo ratings yet
- Background: Pediatric Acute Lymphoblastic LeukemiaDocument3 pagesBackground: Pediatric Acute Lymphoblastic LeukemiaNitin KumarNo ratings yet
- Acute Lymphoblastic Leukemia - LecturioDocument17 pagesAcute Lymphoblastic Leukemia - LecturioCornel PopaNo ratings yet
- Who Diagnostic Criteria MyelofibrosisDocument2 pagesWho Diagnostic Criteria MyelofibrosisaymenNo ratings yet
- Case StudyDocument10 pagesCase Studysabrown109No ratings yet
- غير معروف Chronic Leukemia-8 (Muhadharaty)Document60 pagesغير معروف Chronic Leukemia-8 (Muhadharaty)aliabumrfghNo ratings yet
- MCD 2015 and 2016Document6 pagesMCD 2015 and 2016Jenny LowsleyNo ratings yet
- AML, CML, ALL, CLL, HemophiliaDocument7 pagesAML, CML, ALL, CLL, HemophiliaJamara Kyla Dela CruzNo ratings yet
- Leukemia: Defintion: Leukemias Are Diseases in Which Localised or Generalised Proliferation orDocument12 pagesLeukemia: Defintion: Leukemias Are Diseases in Which Localised or Generalised Proliferation orsharon victoria mendezNo ratings yet
- Leukemia: Nyoto Widyo Astoro Hematologi Onkologi Medik RsgsDocument17 pagesLeukemia: Nyoto Widyo Astoro Hematologi Onkologi Medik RsgsNamun Sibora BoraNo ratings yet
- Cancers 12 01746Document18 pagesCancers 12 01746LauraQuinteroNo ratings yet
- Cancers 12 01746 v2Document18 pagesCancers 12 01746 v2Ulicer CruzNo ratings yet
- Tutorial: Section A: Multiple Choice Question (Mcqs T/F)Document7 pagesTutorial: Section A: Multiple Choice Question (Mcqs T/F)Harith AsriNo ratings yet
- Lymphoma: 2011-2012 Prof - Dr.Rejin Kebudi, M.DDocument57 pagesLymphoma: 2011-2012 Prof - Dr.Rejin Kebudi, M.Dmia rachmiNo ratings yet
- 2010 Childhood LeukaemiaDocument64 pages2010 Childhood LeukaemiaAnastasiafynnNo ratings yet
- Ratheesh R.LDocument42 pagesRatheesh R.LY. Beatrice AbigailNo ratings yet
- 09 Kleebsabai - Acute LeukemiaDocument36 pages09 Kleebsabai - Acute Leukemiadeirdre o'sullivanNo ratings yet
- Childhood Burkitt Lymphoma: Sabbas MDDocument35 pagesChildhood Burkitt Lymphoma: Sabbas MDLegend OMSUNo ratings yet
- Leukemia'S: DR H AlmukharraqDocument15 pagesLeukemia'S: DR H AlmukharraqUm HamoOdNo ratings yet
- Leukemia Pada AnakDocument33 pagesLeukemia Pada AnakandrianNo ratings yet
- Acute Lymphoblastic Leukemia (ALL) Is A Form ofDocument9 pagesAcute Lymphoblastic Leukemia (ALL) Is A Form ofPoohlarica UyNo ratings yet
- OnkologieDocument41 pagesOnkologieNatz BatzNo ratings yet
- Acute Leukemia - Knowledge at AMBOSSDocument1 pageAcute Leukemia - Knowledge at AMBOSSRenad AlharbiNo ratings yet
- Acute LeukemiaDocument6 pagesAcute LeukemiaYolanda UriolNo ratings yet
- 1.chapter I. Introduction (Abcd)Document11 pages1.chapter I. Introduction (Abcd)kualamonkeyNo ratings yet
- Neonatal PresenatestionDocument32 pagesNeonatal PresenatestionMerwan KemalNo ratings yet
- Acute Leukaemia Presentation 1Document20 pagesAcute Leukaemia Presentation 1Vaibhav KrishnaNo ratings yet
- Myeloproliferative Disorders (Bhs Inggris)Document57 pagesMyeloproliferative Disorders (Bhs Inggris)Denny DedenNo ratings yet
- Leucemia GenomicaDocument14 pagesLeucemia GenomicaNathalie Soler BarreraNo ratings yet
- CPP 2017 - HEM - Myeloid Neoplasms - LarsonDocument10 pagesCPP 2017 - HEM - Myeloid Neoplasms - Larsonjtzhang208No ratings yet
- Acute Leukemia: DR Rosline Hassan Hematology Department School of Medical Sciences USMDocument52 pagesAcute Leukemia: DR Rosline Hassan Hematology Department School of Medical Sciences USMJamilNo ratings yet
- Disorders of The Wihte CellsDocument22 pagesDisorders of The Wihte CellsdoniNo ratings yet
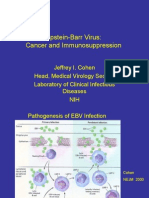
- Epstein-Barr Virus: Cancer and ImmunosuppressionDocument31 pagesEpstein-Barr Virus: Cancer and ImmunosuppressionMoisés SantosNo ratings yet
- Pediatric LeukemiasDocument42 pagesPediatric LeukemiasFilbertaNo ratings yet
- Psu 50318Document4 pagesPsu 50318Dr Venkatachalapathy T S Ped SurgeonNo ratings yet
- Acute and Chronic Leukemia FinalDocument68 pagesAcute and Chronic Leukemia FinalHannah LeiNo ratings yet
- Acute Leukaemia-Update: DR Niranjan N. RathodDocument89 pagesAcute Leukaemia-Update: DR Niranjan N. RathodratanNo ratings yet
- Acute Lymphoblastic LeukemiaDocument80 pagesAcute Lymphoblastic LeukemiaGizo YitayewNo ratings yet
- Transient Myeloproliferative Disorder: What's Eosinophilia Got To Do With It?Document1 pageTransient Myeloproliferative Disorder: What's Eosinophilia Got To Do With It?wadeschulzNo ratings yet
- Ajh 25303Document11 pagesAjh 25303RaffaharianggaraNo ratings yet
- Chronic Myeloid LeukemiaDocument37 pagesChronic Myeloid LeukemialoveNo ratings yet
- AmlDocument29 pagesAmlSari HestiyariniNo ratings yet