
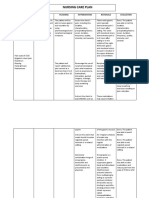
Upper Gastrointestinal - Esophageal Bleeding
Upper Gastrointestinal - Esophageal Bleeding
You might also like
- Nursing Care Plan 6 Impaired Gas ExchangeDocument9 pagesNursing Care Plan 6 Impaired Gas Exchangedbryant0101100% (12)
- Nursing Care Plan: Risk For Disuse SyndromeDocument2 pagesNursing Care Plan: Risk For Disuse SyndromeRozsy FakhrurNo ratings yet
- Nursing Care Plans For Acute ConfusionDocument3 pagesNursing Care Plans For Acute Confusionynecesity75% (4)
- The Back Book PDFDocument14 pagesThe Back Book PDFfoldsnholdsNo ratings yet
- Acute Intermittent Porphyria. General Aspects With Focus On PainDocument8 pagesAcute Intermittent Porphyria. General Aspects With Focus On PainAugusto Espada AraozNo ratings yet
- PBL 1Document7 pagesPBL 1Skyla Fiesta100% (1)
- Risk For InfectionDocument18 pagesRisk For InfectionValiant Baybay0% (1)
- Hypothyroidism Nursing Care PlanDocument2 pagesHypothyroidism Nursing Care Planmrhammer1957100% (2)
- Case Study On Fluid OverloadDocument37 pagesCase Study On Fluid OverloadradicalmpNo ratings yet
- Colon Rectal CancerDocument6 pagesColon Rectal Cancerbryantmaroney811No ratings yet
- ThrombophlebitisDocument10 pagesThrombophlebitismardsz100% (3)
- Sickle Cell CrisisDocument16 pagesSickle Cell Crisismardsz83% (12)
- NCP: Chronic Renal FailureDocument14 pagesNCP: Chronic Renal FailureJavie77% (13)
- Neck Pain Disability Index QuestionnaireDocument2 pagesNeck Pain Disability Index QuestionnaireLiliana Andrei Toader100% (1)
- Stoddard - Osteopathic-Technique PDFDocument271 pagesStoddard - Osteopathic-Technique PDFmitroisergiuNo ratings yet
- Nursing Care Plan For AIDS HIVDocument3 pagesNursing Care Plan For AIDS HIVFARAH MAE MEDINA100% (2)
- Impaired Electrolytes NCPDocument2 pagesImpaired Electrolytes NCPNora BacolNo ratings yet
- NCP Crohn'sDocument2 pagesNCP Crohn'sJanice Marco100% (1)
- NCP Copd4Document15 pagesNCP Copd4Alessa Marie Crisostomo Salazar100% (1)
- Massive AscitesDocument12 pagesMassive Ascitesranitidin100% (1)
- Urinary Tract Infection, (UTI) Is An Infection of One orDocument4 pagesUrinary Tract Infection, (UTI) Is An Infection of One orLorebellNo ratings yet
- NCP Liver CirrhosisDocument7 pagesNCP Liver CirrhosisIris Jimenez-BuanNo ratings yet
- Fluid Volume DeficitDocument2 pagesFluid Volume DeficitRuby AnneNo ratings yet
- NCP Making (Ulcerative Colitis & Crohn's Disease)Document2 pagesNCP Making (Ulcerative Colitis & Crohn's Disease)R Hornilla ArcegaNo ratings yet
- NURSING CARE PLAN FOR CROHN'sDocument2 pagesNURSING CARE PLAN FOR CROHN'sMuhyeeSalaIdjadNo ratings yet
- NCPDocument9 pagesNCPTracy Camille EscobarNo ratings yet
- Upper Gastrointestin Al Bleeding: Case Presentation BSN 3-1Document80 pagesUpper Gastrointestin Al Bleeding: Case Presentation BSN 3-1Lanrose Parocha100% (1)
- Case: Liver Cirrhosis Assessment:: Nursing InferenceDocument7 pagesCase: Liver Cirrhosis Assessment:: Nursing InferenceLovelyn GanirNo ratings yet
- Fluid Volume DeficitDocument3 pagesFluid Volume Deficitprickybiik100% (1)
