Download as pdf or txt
You might also like
- PER1 1aDocument8 pagesPER1 1aFri Fardy100% (1)
- 1 Infection Prevention and ControlDocument57 pages1 Infection Prevention and Controlmariam100% (3)
- Cosmetic Dermatology: Products and ProceduresFrom EverandCosmetic Dermatology: Products and ProceduresRating: 5 out of 5 stars5/5 (1)
- Michie Et Al 2014Document44 pagesMichie Et Al 2014serveh80No ratings yet
- MED. Dental Services (Infectionn Control 1) .003docDocument7 pagesMED. Dental Services (Infectionn Control 1) .003docKenny JosefNo ratings yet
- 2013 - BestPractices For HLDDocument53 pages2013 - BestPractices For HLDDaniela Cirnatu100% (1)
- 1) Infection Control For Prosthodontic ClinicDocument50 pages1) Infection Control For Prosthodontic ClinicmanoNo ratings yet
- SiD 4.3.3.3 at 7 June 2011Document4 pagesSiD 4.3.3.3 at 7 June 2011Dr-Mohamed KandeelNo ratings yet
- Community Lec3Document25 pagesCommunity Lec3woow0217No ratings yet
- Infection Control in Dentistry FinalDocument12 pagesInfection Control in Dentistry FinalDevAshish BNo ratings yet
- ASepsisDocument52 pagesASepsisnew biee100% (1)
- Endoscope ReprocessingDocument34 pagesEndoscope Reprocessingmonir61100% (2)
- PRESENTATION: Primum Non Nocere, Deinde Curare Also Applies To HospitalsDocument26 pagesPRESENTATION: Primum Non Nocere, Deinde Curare Also Applies To HospitalsADB Health Sector Group0% (1)
- Infection. Prevention and Control of Healthcare-Associated Infections in Primary and Community Care.Document24 pagesInfection. Prevention and Control of Healthcare-Associated Infections in Primary and Community Care.Madalina TalpauNo ratings yet
- Environmental Science: Dr. Hemanta MedhiDocument14 pagesEnvironmental Science: Dr. Hemanta MedhiItmej NNo ratings yet
- A? A? A? A? A?: Nosocomial Epidemiology Public HealthDocument8 pagesA? A? A? A? A?: Nosocomial Epidemiology Public HealthAbhijeet TambeNo ratings yet
- Key Points of The Program For Disinfection Technology in Special Places During The Coronavirus Disease-2019 (COVID-19) OutbreakDocument3 pagesKey Points of The Program For Disinfection Technology in Special Places During The Coronavirus Disease-2019 (COVID-19) Outbreakthebestcrypto123No ratings yet
- Pidsr Manual On Infection ControlDocument4 pagesPidsr Manual On Infection ControlKristine EstrellaNo ratings yet
- Infection Control in Dentistry: Done By: M.Janani Sri 3rd Year B.D.SDocument20 pagesInfection Control in Dentistry: Done By: M.Janani Sri 3rd Year B.D.SiamsubashreeNo ratings yet
- 4809 Volume 10 Decontamination of Equipment PDFDocument10 pages4809 Volume 10 Decontamination of Equipment PDFARIKANo ratings yet
- MED. Dental Services (Water Lines & Water Monitoring) .004docDocument5 pagesMED. Dental Services (Water Lines & Water Monitoring) .004docKenny JosefNo ratings yet
- Guidelines For Routine Environmental Cleaning of The Operating RoomDocument13 pagesGuidelines For Routine Environmental Cleaning of The Operating RoomYnaffit Alteza UntalNo ratings yet
- UntitledDocument15 pagesUntitledRao SNo ratings yet
- Sterilization of Ortho Instruments / Orthodontic Courses by Indian Dental AcademyDocument57 pagesSterilization of Ortho Instruments / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Hospital Waste Management PlanDocument4 pagesHospital Waste Management PlanPraiseGod'borngreat Chidozie Emenike100% (1)
- Physical Environment (Household Cleaning) : 5.2 VentilationDocument12 pagesPhysical Environment (Household Cleaning) : 5.2 VentilationliuslinoNo ratings yet
- Infection ControlDocument5 pagesInfection Controldrdarshak100% (1)
