Download as doc, pdf, or txt
You might also like
- NCDC-2 Physical Health Inventory Form A4Document6 pagesNCDC-2 Physical Health Inventory Form A4knock medinaNo ratings yet
- Medical Check Up FormDocument4 pagesMedical Check Up FormDevesh Chauhan60% (5)
- Nursing Care Plan FormatDocument4 pagesNursing Care Plan Formatprince242653100% (1)
- Health Assessment FormDocument3 pagesHealth Assessment FormDarlen RabanoNo ratings yet
- Welcome Letter Template For Group CounselingDocument2 pagesWelcome Letter Template For Group CounselingNurses For Tobacco ControlNo ratings yet
- Graduate SOAP NOTE TEMPLATEDocument7 pagesGraduate SOAP NOTE TEMPLATEMiley MunozNo ratings yet
- Medical History FormDocument1 pageMedical History FormMariel Vargas CamposNo ratings yet
- Patient Medication History InterviewDocument3 pagesPatient Medication History InterviewrazeghiNo ratings yet
- Initial Nutrition AssessmentDocument2 pagesInitial Nutrition Assessmentapi-511287144No ratings yet
- Ncar ColonosDocument15 pagesNcar ColonosMARLA PHOEBE KYTE MULLETNo ratings yet
- Patients ChartDocument1 pagePatients ChartLovely HackeyNo ratings yet
- Patient RecordDocument1 pagePatient Recordben peloniaNo ratings yet
- Mini SBAR Report SheetDocument3 pagesMini SBAR Report Sheetthe201girlsNo ratings yet
- BH Clinical Assessment FormDocument2 pagesBH Clinical Assessment FormMac MacapilNo ratings yet
- Republic of The Philippines Province of Rizal Medical-Dental Health ServicesDocument1 pageRepublic of The Philippines Province of Rizal Medical-Dental Health ServicesCes ReyesNo ratings yet
- Student Physician FormDocument1 pageStudent Physician FormMasr RedaNo ratings yet
- 7.8 Collect Data & Come Up With Plan For Day & Nursing Diagnosis Pre-Conference 8-9 Vitals Then Chart, AM Care, StartDocument2 pages7.8 Collect Data & Come Up With Plan For Day & Nursing Diagnosis Pre-Conference 8-9 Vitals Then Chart, AM Care, StartSade' CovingtonNo ratings yet
- Otcsoap Grid Table Template Fall14w15Document2 pagesOtcsoap Grid Table Template Fall14w15api-286238965No ratings yet
- Georgia College and State University School of Nursing Episodic DocumentDocument11 pagesGeorgia College and State University School of Nursing Episodic Documentapi-310557802No ratings yet
- Nursing Nursing Care PlanDocument15 pagesNursing Nursing Care Planyourmom111No ratings yet
- Medical Form For Grade 7 12Document3 pagesMedical Form For Grade 7 12Deonna Angeline100% (1)
- Final Emr Sbirt Adult II RevDocument11 pagesFinal Emr Sbirt Adult II Revapi-310557802No ratings yet
- Specimen Diabetic Supplementary Statement 2016Document1 pageSpecimen Diabetic Supplementary Statement 2016achintya8No ratings yet
- MDPU Clinical Self Report FormDocument2 pagesMDPU Clinical Self Report FormMohammad AlsuwaidanNo ratings yet
- Obstetric FormDocument4 pagesObstetric FormKhylamarie VillalunaNo ratings yet
- Student Health Record: Republic of The PhilippinesDocument3 pagesStudent Health Record: Republic of The PhilippinesYell ManiponNo ratings yet
- Endocrine Students Guide-2Document2 pagesEndocrine Students Guide-2DR. MUSICNo ratings yet
- Adult Weight Management ToolkitDocument4 pagesAdult Weight Management ToolkitAmany Salama67% (3)
- Nutrition AssessmentDocument4 pagesNutrition AssessmentmarciadaddsNo ratings yet
- Adime Note Template1Document1 pageAdime Note Template1api-242225348No ratings yet
