Download as pdf or txt
You might also like
- Form A - OJT PDSDocument2 pagesForm A - OJT PDSjive_gumela50% (2)
- Rop Job Application With Availability - Fillable For WebsiteDocument2 pagesRop Job Application With Availability - Fillable For Websiteapi-283957827No ratings yet
- Request For Clearance Form: Surname First Middle TitleDocument2 pagesRequest For Clearance Form: Surname First Middle TitleCherrell LynchNo ratings yet
- West Main Pizza ApplicationDocument3 pagesWest Main Pizza ApplicationAimee DeLine BriggsNo ratings yet
- Patient/Client Information Form - Animal Medical ClinicDocument1 pagePatient/Client Information Form - Animal Medical ClinicArchetype ProductionsNo ratings yet
- Rop Application: Directions: Please Print LegiblyDocument2 pagesRop Application: Directions: Please Print Legiblyapi-284469921No ratings yet
- Hwghjgfjbklgjbksrthio Hgaetopjhtkop LsxexpDocument2 pagesHwghjgfjbklgjbksrthio Hgaetopjhtkop Lsxexpapi-284999187No ratings yet
- British Virgin IslandsDocument2 pagesBritish Virgin IslandsNoushin ShaikNo ratings yet
- Gopher Hole Applicationjacob GuerreroDocument3 pagesGopher Hole Applicationjacob Guerreroapi-311839096No ratings yet
- Employee Emergency Contact FormDocument1 pageEmployee Emergency Contact FormJack SmithNo ratings yet
- Biggest Looser FormDocument2 pagesBiggest Looser FormnobeauNo ratings yet
- WRV Reimbursement Form2014Document1 pageWRV Reimbursement Form2014api-308755886No ratings yet
- Attendance Card AlcarazDocument37 pagesAttendance Card AlcarazDylan Brhyce EsparagozaNo ratings yet
- Rop ApplicationDocument2 pagesRop Applicationapi-285958491No ratings yet
- DemographicsDocument1 pageDemographicslmaidlowNo ratings yet
- Membership Update FormDocument1 pageMembership Update FormTriumphNo ratings yet
- AuthorityDocument1 pageAuthorityScott BrownNo ratings yet
- Camp Application 2011Document3 pagesCamp Application 2011zactraversaNo ratings yet
- Sampaguita Elementary School Contact Tracing FormDocument1 pageSampaguita Elementary School Contact Tracing FormFilo PaitanNo ratings yet
- Philippine Crop Insurance Corporation - Livestock InsuranceDocument2 pagesPhilippine Crop Insurance Corporation - Livestock InsuranceJoselito M. BaborNo ratings yet
- Membership Form 2012Document1 pageMembership Form 2012susie6771No ratings yet
- Ugandan Professionals Network Registration Form: NameDocument1 pageUgandan Professionals Network Registration Form: NameTony Blaze KatendeNo ratings yet
- Indigo Registration Form PDFDocument5 pagesIndigo Registration Form PDFindigoairlines00001No ratings yet
- Rop Job Application With Availability - Fillable For WebsiteDocument2 pagesRop Job Application With Availability - Fillable For Websiteapi-285980844No ratings yet
- Fortunes Ihrd & Consultancy Services: Personal Bio-Data of The ApplicantDocument3 pagesFortunes Ihrd & Consultancy Services: Personal Bio-Data of The ApplicantPrameela JacobNo ratings yet
- HeroReward AppDocument2 pagesHeroReward Appmcgloen09No ratings yet
- JobapplicationDocument2 pagesJobapplicationapi-284274502No ratings yet
- Rop SeniorDocument2 pagesRop Seniorapi-285533040No ratings yet
- Matrimony - Application FormDocument1 pageMatrimony - Application FormMarian ToquireNo ratings yet
- Patient Data Form PDFDocument1 pagePatient Data Form PDFjamNo ratings yet
- WWW Muhsd k12 Ca Us Cms Lib5 Ca01001051 Centricity Domain 1016 Job ApplicationDocument2 pagesWWW Muhsd k12 Ca Us Cms Lib5 Ca01001051 Centricity Domain 1016 Job Applicationapi-253740937No ratings yet
- Employee Information Form: JMP Building 2, Aparente Street General Santos City 0922-503 - 5724Document2 pagesEmployee Information Form: JMP Building 2, Aparente Street General Santos City 0922-503 - 5724Ryan Bonsay BalolotNo ratings yet
- Information SheetDocument2 pagesInformation SheetAileenNo ratings yet
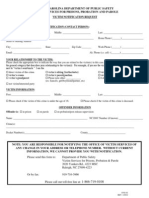
- Victim Notification Request FormDocument1 pageVictim Notification Request FormSarah Beth BreckNo ratings yet
- Rop Job Application With Availability - Fillable For WebsiteDocument2 pagesRop Job Application With Availability - Fillable For Websiteapi-284031811No ratings yet
- Pre Application - FormDocument3 pagesPre Application - Formzaman872003No ratings yet
- Job ApplicationDocument4 pagesJob Applicationapi-545948540No ratings yet