- Hospital Textiles, Are They A Possible Vehicle For Healthcare-Associated Infections?Document14 pagesHospital Textiles, Are They A Possible Vehicle For Healthcare-Associated Infections?Muhammad Nadeem RazaNo ratings yet
- Inf Control DentalDocument11 pagesInf Control Dentals01223145725No ratings yet
- !!! Environmental-persistence-of-SARS - CoV - 2-Virus-Options-For-Cleaning2020-03-26 - 0Document5 pages!!! Environmental-persistence-of-SARS - CoV - 2-Virus-Options-For-Cleaning2020-03-26 - 0Silvester KolicNo ratings yet
- JTallon - Keeping Hospitals CleanDocument37 pagesJTallon - Keeping Hospitals CleanHaroon RasheedNo ratings yet
- Endoscope DisinfectionDocument14 pagesEndoscope Disinfectioneliasox123No ratings yet
- INTRODUCTION To ENDOSCOPY For Physician Assistants Class 2Document34 pagesINTRODUCTION To ENDOSCOPY For Physician Assistants Class 2Sathya PrabaNo ratings yet
- Infection Control in Surgical PracticeDocument41 pagesInfection Control in Surgical PracticeMuhammad Azeem KhanNo ratings yet
- 6 Reprocessing of EndosDocument28 pages6 Reprocessing of Endoshananshosha743No ratings yet
- Lec 11 PDFDocument8 pagesLec 11 PDFFlorida ManNo ratings yet
- Biomedical WasteDocument14 pagesBiomedical WasteYogesh ShigvanNo ratings yet
- National Guidelines For Safe Dental Practice During Covid-19 PandemicDocument7 pagesNational Guidelines For Safe Dental Practice During Covid-19 PandemicSatisha TSNo ratings yet
- Ipccc 23937Document226 pagesIpccc 23937سامح سلامهNo ratings yet
- 007 Policies Infection ControlDocument16 pages007 Policies Infection ControllabiaernestoNo ratings yet
- The New Images of Infection Control AND Sterilization GuidelinesDocument43 pagesThe New Images of Infection Control AND Sterilization GuidelinesLama AhmadNo ratings yet
- Bio-Medical Waste Management: Risk To Human HealthDocument4 pagesBio-Medical Waste Management: Risk To Human HealthtriratnacomNo ratings yet
- Operation Theatre Basic Architecture PDFDocument6 pagesOperation Theatre Basic Architecture PDFnatmita08No ratings yet
- Endoscope Reprocessing Risk and Current Risk PracticeDocument65 pagesEndoscope Reprocessing Risk and Current Risk PracticeHosam GomaaNo ratings yet
- AnestesiaDocument2 pagesAnestesiaMarcus PorterNo ratings yet
- Gerpac 2014 ReviewDocument3 pagesGerpac 2014 ReviewTim SandleNo ratings yet
- My SeminarDocument52 pagesMy SeminarvinnycoolbuddyNo ratings yet
- Infection Control in DentistryDocument69 pagesInfection Control in DentistryShahrukh ali khanNo ratings yet
- 3 Healthcare Waste ManagementDocument35 pages3 Healthcare Waste ManagementmariamNo ratings yet
- BSG Guidelines Decontamination of Equipment For Gastrointestinal EndosDocument25 pagesBSG Guidelines Decontamination of Equipment For Gastrointestinal Endoshani1986yeNo ratings yet
- Housekeeping Manual 2014Document33 pagesHousekeeping Manual 2014Francesca AckumburNo ratings yet
- Introduction in Surgery ASEPSIS AND ANTISEPSISDocument20 pagesIntroduction in Surgery ASEPSIS AND ANTISEPSISHana100% (1)
- HPS Endoscope Decontamination 2004 PDFDocument190 pagesHPS Endoscope Decontamination 2004 PDFHong-Nam Kim100% (1)
- Standard Precautions (Autosaved)Document15 pagesStandard Precautions (Autosaved)Avantika SharmaNo ratings yet
- 3.8.25 Physical TherapyDocument25 pages3.8.25 Physical TherapyNeil OsborneNo ratings yet
- Waste ManagementDocument25 pagesWaste ManagementDeep_Heart71% (7)
- The Basics of SterilizationDocument9 pagesThe Basics of SterilizationMohammed YousffiNo ratings yet
- 3.2 Dr. Taufin SpOT - Operating RoomDocument29 pages3.2 Dr. Taufin SpOT - Operating RoomTaqwatin Ma'rifahNo ratings yet