- Cues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale EvaluationDocument4 pagesCues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale Evaluationjomsportg0% (1)
- NCP Anorexia NervosaDocument5 pagesNCP Anorexia NervosaJohn Ver Tolentino AdaoNo ratings yet
- Nursing DiagnosisDocument4 pagesNursing DiagnosisLouren Marie DavidNo ratings yet
- Nursing Care PlanDocument14 pagesNursing Care PlanVin Landicho100% (1)
- Nursing Care PlanDocument22 pagesNursing Care PlanjamNo ratings yet
- Ineffective Airway ClearanceDocument2 pagesIneffective Airway ClearanceHanya Bint PotawanNo ratings yet
- Septic ShockDocument1 pageSeptic ShockShaine Wolfe100% (1)
- NCP For UtiDocument3 pagesNCP For UtiAaron Sanchez100% (1)
- Impaired Physical Mobility...Document3 pagesImpaired Physical Mobility...Christy BerryNo ratings yet
- Final Major Case StudyDocument17 pagesFinal Major Case Studyapi-546876878No ratings yet
- The First Film Philippine System Was Published On Aug 22, 2016 and Was Created by The Team of Gwenn Marie DimalantaDocument2 pagesThe First Film Philippine System Was Published On Aug 22, 2016 and Was Created by The Team of Gwenn Marie DimalantaErica Ruth CabrillasNo ratings yet
- Ncp-Impaired S.i.-NavidasDocument4 pagesNcp-Impaired S.i.-NavidasFran LanNo ratings yet
- Impaired Gas ExchangeDocument22 pagesImpaired Gas ExchangecheenapberberNo ratings yet
- COPD Care PLAN PDFDocument2 pagesCOPD Care PLAN PDFVanessaMUeller100% (1)
- Copd Case StudyDocument5 pagesCopd Case StudyJake Yvan DizonNo ratings yet
- NCP PneumoniaDocument28 pagesNCP PneumoniaW'ton Borbe83% (6)
- Signs and Symptoms Nursing Diagnosis Rationale Objective Nursing Intervention Rationale EvaluationDocument5 pagesSigns and Symptoms Nursing Diagnosis Rationale Objective Nursing Intervention Rationale EvaluationRemuelMagsinoNo ratings yet
- NCP - Drug Study - Peptic UlcerDocument18 pagesNCP - Drug Study - Peptic UlcerEmi EspinoNo ratings yet
- NCP Inffective Tissue PerfusionDocument3 pagesNCP Inffective Tissue PerfusionPaul Cubacub0% (1)
- NCP Imbalanced NutritionDocument3 pagesNCP Imbalanced NutritionAav Canlas100% (1)
- CystoclysisDocument2 pagesCystoclysisRaymond BasiloniaNo ratings yet
- Hypertonic SolutionsDocument4 pagesHypertonic SolutionsVanessa PaguiriganNo ratings yet
- NCPDocument7 pagesNCPChris Denver BancaleNo ratings yet
- Activity IntoleranceDocument2 pagesActivity Intolerancejunex123No ratings yet
- Impaired Tissue PerfusionDocument2 pagesImpaired Tissue PerfusionLyka Mae Imbat - PacnisNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goal: IndependentDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goal: IndependentNinaNo ratings yet
- NCP IschemicDocument19 pagesNCP IschemicChristina Espiña EjercitoNo ratings yet
- Lung Cancer (Nursing Care)Document5 pagesLung Cancer (Nursing Care)heiyuNo ratings yet
- Impaired Tissue IntegrityDocument2 pagesImpaired Tissue IntegrityJacoJone11100% (1)
- Risk For Fluid ImbalanceDocument8 pagesRisk For Fluid Imbalanceapi-277522722100% (1)
- Chronic Obstructive Bronchitis Is An Inflammation of The BronchiDocument9 pagesChronic Obstructive Bronchitis Is An Inflammation of The Bronchiinamaliit100% (1)