- Piddig District Hospital: History and Physical ExaminationDocument2 pagesPiddig District Hospital: History and Physical ExaminationMark Emil BautistaNo ratings yet
- Abdominal WorksheetDocument1 pageAbdominal WorksheetJennyNo ratings yet
- Comprehensive H&PDocument2 pagesComprehensive H&PjwwisnerNo ratings yet
- Obstetrics History General DataDocument7 pagesObstetrics History General DataColeen NeyraNo ratings yet
- Example of Completed Form: Admit Dx/Chief Complaint/Hx Current ILLNESS: - Bowel Obstruction RespiratoryDocument3 pagesExample of Completed Form: Admit Dx/Chief Complaint/Hx Current ILLNESS: - Bowel Obstruction RespiratoryJosephNo ratings yet
- Antenatal BookDocument20 pagesAntenatal BookNurmunirah DasnanNo ratings yet
- HTP and DX Study 1Document2 pagesHTP and DX Study 1JHON KURT MONIBETNo ratings yet
- PT Assessment ToolDocument2 pagesPT Assessment ToolSally GigelioNo ratings yet
- Patient Data SheetDocument1 pagePatient Data SheetLeanne TorresNo ratings yet
- Discharge Plan FormatDocument1 pageDischarge Plan FormatSuzette Rae TateNo ratings yet
- Tangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationDocument3 pagesTangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationbenNo ratings yet
- 2.physical E, HISTORY NCPDocument13 pages2.physical E, HISTORY NCPمريم حجيNo ratings yet
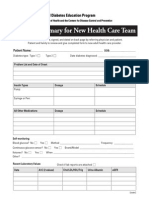
- Clinical Summary For New Health Care Team: R R R R R R RDocument2 pagesClinical Summary For New Health Care Team: R R R R R R RDana GrigorescuNo ratings yet
- History Taking FormDocument14 pagesHistory Taking FormFebbie ArcalesNo ratings yet
- Primary Health Care HandoutsDocument34 pagesPrimary Health Care HandoutspauchanmnlNo ratings yet
- Obstetric Assessment ToolDocument5 pagesObstetric Assessment ToolDudil GoatNo ratings yet
- Case Study FormatDocument9 pagesCase Study FormatakinameeNo ratings yet
- Diabetes Assessment FormDocument2 pagesDiabetes Assessment FormAhmad JamaluddinNo ratings yet
- 100 MCQ S Community MedicineDocument100 pages100 MCQ S Community Medicinehassan qureshiNo ratings yet
- Peace Corps Alcohol/Substance Abuse Current Evaluation Form PC-262-6 (Initial Approval 08/2012Document5 pagesPeace Corps Alcohol/Substance Abuse Current Evaluation Form PC-262-6 (Initial Approval 08/2012Accessible Journal Media: Peace Corps DocumentsNo ratings yet
- Students Medical RecordDocument2 pagesStudents Medical RecordMary Grace EncisaNo ratings yet
- P.A. Tool (Case Pres FINAL.)Document23 pagesP.A. Tool (Case Pres FINAL.)Crystal Ann TadiamonNo ratings yet
- Tobacco 5asdoc 5Document2 pagesTobacco 5asdoc 5dwyneNo ratings yet
- Assessment - Critical CareDocument1 pageAssessment - Critical CareMartini ListrikNo ratings yet
- SHUMAILADocument11 pagesSHUMAILALord arainNo ratings yet
- Auerbach Breast Center Patient Medical HistoryDocument1 pageAuerbach Breast Center Patient Medical Historydeepeezee_beenNo ratings yet
- Demographic Data & Health HistoryDocument1 pageDemographic Data & Health HistorysugarmontejoNo ratings yet
- General Health Profiling Questionnaire For Punjab University StudentsDocument4 pagesGeneral Health Profiling Questionnaire For Punjab University StudentsMuhammad YousafNo ratings yet
- General Health Profiling Questionnaire For Punjab University StudentsDocument4 pagesGeneral Health Profiling Questionnaire For Punjab University StudentsMuhammad YousafNo ratings yet
