Download as pdf or txt
You might also like
- Public Health Nursing: Scope and Standards of PracticeFrom EverandPublic Health Nursing: Scope and Standards of PracticeRating: 5 out of 5 stars5/5 (1)
- Evidence Based Practive 2006Document15 pagesEvidence Based Practive 2006Bolo GanNo ratings yet
- Best Practices For Mixed Methods ResearchDocument39 pagesBest Practices For Mixed Methods Researchscribd104444No ratings yet
- Evidence-Based Nursing Practice For Health Promotion in Adults With Hypertension: A Literature ReviewDocument19 pagesEvidence-Based Nursing Practice For Health Promotion in Adults With Hypertension: A Literature ReviewYusvita WaliaNo ratings yet
- Evidence-Based Nursing Practice For Health Promotion in Adults With Hypertension: A Literature ReviewDocument38 pagesEvidence-Based Nursing Practice For Health Promotion in Adults With Hypertension: A Literature Reviewmarisa isahNo ratings yet
- Conjoint in HEALTH ResearchDocument17 pagesConjoint in HEALTH ResearchDiana Tan May KimNo ratings yet
- 8-2 Health Services Research Translating Research Into PolicyDocument39 pages8-2 Health Services Research Translating Research Into PolicyFady Jehad ZabenNo ratings yet
- Primary Health Care Literature ReviewDocument4 pagesPrimary Health Care Literature Reviewafdtbluwq100% (1)
- Session 7Document76 pagesSession 7priyanshiraichada15No ratings yet
- America's Healthcare Transformation: Strategies and InnovationsFrom EverandAmerica's Healthcare Transformation: Strategies and InnovationsNo ratings yet
- Peer-Reviewed Example PaperDocument4 pagesPeer-Reviewed Example PaperEunique NoelNo ratings yet
- Ramseier Et Al-2015-Journal of Clinical Periodontology PDFDocument12 pagesRamseier Et Al-2015-Journal of Clinical Periodontology PDFChristine HacheNo ratings yet
- Health Service Research An Evolving Definition of The FieldDocument3 pagesHealth Service Research An Evolving Definition of The FieldSamNo ratings yet
- A Framework To Measure The Impact of Investments in Health ResearchDocument16 pagesA Framework To Measure The Impact of Investments in Health ResearchGesler Pilvan SainNo ratings yet
- What Is Health Services ResearchDocument5 pagesWhat Is Health Services ResearchClara Bermúdez TamayoNo ratings yet
- Quality Improvement ModelsDocument64 pagesQuality Improvement ModelsShahin Patowary100% (2)
- The Integration of Primary Health Care Services A Systematic Literature ReviewDocument5 pagesThe Integration of Primary Health Care Services A Systematic Literature ReviewrdssibwgfNo ratings yet
- Sdi 5294 KumarDocument20 pagesSdi 5294 KumarBharatKumarMaheshwariNo ratings yet
- Patient CenteredDocument12 pagesPatient CenteredNina NaguyevskayaNo ratings yet
- 2012 Bigbee Models PHNDocument11 pages2012 Bigbee Models PHNJulia Dewi Eka GunawatiNo ratings yet
- Public Health Dissertation TitlesDocument7 pagesPublic Health Dissertation TitlesWriteMyPaperPleaseSingapore100% (1)
- Closing The Quality Gap-A Critical Analysis of Quality Improvement StrategiesDocument206 pagesClosing The Quality Gap-A Critical Analysis of Quality Improvement Strategiesturbina155No ratings yet
- Faber - Public Reporting in Health CareDocument8 pagesFaber - Public Reporting in Health CareDaniel Rico FuentesNo ratings yet
- HLRP 0220 CudjoeDocument24 pagesHLRP 0220 CudjoeaaanzaniiNo ratings yet
- Quality Indicators For Primary Health Care A Systematic Literature ReviewDocument10 pagesQuality Indicators For Primary Health Care A Systematic Literature ReviewafdtygyhkNo ratings yet
- Journal Reading MavDocument2 pagesJournal Reading MavCuttie Anne GalangNo ratings yet