- CP Upper Gastrointestinal / Esophageal BleedingDocument5 pagesCP Upper Gastrointestinal / Esophageal Bleedingeyecatcher_0013532No ratings yet
- CP Upper Gastrointestinal / Esophageal BleedingDocument5 pagesCP Upper Gastrointestinal / Esophageal Bleedingeyecatcher_0013532No ratings yet
- PancreatitisDocument12 pagesPancreatitismardsz100% (5)
- PancreatitisDocument12 pagesPancreatitisapi-3797941100% (2)
- PancreatitisDocument12 pagesPancreatitisjhodane100% (4)
- Inflammatory Bowel DiseaseDocument16 pagesInflammatory Bowel Diseaseapi-3797941No ratings yet
- Nursing Care Plan For Inflammatory Bowel DiseaseDocument17 pagesNursing Care Plan For Inflammatory Bowel DiseaseLyka Joy DavilaNo ratings yet
- Ventilatory Assistance MechanicalDocument18 pagesVentilatory Assistance Mechanicalmardsz100% (5)
- UROLITHIASISDocument9 pagesUROLITHIASISmardsz100% (13)
- Sepsis SepticemiaDocument13 pagesSepsis Septicemiamardsz100% (10)
- Spinal Cord InjuryDocument26 pagesSpinal Cord Injurymardsz100% (13)
- Urinary Diversions UrostomyDocument15 pagesUrinary Diversions Urostomymardsz100% (3)
- TransplantationDocument11 pagesTransplantationmardsz100% (1)
- Total Joint ReplacementDocument10 pagesTotal Joint Replacementmardsz100% (6)
- Substance DependenceDocument16 pagesSubstance Dependencemardsz94% (18)
- THYROIDECTOMYDocument7 pagesTHYROIDECTOMYmardsz100% (8)
- Surgical InterventionDocument27 pagesSurgical Interventionmardsz100% (9)
- Respiratory AlkalosisDocument4 pagesRespiratory Alkalosismardsz100% (1)
- Seizure DisordersDocument12 pagesSeizure Disordersmardsz83% (6)
- Rheumatoid ArthritisDocument13 pagesRheumatoid ArthritisjhodaneNo ratings yet
- Respiratory AcidosisDocument5 pagesRespiratory Acidosisapi-376421583% (6)
- Renal Dialysis PeritonealDocument7 pagesRenal Dialysis Peritonealmardsz100% (2)
- Renal DialysisDocument14 pagesRenal Dialysisjhodane100% (1)
- Pediatric ConsiderationsDocument17 pagesPediatric ConsiderationsmardszNo ratings yet
- ProstatectomyDocument9 pagesProstatectomymardsz100% (1)
- PeritonitisDocument9 pagesPeritonitismardsz100% (4)
- Metabolic AlkalosisDocument4 pagesMetabolic AlkalosisCay Sevilla100% (1)
- PancreatitisDocument12 pagesPancreatitismardsz100% (5)
- Medical/Surgical: Select A System Plan From The List BelowDocument13 pagesMedical/Surgical: Select A System Plan From The List BelowmardszNo ratings yet
- Obesity Surgical InterventionsDocument12 pagesObesity Surgical Interventionsapi-3797941No ratings yet
- Metabolic Acid - Base ImbalancesDocument5 pagesMetabolic Acid - Base Imbalancesmardsz100% (1)
- Myocardial InfarctionDocument16 pagesMyocardial InfarctionCay Sevilla100% (4)
- MastectomyDocument12 pagesMastectomykkklllkl100% (1)
- LymphomasDocument10 pagesLymphomasapi-3797941No ratings yet
- Donna Eveline Prisca Panduu 1061050030 Pembimbing: Dr. Karyadi Prayanangga, SP - AnDocument20 pagesDonna Eveline Prisca Panduu 1061050030 Pembimbing: Dr. Karyadi Prayanangga, SP - AndonnaevelineNo ratings yet