- BGT Registration FormDocument1 pageBGT Registration FormbuffalotalentNo ratings yet
- SerranoDocument2 pagesSerranoapi-285975923No ratings yet
- Authorized Persons Outside Residence (Apor) Application FormDocument1 pageAuthorized Persons Outside Residence (Apor) Application FormLadyNoreen Asis ClitarNo ratings yet
- Authorized Persons Outside Residence (Apor) Application FormDocument1 pageAuthorized Persons Outside Residence (Apor) Application FormRamnuj Orecul Soralc100% (5)
- Commendation Form ColumnsDocument1 pageCommendation Form ColumnsMark ReinhardtNo ratings yet
- Patient InformationDocument1 pagePatient Informationmikelefty0% (1)
- WaiverDocument1 pageWaiverjoyzapiladoNo ratings yet
- Passport ApplicationformDocument1 pagePassport ApplicationformJhoannamarienavarro DavidNo ratings yet
- Tafskills: Engineering Mindset SolutionsDocument2 pagesTafskills: Engineering Mindset SolutionsTHEOPHILUS ATO FLETCHERNo ratings yet
- Disclosure of Personal Information - Consent FormDocument1 pageDisclosure of Personal Information - Consent Formadds.mahmood786No ratings yet
- AMA EAST RIZAL (Allan Aguilar)Document3 pagesAMA EAST RIZAL (Allan Aguilar)arquidsNo ratings yet
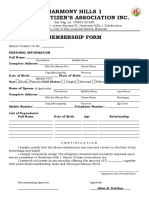
- Harmony Hills 1 Senior Citizen Association Inc Membership FormDocument2 pagesHarmony Hills 1 Senior Citizen Association Inc Membership FormRoxanne Tiffany Dotillos Sarino100% (1)
- Nomination FormDocument2 pagesNomination FormpedropierluisiNo ratings yet
- Important RemindersDocument2 pagesImportant RemindersHeathcliff Hismaña LealNo ratings yet
- Forms SBA Production 2Document2 pagesForms SBA Production 2yrvin stephensNo ratings yet
- New Patient Consultation Fax RequestDocument1 pageNew Patient Consultation Fax RequestdrschianodotcomNo ratings yet
- Humber River Hospital Consent Form To 11127 TpsDocument1 pageHumber River Hospital Consent Form To 11127 Tpsapi-676582318No ratings yet
- Barclays Funds Release FormDocument3 pagesBarclays Funds Release FormrsusyantiNo ratings yet
- High Level Play Association Recreation Subsidy Application FormDocument3 pagesHigh Level Play Association Recreation Subsidy Application Formapi-256724204No ratings yet
- Application Personal DetailsDocument3 pagesApplication Personal DetailsAddington SchoolNo ratings yet
- Microsoft Word - Application For Grant of Double Bed Room House-Application FormDocument2 pagesMicrosoft Word - Application For Grant of Double Bed Room House-Application FormHariPonnanaNo ratings yet
- Jump Stretch November 2014Document2 pagesJump Stretch November 2014jmfleckNo ratings yet
- 2014-2015 Dance ClassDocument1 page2014-2015 Dance ClassjmfleckNo ratings yet
- BCRC Dec 2014 ScheduleDocument16 pagesBCRC Dec 2014 SchedulejmfleckNo ratings yet
- Nov 2014 ScheduleDocument8 pagesNov 2014 SchedulejmfleckNo ratings yet
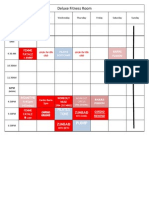
- Deluxe Fitness Nov 2014 CalendarDocument1 pageDeluxe Fitness Nov 2014 CalendarjmfleckNo ratings yet
- Youth Gymnastics Class Schedule 2014-2015: Class Ages DAY TimeDocument1 pageYouth Gymnastics Class Schedule 2014-2015: Class Ages DAY TimejmfleckNo ratings yet
- TriFold - 5KDocument2 pagesTriFold - 5KjmfleckNo ratings yet
- 2014-2015 Dance Class RegistrationDocument1 page2014-2015 Dance Class RegistrationjmfleckNo ratings yet
- Expo 2014 FormDocument1 pageExpo 2014 FormjmfleckNo ratings yet
- 5K FormDocument2 pages5K FormjmfleckNo ratings yet
- Jump Stretch August 2014Document2 pagesJump Stretch August 2014jmfleckNo ratings yet
- Gymnastics Registration 2014Document1 pageGymnastics Registration 2014jmfleckNo ratings yet
- HistoryDocument1 pageHistoryjmfleckNo ratings yet
- All Questions, Contact: Michelle Bower (724) 699-4383: 2014-2015 Dance ScheduleDocument1 pageAll Questions, Contact: Michelle Bower (724) 699-4383: 2014-2015 Dance SchedulejmfleckNo ratings yet
- Pre School CampDocument1 pagePre School CampjmfleckNo ratings yet
- SurveyDocument1 pageSurveyjmfleckNo ratings yet
- July 2014 ScheduleDocument12 pagesJuly 2014 SchedulejmfleckNo ratings yet
- 401 - Northern Route To Downtown Sharon (Monday-Friday)Document9 pages401 - Northern Route To Downtown Sharon (Monday-Friday)jmfleckNo ratings yet
- Tot Swimming Winter 2014Document1 pageTot Swimming Winter 2014jmfleckNo ratings yet
- Financial ArrangementsDocument1 pageFinancial ArrangementsjmfleckNo ratings yet