- Mr. Hariom Rajput Mr. Ramsingh Ji Gmail-ID International Association of Oncology (IAO) Government of IndiaDocument6 pagesMr. Hariom Rajput Mr. Ramsingh Ji Gmail-ID International Association of Oncology (IAO) Government of IndiaHariom RajputNo ratings yet
- Perceptions of The Professional Pharmacy Services in A Major Canadian Hospital: A Comparison of Stakeholder GroupsDocument12 pagesPerceptions of The Professional Pharmacy Services in A Major Canadian Hospital: A Comparison of Stakeholder GroupsGracia GiasiNo ratings yet
- Intergrative Review Final DraftDocument22 pagesIntergrative Review Final Draftapi-432119884No ratings yet
- Guide To Patient and Family Engagement: Environmental Scan ReportDocument100 pagesGuide To Patient and Family Engagement: Environmental Scan ReportjustdoyourNo ratings yet
- 0rder 343 NRS-493-ASSIGNMENT 3 Literature ReviewDocument6 pages0rder 343 NRS-493-ASSIGNMENT 3 Literature Reviewjoshua chegeNo ratings yet
- Evidence-Based Health Policy: A Preliminary Systematic ReviewDocument5 pagesEvidence-Based Health Policy: A Preliminary Systematic ReviewAndre LanzerNo ratings yet
- Quality of Healthcare Services Rural IndiaDocument10 pagesQuality of Healthcare Services Rural IndiaPradeep BishtNo ratings yet
- Health Care Quality Assessment: Michael A. Counte, PH.DDocument30 pagesHealth Care Quality Assessment: Michael A. Counte, PH.DAnonymous TO9fMjNo ratings yet
- Measuring Oral Health and Quality of LifeDocument172 pagesMeasuring Oral Health and Quality of LifeCalin Dragoman100% (1)
- Models For Individual Oral Health Promotion and Their Effectiveness: A Systematic ReviewDocument8 pagesModels For Individual Oral Health Promotion and Their Effectiveness: A Systematic ReviewMonica Agustine HartonoNo ratings yet
- C Truong, M., Paradies, Y. & Priest, N. (2014Document17 pagesC Truong, M., Paradies, Y. & Priest, N. (2014Ign EcheverríaNo ratings yet
- Sabitha PROJECT SYNOPSISDocument4 pagesSabitha PROJECT SYNOPSISJohn MohanNo ratings yet
- Journal Reading ReportDocument2 pagesJournal Reading ReportCuttie Anne GalangNo ratings yet
- Critical Appraisal For Public Health: A New ChecklistDocument7 pagesCritical Appraisal For Public Health: A New Checklistkristina dewiNo ratings yet
- Literature Review Developing Competencies For Health Promotion Deliverable 3bDocument10 pagesLiterature Review Developing Competencies For Health Promotion Deliverable 3bxfeivdsifNo ratings yet
- Systematic Literature Review of Oral HygieneDocument52 pagesSystematic Literature Review of Oral HygieneAnkit Kothiyal0% (1)
- Evidence Based Practice in Nursing BinuDocument51 pagesEvidence Based Practice in Nursing BinuBinu Joshva100% (3)
- 1 - 4 Quality of CareDocument10 pages1 - 4 Quality of CareRaul Gascueña100% (1)
- How Can Clinical Epidemiology Better Support Evidence-Based Guidelines and Policies in Low-Income CountriesDocument3 pagesHow Can Clinical Epidemiology Better Support Evidence-Based Guidelines and Policies in Low-Income CountriesEko Wahyu AgustinNo ratings yet
- SAGE Open Medicine 2: 2050312114522618 © The Author(s) 2014 A Qualitative Study of Conceptual and Operational Definitions For Leaders inDocument21 pagesSAGE Open Medicine 2: 2050312114522618 © The Author(s) 2014 A Qualitative Study of Conceptual and Operational Definitions For Leaders inascarolineeNo ratings yet
- Patient Engagement in Research: A Systematic Review: Researcharticle Open AccessDocument9 pagesPatient Engagement in Research: A Systematic Review: Researcharticle Open Accessv_ratNo ratings yet