- Guidelines On The Management of Postoperative PainDocument38 pagesGuidelines On The Management of Postoperative PainIeyna Key Nor Azmina100% (1)
- Examination of The Upper Cervical Spine PDFDocument22 pagesExamination of The Upper Cervical Spine PDFiikemNo ratings yet
- NCP, PL, DPDocument6 pagesNCP, PL, DPJazel Algara JompillaNo ratings yet
- Bridging The Gap Between Advances in - Research and Clinical Patient ManagemenDocument427 pagesBridging The Gap Between Advances in - Research and Clinical Patient ManagemenswagataNo ratings yet
- DAFTARDocument9 pagesDAFTARsugih warasNo ratings yet
- How Does Hypnosis WorkDocument11 pagesHow Does Hypnosis WorkchoileoNo ratings yet
- Cancer PainDocument52 pagesCancer PainIndraYudhi100% (1)
- Nursing Care Plan Rheumatoid ArthritisDocument3 pagesNursing Care Plan Rheumatoid ArthritisKath Mendoza Ü63% (8)
- Dermatomes Vs Peripheral Cutaneous NervesDocument9 pagesDermatomes Vs Peripheral Cutaneous NervesLala Qafsiel100% (1)
- Identification Data of PatientDocument12 pagesIdentification Data of PatientJyoti100% (6)
- 1156 The Effects of Acupuncture Versus Sham Acupuncture in The Treatment of Fibromyalgia A Randomized Controlled Clinical Trial FileDocument6 pages1156 The Effects of Acupuncture Versus Sham Acupuncture in The Treatment of Fibromyalgia A Randomized Controlled Clinical Trial FileValdemar Caumo JuniorNo ratings yet
- Articulo #6Document9 pagesArticulo #6Jorge GámezNo ratings yet
- Diagnostic Criteria For Burning Mouth Syndrome - Beta Version - 2020 - 11 - 17Document33 pagesDiagnostic Criteria For Burning Mouth Syndrome - Beta Version - 2020 - 11 - 17junipergreen07No ratings yet
- Harahsheh2017 Banderas RojasDocument8 pagesHarahsheh2017 Banderas RojasAngela LópezNo ratings yet
- From Jeanette Bicknell, Why Music Moves Us (Palgrave Macmillan, 2009)Document5 pagesFrom Jeanette Bicknell, Why Music Moves Us (Palgrave Macmillan, 2009)brianNo ratings yet
- Pain in Children With Autism Spectrum Disorder: Experience, Expression, and AssessmentDocument6 pagesPain in Children With Autism Spectrum Disorder: Experience, Expression, and Assessmentflower21No ratings yet
- Pain Management GuidelinesDocument54 pagesPain Management GuidelinesAlNo ratings yet
- 120 HAAD Exam QuestionsDocument13 pages120 HAAD Exam Questionsbien50% (2)
- Daun Kersen (Muntingia Calabura L.) Sebagai Alternatif Terapi Pada Penderita Gout ArtritisDocument9 pagesDaun Kersen (Muntingia Calabura L.) Sebagai Alternatif Terapi Pada Penderita Gout ArtritisdianNo ratings yet
- NCP NSD 2Document3 pagesNCP NSD 2Warren Bilog OleaNo ratings yet
- Scenar Testimonials (Updated)Document10 pagesScenar Testimonials (Updated)Tom Askew100% (1)
- Effect of Epidural Analgesia IDocument14 pagesEffect of Epidural Analgesia IRhandy SeptiantoNo ratings yet
- 2005 Self-Assessment Examination For Residents (Sae-R) : Abridged VersionDocument22 pages2005 Self-Assessment Examination For Residents (Sae-R) : Abridged VersionSoumabho DasNo ratings yet
- MCQ Pathways9th.IDocument4 pagesMCQ Pathways9th.Iareej alblowi100% (1)
