Download as pdf or txt
You might also like
- Prior Authorization Request FormDocument3 pagesPrior Authorization Request FormvanessaNo ratings yet
- New Patient Intake FormDocument6 pagesNew Patient Intake FormCraig TrujilloNo ratings yet
- Patient Information: Person Responsible For Account (If Other Than Patient)Document5 pagesPatient Information: Person Responsible For Account (If Other Than Patient)abelcooleyNo ratings yet
- Practice of Chet Gentry, MD Alison Hicks, FNP-C Tiffany Ward, FNP-BC William Wilson, FNPDocument6 pagesPractice of Chet Gentry, MD Alison Hicks, FNP-C Tiffany Ward, FNP-BC William Wilson, FNPPeyton BooherNo ratings yet
- Pet Owner SurveyDocument1 pagePet Owner Surveyapi-302018013No ratings yet
- New Patient FormDocument7 pagesNew Patient Formhamzahali039No ratings yet
- Patient FormsDocument4 pagesPatient Formsapi-203989638No ratings yet
- Officers Board of Directors: Anne Arundel County Maryland Ostomy Association, Inc. P.O. BOX 847 Gambrills, MD 21054Document8 pagesOfficers Board of Directors: Anne Arundel County Maryland Ostomy Association, Inc. P.O. BOX 847 Gambrills, MD 21054janicewinters7760No ratings yet
- 2021 New PT PPWK EditableDocument14 pages2021 New PT PPWK EditableHogla GonzalezNo ratings yet
- Registration Forms Non Breast BEPDocument8 pagesRegistration Forms Non Breast BEPvirginialordanNo ratings yet
- Officers Board of Directors: Anne Arundel County Maryland Ostomy Association, Inc. P.O. BOX 847 Gambrills, MD 21054Document8 pagesOfficers Board of Directors: Anne Arundel County Maryland Ostomy Association, Inc. P.O. BOX 847 Gambrills, MD 21054janicewinters7760No ratings yet
- APPLICATION - Adult Volunteer - 3-17 Physicians RegionalDocument12 pagesAPPLICATION - Adult Volunteer - 3-17 Physicians RegionalvikNo ratings yet
- DP New Patient Form - 2023Document5 pagesDP New Patient Form - 2023cdbn2326No ratings yet
- Donald HazzardDocument14 pagesDonald HazzardshogaibutsuNo ratings yet
- Gynemed Surgical Abortion FormsDocument17 pagesGynemed Surgical Abortion FormsLina GonzalesNo ratings yet
- Salon Client Intake FormDocument3 pagesSalon Client Intake FormholmestenishiaNo ratings yet
- Welcome PackageDocument13 pagesWelcome PackageLene HeinlenNo ratings yet
- Officers Board of Directors: Anne Arundel County Maryland Ostomy Association, Inc. P.O. BOX 847 Gambrills, MD 21054Document8 pagesOfficers Board of Directors: Anne Arundel County Maryland Ostomy Association, Inc. P.O. BOX 847 Gambrills, MD 21054janicewinters7760No ratings yet
- New Patient Information-2021Document6 pagesNew Patient Information-2021Anime300No ratings yet
- PATIENT INFORMATION - Please Fill Out CompletelyDocument5 pagesPATIENT INFORMATION - Please Fill Out CompletelynorniellarNo ratings yet
- CAMH Referral Form PDFDocument3 pagesCAMH Referral Form PDFDeisel AssisNo ratings yet
- Volunteer Application Complete 2014Document9 pagesVolunteer Application Complete 2014Arianne FosterNo ratings yet
- Officers Board of Directors: Anne Arundel County Maryland Ostomy Association, Inc. P.O. BOX 847 Gambrills, MD 21054Document8 pagesOfficers Board of Directors: Anne Arundel County Maryland Ostomy Association, Inc. P.O. BOX 847 Gambrills, MD 21054janicewinters7760No ratings yet
- Cambridge Memorial Hospital Volunteer Association Application FormDocument6 pagesCambridge Memorial Hospital Volunteer Association Application Formdaniela velascoNo ratings yet
- Patient Registration : Be Well Associates, Dan O. Harper, M.DDocument20 pagesPatient Registration : Be Well Associates, Dan O. Harper, M.DAnonymous YkfnE1No ratings yet
- Purchasing LetterDocument1 pagePurchasing LetterHannah Catherina Recato LinoNo ratings yet
- Patient Required Forms - Pasadena Cyberknife CenterDocument11 pagesPatient Required Forms - Pasadena Cyberknife CenterPasadena Cyberknife Center100% (1)
- Patient Survey QuestionnaireDocument3 pagesPatient Survey QuestionnaireVivek DasNo ratings yet
- RMT Intake Form NorthvilleDocument3 pagesRMT Intake Form Northvillehonglu.cheng.pubNo ratings yet
- Officers Board of Directors: Anne Arundel County Maryland Ostomy Association, Inc. P.O. BOX 847 Gambrills, MD 21054Document8 pagesOfficers Board of Directors: Anne Arundel County Maryland Ostomy Association, Inc. P.O. BOX 847 Gambrills, MD 21054janicewinters7760No ratings yet
- Care1st Dental DirectoryDocument137 pagesCare1st Dental DirectorytxgenicNo ratings yet
- Commitment To Care PackagesDocument4 pagesCommitment To Care PackagesJessica SimpsonNo ratings yet
- Registration - Clinics at CaumsettDocument2 pagesRegistration - Clinics at Caumsettapi-228378848No ratings yet