- Nursing care process in patients with chronic obstructive pulmonary diseaseFrom EverandNursing care process in patients with chronic obstructive pulmonary diseaseNo ratings yet
- Handbook of Emergency Disposal and Management of Medical Waste in ChinaFrom EverandHandbook of Emergency Disposal and Management of Medical Waste in ChinaNo ratings yet
- Practical Manual for Detection of Parasites in Feces, Blood and Urine SamplesFrom EverandPractical Manual for Detection of Parasites in Feces, Blood and Urine SamplesNo ratings yet
- Providing Oral CareDocument54 pagesProviding Oral CareErcel ArellanoNo ratings yet
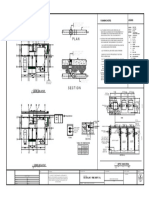
- 01-rmh Setingkat-Model 6Document1 page01-rmh Setingkat-Model 6Amirul AdamNo ratings yet
- Humanitarian Situation Report No. 10: HighlightsDocument5 pagesHumanitarian Situation Report No. 10: HighlightsSoe Thiha TinNo ratings yet
- Safety GoalsDocument18 pagesSafety Goalsprisma1No ratings yet
- SOP Personnel HygieneDocument4 pagesSOP Personnel HygieneBejoy Karim100% (3)
- InvisiblesunblockDocument1 pageInvisiblesunblockDavidNo ratings yet
- Standard Precautions 1Document34 pagesStandard Precautions 1Melody LandichoNo ratings yet
- Water SupplyDocument19 pagesWater SupplyAngelo John R. JavinezNo ratings yet
- Doe School PlanDocument16 pagesDoe School PlanHNNNo ratings yet
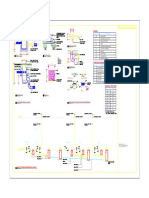
- Plumbing Notes: Legend:: 1.50 0.70 Mts 0.70 MtsDocument1 pagePlumbing Notes: Legend:: 1.50 0.70 Mts 0.70 MtsGhian Carlo Garcia CalibuyotNo ratings yet
- Training Plan VCI TemplateDocument67 pagesTraining Plan VCI TemplateJohn Cesar Cam AntiqueNo ratings yet
- Manual - Solar Disinfection of Water - SODISDocument88 pagesManual - Solar Disinfection of Water - SODISNayraCampos100% (1)
- Material Safety Data Sheet: Product Name: NUTO H 68Document60 pagesMaterial Safety Data Sheet: Product Name: NUTO H 68Rodolfo Mata LoeraNo ratings yet
- Summary (Quantity Based On 269 Flats) : Flexible Hose RequiredDocument7 pagesSummary (Quantity Based On 269 Flats) : Flexible Hose RequiredArun UdayabhanuNo ratings yet
- WordsearchDocument2 pagesWordsearchpepac414No ratings yet
- WEEKLY CONSUMPTION REPORT May, 2023Document2 pagesWEEKLY CONSUMPTION REPORT May, 2023OMOKARO GORDONNo ratings yet
- Oriflame Products Knowledge-1Document14 pagesOriflame Products Knowledge-1Aqsa100% (3)
- Hygiene Is A Component of Education Which, in The Sportive and in Any Person WhoDocument2 pagesHygiene Is A Component of Education Which, in The Sportive and in Any Person WhoVladGrosuNo ratings yet
- Project Report ON Service Delivery: in Thuravoor Grama PanchayatDocument19 pagesProject Report ON Service Delivery: in Thuravoor Grama PanchayatAbinash NandaNo ratings yet
- S.N Product Weight Quantity: Chart Title Chart TitleDocument4 pagesS.N Product Weight Quantity: Chart Title Chart Titleमनोज मोक्तान ब्लोनNo ratings yet
- Grade 12 Mathematics Platinum Navigation PackDocument71 pagesGrade 12 Mathematics Platinum Navigation PackAlicia Magama100% (1)
- Haccp Plan - Rework Megalac / CaspfaDocument10 pagesHaccp Plan - Rework Megalac / CaspfaafrizalNo ratings yet
- AyurvedaDocument2 pagesAyurvedaHana GinaNo ratings yet
- Cleaning PointsDocument15 pagesCleaning PointsJosie Navaja100% (1)
- 4 Cleanliness and HygieneDocument4 pages4 Cleanliness and HygienekarthikbolluNo ratings yet
- Covid-19 Safety PlanDocument9 pagesCovid-19 Safety Planapi-481613484No ratings yet
- Standard Design - Septic - TankDocument39 pagesStandard Design - Septic - Tankamantz91No ratings yet
- Food Safety Training Guide Level 2 PDFDocument56 pagesFood Safety Training Guide Level 2 PDFNaeem MalikNo ratings yet
- IP and FNCP KoDocument4 pagesIP and FNCP KoPam GonzalesNo ratings yet