- Orthopedic NursingDocument21 pagesOrthopedic NursingCris Constantino San JuanNo ratings yet




















































































































Download as rtf, pdf, or txt
You might also like
- Nursing Care Plan 6 Impaired Gas ExchangeDocument9 pagesNursing Care Plan 6 Impaired Gas Exchangedbryant0101100% (12)
- Nursing Care Plan: Risk For Disuse SyndromeDocument2 pagesNursing Care Plan: Risk For Disuse SyndromeRozsy FakhrurNo ratings yet
- Nursing Care Plans For Acute ConfusionDocument3 pagesNursing Care Plans For Acute Confusionynecesity75% (4)
- The Back Book PDFDocument14 pagesThe Back Book PDFfoldsnholdsNo ratings yet
- Acute Intermittent Porphyria. General Aspects With Focus On PainDocument8 pagesAcute Intermittent Porphyria. General Aspects With Focus On PainAugusto Espada AraozNo ratings yet
- PBL 1Document7 pagesPBL 1Skyla Fiesta100% (1)
- Risk For InfectionDocument18 pagesRisk For InfectionValiant Baybay0% (1)
- Hypothyroidism Nursing Care PlanDocument2 pagesHypothyroidism Nursing Care Planmrhammer1957100% (2)
- Case Study On Fluid OverloadDocument37 pagesCase Study On Fluid OverloadradicalmpNo ratings yet
- Colon Rectal CancerDocument6 pagesColon Rectal Cancerbryantmaroney811No ratings yet
- ThrombophlebitisDocument10 pagesThrombophlebitismardsz100% (3)
- Sickle Cell CrisisDocument16 pagesSickle Cell Crisismardsz83% (12)
- NCP: Chronic Renal FailureDocument14 pagesNCP: Chronic Renal FailureJavie77% (13)
- Neck Pain Disability Index QuestionnaireDocument2 pagesNeck Pain Disability Index QuestionnaireLiliana Andrei Toader100% (1)
- Stoddard - Osteopathic-Technique PDFDocument271 pagesStoddard - Osteopathic-Technique PDFmitroisergiuNo ratings yet
- Nursing Care Plan For AIDS HIVDocument3 pagesNursing Care Plan For AIDS HIVFARAH MAE MEDINA100% (2)
- Impaired Electrolytes NCPDocument2 pagesImpaired Electrolytes NCPNora BacolNo ratings yet
- NCP Crohn'sDocument2 pagesNCP Crohn'sJanice Marco100% (1)
- NCP Copd4Document15 pagesNCP Copd4Alessa Marie Crisostomo Salazar100% (1)
- Massive AscitesDocument12 pagesMassive Ascitesranitidin100% (1)
- Urinary Tract Infection, (UTI) Is An Infection of One orDocument4 pagesUrinary Tract Infection, (UTI) Is An Infection of One orLorebellNo ratings yet
- NCP Liver CirrhosisDocument7 pagesNCP Liver CirrhosisIris Jimenez-BuanNo ratings yet
- Fluid Volume DeficitDocument2 pagesFluid Volume DeficitRuby AnneNo ratings yet
- NCP Making (Ulcerative Colitis & Crohn's Disease)Document2 pagesNCP Making (Ulcerative Colitis & Crohn's Disease)R Hornilla ArcegaNo ratings yet
- NURSING CARE PLAN FOR CROHN'sDocument2 pagesNURSING CARE PLAN FOR CROHN'sMuhyeeSalaIdjadNo ratings yet
- NCPDocument9 pagesNCPTracy Camille EscobarNo ratings yet
- Upper Gastrointestin Al Bleeding: Case Presentation BSN 3-1Document80 pagesUpper Gastrointestin Al Bleeding: Case Presentation BSN 3-1Lanrose Parocha100% (1)
- Case: Liver Cirrhosis Assessment:: Nursing InferenceDocument7 pagesCase: Liver Cirrhosis Assessment:: Nursing InferenceLovelyn GanirNo ratings yet
- Fluid Volume DeficitDocument3 pagesFluid Volume Deficitprickybiik100% (1)