- Clinical Record Form: (May Be Completed by Patient)Document11 pagesClinical Record Form: (May Be Completed by Patient)joseNo ratings yet
- Discharge PlanDocument3 pagesDischarge PlanDoneva Lyn MedinaNo ratings yet
- Curriculum Vitae Jeannette O. Andrews PHD, RN, FNP, Faan: J.Andrews@Sc - EduDocument39 pagesCurriculum Vitae Jeannette O. Andrews PHD, RN, FNP, Faan: J.Andrews@Sc - EduNurses For Tobacco ControlNo ratings yet
- Measure Information Form: Release NotesDocument5 pagesMeasure Information Form: Release NotesNurses For Tobacco ControlNo ratings yet
- ClaudiaDocument21 pagesClaudiaNurses For Tobacco ControlNo ratings yet
- Measure Information Form: Release NotesDocument5 pagesMeasure Information Form: Release NotesNurses For Tobacco ControlNo ratings yet
- Standing OrdersDocument2 pagesStanding OrdersNurses For Tobacco ControlNo ratings yet
- Campaign For Tobacco Free KidsDocument1 pageCampaign For Tobacco Free KidsNurses For Tobacco ControlNo ratings yet
- PneumoniaDocument6 pagesPneumoniaNurses For Tobacco ControlNo ratings yet
- Group Counseling GuideDocument13 pagesGroup Counseling GuideNurses For Tobacco ControlNo ratings yet
- Progress Note Template For Out-Patient TreatmentDocument1 pageProgress Note Template For Out-Patient TreatmentNurses For Tobacco ControlNo ratings yet
- 5 AsDocument9 pages5 AsNurses For Tobacco ControlNo ratings yet
- Case ReportDocument22 pagesCase ReportNurses For Tobacco ControlNo ratings yet
- Janie Heath PHD, Aprn-Bc, Anp, Acnp Associate Dean Academic Nursing Practice Medical College of GeorgiaDocument41 pagesJanie Heath PHD, Aprn-Bc, Anp, Acnp Associate Dean Academic Nursing Practice Medical College of GeorgiaNurses For Tobacco ControlNo ratings yet
- Capitol Hill Caucus: Nursing Leaders For Tobacco Control: Janie Heath PHD, Aprn, Bc-Anp, AcnpDocument25 pagesCapitol Hill Caucus: Nursing Leaders For Tobacco Control: Janie Heath PHD, Aprn, Bc-Anp, AcnpNurses For Tobacco ControlNo ratings yet
- Carcinogen Exposure Part 2Document23 pagesCarcinogen Exposure Part 2Nurses For Tobacco ControlNo ratings yet
- Tobacco Cessation: Academic Partnerships For SuccessDocument48 pagesTobacco Cessation: Academic Partnerships For SuccessNurses For Tobacco ControlNo ratings yet
- Janie Heath PHD, Aprn-Bc, Anp, Acnp Associate Dean Academic Nursing Practice Medical College of GeorgiaDocument59 pagesJanie Heath PHD, Aprn-Bc, Anp, Acnp Associate Dean Academic Nursing Practice Medical College of GeorgiaNurses For Tobacco ControlNo ratings yet
- Tobacco Cessation: Essential Steps For SuccessDocument49 pagesTobacco Cessation: Essential Steps For SuccessNurses For Tobacco ControlNo ratings yet
- Tobacco Cessation: Academic Nursing Partnerships For SuccessDocument52 pagesTobacco Cessation: Academic Nursing Partnerships For SuccessNurses For Tobacco ControlNo ratings yet
- Integrating The "3 Minute" Tobacco Cessation Intervention in DAILY PracticeDocument50 pagesIntegrating The "3 Minute" Tobacco Cessation Intervention in DAILY PracticeNurses For Tobacco ControlNo ratings yet
- There's NO Safe Way To Operate A Cigarette: Seek The To Be Smoke Free!Document25 pagesThere's NO Safe Way To Operate A Cigarette: Seek The To Be Smoke Free!Nurses For Tobacco ControlNo ratings yet