- Medical History FormDocument2 pagesMedical History Form2oclockNo ratings yet
- Brown Hearing Centers: Personal InformationDocument2 pagesBrown Hearing Centers: Personal InformationEddie TooheyNo ratings yet
- Retailer - Membership Application Form: YU Ntnubcabskmbonqc Nlnbns PEDocument1 pageRetailer - Membership Application Form: YU Ntnubcabskmbonqc Nlnbns PEalex metalNo ratings yet
- Payment Policies and Agreement To PayDocument5 pagesPayment Policies and Agreement To PayChristopher HartmanNo ratings yet
- Compassionate Care Network (CCN) : Application ForDocument1 pageCompassionate Care Network (CCN) : Application ForMirNo ratings yet
- Scrisoare de IntentieDocument7 pagesScrisoare de IntentieAlina ManescuNo ratings yet
- Dental WaiverDocument1 pageDental WaiverMary Grace LemonNo ratings yet
- Job Application Letter and Examples For CV EuropassDocument7 pagesJob Application Letter and Examples For CV EuropassAlina ManescuNo ratings yet
- New Patient FormDocument4 pagesNew Patient Formapi-288684181No ratings yet
- AsteraZenca Bpplication EditformDocument5 pagesAsteraZenca Bpplication Editformmjdjnk100% (1)
- Patient Form 01 (Revised Oct. 2009)Document3 pagesPatient Form 01 (Revised Oct. 2009)jtaylo49100% (1)
- Consent FormDocument2 pagesConsent FormYsabel MendrosNo ratings yet
- AesthetechDocument2 pagesAesthetechRKNo ratings yet
- Feedback EnglishDocument4 pagesFeedback Englishsreesai maternityNo ratings yet
- Name of The IndividualDocument11 pagesName of The IndividualSandeep VmNo ratings yet
- A L S I: Ssisted Iving Ervices, NCDocument2 pagesA L S I: Ssisted Iving Ervices, NCbgeyserNo ratings yet
- Knee Clinic Intake Forms 2013Document4 pagesKnee Clinic Intake Forms 2013Dr. Dale MacdonaldNo ratings yet
- Health History QuestionnaireDocument3 pagesHealth History QuestionnairejlaferriereNo ratings yet
- Adult Client Intake Forms2Document7 pagesAdult Client Intake Forms2api-310813184No ratings yet
- Inpatient Feedback Form Final (R)Document2 pagesInpatient Feedback Form Final (R)smaranikatripathyNo ratings yet
- Botox New Patient PaperworkDocument9 pagesBotox New Patient PaperworkMAI100% (1)
- SpaConsultation FormDocument1 pageSpaConsultation FormtomzaycoNo ratings yet
- What Is Next After Passing The Board ExamDocument6 pagesWhat Is Next After Passing The Board Examtimie_reyesNo ratings yet
- New Patient Package 2021 ICARE RXDocument15 pagesNew Patient Package 2021 ICARE RXAckie LoyolaNo ratings yet
- Intake Form Oct 2023Document4 pagesIntake Form Oct 2023mercerjay15No ratings yet
- Out-Patient Medical Benefits: Associates ofDocument24 pagesOut-Patient Medical Benefits: Associates ofOng Jun Xiang VarianNo ratings yet
- Jump Stretch November 2014Document2 pagesJump Stretch November 2014jmfleckNo ratings yet
- 2014-2015 Dance ClassDocument1 page2014-2015 Dance ClassjmfleckNo ratings yet
- BCRC Dec 2014 ScheduleDocument16 pagesBCRC Dec 2014 SchedulejmfleckNo ratings yet
- Nov 2014 ScheduleDocument8 pagesNov 2014 SchedulejmfleckNo ratings yet
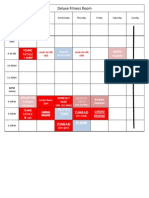
- Deluxe Fitness Nov 2014 CalendarDocument1 pageDeluxe Fitness Nov 2014 CalendarjmfleckNo ratings yet
- Youth Gymnastics Class Schedule 2014-2015: Class Ages DAY TimeDocument1 pageYouth Gymnastics Class Schedule 2014-2015: Class Ages DAY TimejmfleckNo ratings yet
- TriFold - 5KDocument2 pagesTriFold - 5KjmfleckNo ratings yet
- 2014-2015 Dance Class RegistrationDocument1 page2014-2015 Dance Class RegistrationjmfleckNo ratings yet
- Expo 2014 FormDocument1 pageExpo 2014 FormjmfleckNo ratings yet
- 5K FormDocument2 pages5K FormjmfleckNo ratings yet
- Jump Stretch August 2014Document2 pagesJump Stretch August 2014jmfleckNo ratings yet
- Gymnastics Registration 2014Document1 pageGymnastics Registration 2014jmfleckNo ratings yet
- HistoryDocument1 pageHistoryjmfleckNo ratings yet
- All Questions, Contact: Michelle Bower (724) 699-4383: 2014-2015 Dance ScheduleDocument1 pageAll Questions, Contact: Michelle Bower (724) 699-4383: 2014-2015 Dance SchedulejmfleckNo ratings yet
- Pre School CampDocument1 pagePre School CampjmfleckNo ratings yet
- IntakeDocument1 pageIntakejmfleckNo ratings yet
- July 2014 ScheduleDocument12 pagesJuly 2014 SchedulejmfleckNo ratings yet
- 401 - Northern Route To Downtown Sharon (Monday-Friday)Document9 pages401 - Northern Route To Downtown Sharon (Monday-Friday)jmfleckNo ratings yet
- Tot Swimming Winter 2014Document1 pageTot Swimming Winter 2014jmfleckNo ratings yet
- Financial ArrangementsDocument1 pageFinancial ArrangementsjmfleckNo ratings yet