- Cues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale EvaluationDocument4 pagesCues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale Evaluationjomsportg0% (1)
- NCP Anorexia NervosaDocument5 pagesNCP Anorexia NervosaJohn Ver Tolentino AdaoNo ratings yet
- Nursing DiagnosisDocument4 pagesNursing DiagnosisLouren Marie DavidNo ratings yet
- Nursing Care PlanDocument14 pagesNursing Care PlanVin Landicho100% (1)
- Nursing Care PlanDocument22 pagesNursing Care PlanjamNo ratings yet
- Ineffective Airway ClearanceDocument2 pagesIneffective Airway ClearanceHanya Bint PotawanNo ratings yet
- Septic ShockDocument1 pageSeptic ShockShaine Wolfe100% (1)
- NCP For UtiDocument3 pagesNCP For UtiAaron Sanchez100% (1)
- Impaired Physical Mobility...Document3 pagesImpaired Physical Mobility...Christy BerryNo ratings yet
- Final Major Case StudyDocument17 pagesFinal Major Case Studyapi-546876878No ratings yet
- The First Film Philippine System Was Published On Aug 22, 2016 and Was Created by The Team of Gwenn Marie DimalantaDocument2 pagesThe First Film Philippine System Was Published On Aug 22, 2016 and Was Created by The Team of Gwenn Marie DimalantaErica Ruth CabrillasNo ratings yet
- Ncp-Impaired S.i.-NavidasDocument4 pagesNcp-Impaired S.i.-NavidasFran LanNo ratings yet
- Impaired Gas ExchangeDocument22 pagesImpaired Gas ExchangecheenapberberNo ratings yet
- COPD Care PLAN PDFDocument2 pagesCOPD Care PLAN PDFVanessaMUeller100% (1)
- Copd Case StudyDocument5 pagesCopd Case StudyJake Yvan DizonNo ratings yet
- NCP PneumoniaDocument28 pagesNCP PneumoniaW'ton Borbe83% (6)
- Signs and Symptoms Nursing Diagnosis Rationale Objective Nursing Intervention Rationale EvaluationDocument5 pagesSigns and Symptoms Nursing Diagnosis Rationale Objective Nursing Intervention Rationale EvaluationRemuelMagsinoNo ratings yet
- NCP - Drug Study - Peptic UlcerDocument18 pagesNCP - Drug Study - Peptic UlcerEmi EspinoNo ratings yet
- NCP Inffective Tissue PerfusionDocument3 pagesNCP Inffective Tissue PerfusionPaul Cubacub0% (1)
- NCP Imbalanced NutritionDocument3 pagesNCP Imbalanced NutritionAav Canlas100% (1)
- CystoclysisDocument2 pagesCystoclysisRaymond BasiloniaNo ratings yet
- Hypertonic SolutionsDocument4 pagesHypertonic SolutionsVanessa PaguiriganNo ratings yet
- NCPDocument7 pagesNCPChris Denver BancaleNo ratings yet
- Activity IntoleranceDocument2 pagesActivity Intolerancejunex123No ratings yet
- Impaired Tissue PerfusionDocument2 pagesImpaired Tissue PerfusionLyka Mae Imbat - PacnisNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goal: IndependentDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goal: IndependentNinaNo ratings yet
- NCP IschemicDocument19 pagesNCP IschemicChristina Espiña EjercitoNo ratings yet
- Lung Cancer (Nursing Care)Document5 pagesLung Cancer (Nursing Care)heiyuNo ratings yet
- Impaired Tissue IntegrityDocument2 pagesImpaired Tissue IntegrityJacoJone11100% (1)
- Risk For Fluid ImbalanceDocument8 pagesRisk For Fluid Imbalanceapi-277522722100% (1)
- Chronic Obstructive Bronchitis Is An Inflammation of The BronchiDocument9 pagesChronic Obstructive Bronchitis Is An Inflammation of The Bronchiinamaliit100% (1)