- Effects of Worksite Health Promotion Interventions On Employee Diets: A Systematic ReviewDocument7 pagesEffects of Worksite Health Promotion Interventions On Employee Diets: A Systematic ReviewUtami LukitaNo ratings yet
- Integrative Health Care Shift Benefits and Challenges Among Health Care ProfessionalsDocument4 pagesIntegrative Health Care Shift Benefits and Challenges Among Health Care ProfessionalsEditor IJTSRDNo ratings yet
- Health Seeking BehaviourDocument27 pagesHealth Seeking BehaviourRommel IrabagonNo ratings yet
- Taxonomia BCWDocument216 pagesTaxonomia BCWMae SilvaNo ratings yet
- Nursing ResearchDocument15 pagesNursing Researchsubhashreepal13No ratings yet
- HLTH 520 Reseach Appraisal - ResearchDocument16 pagesHLTH 520 Reseach Appraisal - Researchapi-479186899No ratings yet
- Summary ResearchDocument6 pagesSummary ResearchLance SilvaNo ratings yet
- Ahrq DissertationDocument4 pagesAhrq Dissertationsupnilante1980100% (1)
- Writing The Proposal For A Qualitative Research Methodology ProjectDocument41 pagesWriting The Proposal For A Qualitative Research Methodology Projectrcaba100% (1)
- Psychiatry Research: Alison B. Hamilton, Erin P. Finley TDocument8 pagesPsychiatry Research: Alison B. Hamilton, Erin P. Finley TEloisa Garcia AñinoNo ratings yet
- Plos Medicine /Article/Crossref/I /Article/Tw Itter/Info /Article/Metrics/Inf Info:Doi/10.1371/J Patient Adher 1185260400000Document25 pagesPlos Medicine /Article/Crossref/I /Article/Tw Itter/Info /Article/Metrics/Inf Info:Doi/10.1371/J Patient Adher 1185260400000khattak_i89No ratings yet
- Accelerating Medical Evidence Generation and Use: Summary of a Meeting SeriesFrom EverandAccelerating Medical Evidence Generation and Use: Summary of a Meeting SeriesNo ratings yet
- Cahn&Polich - 06 Meditation States and Traits ReviewDocument33 pagesCahn&Polich - 06 Meditation States and Traits ReviewfiseradaNo ratings yet
- Membertou Family Homes Law Fact SheetDocument2 pagesMembertou Family Homes Law Fact SheetfiseradaNo ratings yet
- Cultural Sensitivity and Adaptation in Family Based Prevention InterventionsDocument6 pagesCultural Sensitivity and Adaptation in Family Based Prevention Interventionsfiserada100% (1)
- Shojin Ryori Culinary Fundamentals in Zen PDFDocument1 pageShojin Ryori Culinary Fundamentals in Zen PDFfiseradaNo ratings yet
- Tsung-Mi and The Single Word "Awareness" (Chih) by Peter GregoryDocument20 pagesTsung-Mi and The Single Word "Awareness" (Chih) by Peter GregoryfiseradaNo ratings yet
- Diagnostic Systematic Reviews Road Map V3Document2 pagesDiagnostic Systematic Reviews Road Map V3fiseradaNo ratings yet
- Large SystemsDocument220 pagesLarge SystemsfiseradaNo ratings yet
- Making Outcome Mapping WorkDocument79 pagesMaking Outcome Mapping WorkfiseradaNo ratings yet
- How Far Can Q-Analysis Go Into Social Systems Understanding ?Document10 pagesHow Far Can Q-Analysis Go Into Social Systems Understanding ?fiseradaNo ratings yet
- Innovation in Instrument DesignDocument28 pagesInnovation in Instrument DesignfiseradaNo ratings yet
- Diavik Fact BookDocument20 pagesDiavik Fact BookfiseradaNo ratings yet
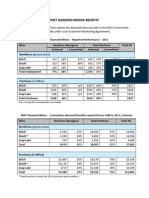
- NWT Diamond Mining Benefits: N/a - No Specific Commitments Were MadeDocument2 pagesNWT Diamond Mining Benefits: N/a - No Specific Commitments Were MadefiseradaNo ratings yet
- Economic Resilience To DisastersDocument59 pagesEconomic Resilience To DisastersfiseradaNo ratings yet
- Biblical Hebrew A Text and WorkbookDocument451 pagesBiblical Hebrew A Text and Workbookannegh100% (4)