- CP Upper Gastrointestinal / Esophageal BleedingDocument5 pagesCP Upper Gastrointestinal / Esophageal Bleedingeyecatcher_0013532No ratings yet
- CP Upper Gastrointestinal / Esophageal BleedingDocument5 pagesCP Upper Gastrointestinal / Esophageal Bleedingeyecatcher_0013532No ratings yet
- PancreatitisDocument12 pagesPancreatitismardsz100% (5)
- PancreatitisDocument12 pagesPancreatitisapi-3797941100% (2)
- PancreatitisDocument12 pagesPancreatitisjhodane100% (4)
- Inflammatory Bowel DiseaseDocument16 pagesInflammatory Bowel Diseaseapi-3797941No ratings yet
- Nursing Care Plan For Inflammatory Bowel DiseaseDocument17 pagesNursing Care Plan For Inflammatory Bowel DiseaseLyka Joy DavilaNo ratings yet
- Ventilatory Assistance MechanicalDocument18 pagesVentilatory Assistance Mechanicalmardsz100% (5)
- UROLITHIASISDocument9 pagesUROLITHIASISmardsz100% (13)
- Sepsis SepticemiaDocument13 pagesSepsis Septicemiamardsz100% (10)
- Spinal Cord InjuryDocument26 pagesSpinal Cord Injurymardsz100% (13)
- Urinary Diversions UrostomyDocument15 pagesUrinary Diversions Urostomymardsz100% (3)
- TransplantationDocument11 pagesTransplantationmardsz100% (1)
- Total Joint ReplacementDocument10 pagesTotal Joint Replacementmardsz100% (6)
- Substance DependenceDocument16 pagesSubstance Dependencemardsz94% (18)
- THYROIDECTOMYDocument7 pagesTHYROIDECTOMYmardsz100% (8)
- Surgical InterventionDocument27 pagesSurgical Interventionmardsz100% (9)
- Respiratory AlkalosisDocument4 pagesRespiratory Alkalosismardsz100% (1)
- Seizure DisordersDocument12 pagesSeizure Disordersmardsz83% (6)
- Rheumatoid ArthritisDocument13 pagesRheumatoid ArthritisjhodaneNo ratings yet
- Respiratory AcidosisDocument5 pagesRespiratory Acidosisapi-376421583% (6)
- Renal Dialysis PeritonealDocument7 pagesRenal Dialysis Peritonealmardsz100% (2)
- Renal DialysisDocument14 pagesRenal Dialysisjhodane100% (1)
- Pediatric ConsiderationsDocument17 pagesPediatric ConsiderationsmardszNo ratings yet
- ProstatectomyDocument9 pagesProstatectomymardsz100% (1)
- PeritonitisDocument9 pagesPeritonitismardsz100% (4)
- Metabolic AlkalosisDocument4 pagesMetabolic AlkalosisCay Sevilla100% (1)
- PancreatitisDocument12 pagesPancreatitismardsz100% (5)
- Medical/Surgical: Select A System Plan From The List BelowDocument13 pagesMedical/Surgical: Select A System Plan From The List BelowmardszNo ratings yet
- Obesity Surgical InterventionsDocument12 pagesObesity Surgical Interventionsapi-3797941No ratings yet
- Metabolic Acid - Base ImbalancesDocument5 pagesMetabolic Acid - Base Imbalancesmardsz100% (1)
- Myocardial InfarctionDocument16 pagesMyocardial InfarctionCay Sevilla100% (4)
- MastectomyDocument12 pagesMastectomykkklllkl100% (1)
- LymphomasDocument10 pagesLymphomasapi-3797941No ratings yet
- Donna Eveline Prisca Panduu 1061050030 Pembimbing: Dr. Karyadi Prayanangga, SP - AnDocument20 pagesDonna Eveline Prisca Panduu 1061050030 Pembimbing: Dr. Karyadi Prayanangga, SP - AndonnaevelineNo ratings yet
- Guidelines On The Management of Postoperative PainDocument38 pagesGuidelines On The Management of Postoperative PainIeyna Key Nor Azmina100% (1)
- Examination of The Upper Cervical Spine PDFDocument22 pagesExamination of The Upper Cervical Spine PDFiikemNo ratings yet
- NCP, PL, DPDocument6 pagesNCP, PL, DPJazel Algara JompillaNo ratings yet
- Bridging The Gap Between Advances in - Research and Clinical Patient ManagemenDocument427 pagesBridging The Gap Between Advances in - Research and Clinical Patient ManagemenswagataNo ratings yet
- DAFTARDocument9 pagesDAFTARsugih warasNo ratings yet
- How Does Hypnosis WorkDocument11 pagesHow Does Hypnosis WorkchoileoNo ratings yet
- Cancer PainDocument52 pagesCancer PainIndraYudhi100% (1)
- Nursing Care Plan Rheumatoid ArthritisDocument3 pagesNursing Care Plan Rheumatoid ArthritisKath Mendoza Ü63% (8)
- Dermatomes Vs Peripheral Cutaneous NervesDocument9 pagesDermatomes Vs Peripheral Cutaneous NervesLala Qafsiel100% (1)
- Identification Data of PatientDocument12 pagesIdentification Data of PatientJyoti100% (6)
- 1156 The Effects of Acupuncture Versus Sham Acupuncture in The Treatment of Fibromyalgia A Randomized Controlled Clinical Trial FileDocument6 pages1156 The Effects of Acupuncture Versus Sham Acupuncture in The Treatment of Fibromyalgia A Randomized Controlled Clinical Trial FileValdemar Caumo JuniorNo ratings yet
- Articulo #6Document9 pagesArticulo #6Jorge GámezNo ratings yet
- Diagnostic Criteria For Burning Mouth Syndrome - Beta Version - 2020 - 11 - 17Document33 pagesDiagnostic Criteria For Burning Mouth Syndrome - Beta Version - 2020 - 11 - 17junipergreen07No ratings yet
- Harahsheh2017 Banderas RojasDocument8 pagesHarahsheh2017 Banderas RojasAngela LópezNo ratings yet
- From Jeanette Bicknell, Why Music Moves Us (Palgrave Macmillan, 2009)Document5 pagesFrom Jeanette Bicknell, Why Music Moves Us (Palgrave Macmillan, 2009)brianNo ratings yet
- Pain in Children With Autism Spectrum Disorder: Experience, Expression, and AssessmentDocument6 pagesPain in Children With Autism Spectrum Disorder: Experience, Expression, and Assessmentflower21No ratings yet
- Pain Management GuidelinesDocument54 pagesPain Management GuidelinesAlNo ratings yet
- 120 HAAD Exam QuestionsDocument13 pages120 HAAD Exam Questionsbien50% (2)
- Daun Kersen (Muntingia Calabura L.) Sebagai Alternatif Terapi Pada Penderita Gout ArtritisDocument9 pagesDaun Kersen (Muntingia Calabura L.) Sebagai Alternatif Terapi Pada Penderita Gout ArtritisdianNo ratings yet
- NCP NSD 2Document3 pagesNCP NSD 2Warren Bilog OleaNo ratings yet
- Scenar Testimonials (Updated)Document10 pagesScenar Testimonials (Updated)Tom Askew100% (1)
- Effect of Epidural Analgesia IDocument14 pagesEffect of Epidural Analgesia IRhandy SeptiantoNo ratings yet
- 2005 Self-Assessment Examination For Residents (Sae-R) : Abridged VersionDocument22 pages2005 Self-Assessment Examination For Residents (Sae-R) : Abridged VersionSoumabho DasNo ratings yet
- MCQ Pathways9th.IDocument4 pagesMCQ Pathways9th.Iareej alblowi100% (1)
- Orthopedic NursingDocument21 pagesOrthopedic NursingCris Constantino San JuanNo ratings yet