Download as doc, pdf, or txt
You might also like
- Chapter 12 Drugs and The Autonomic Nervous System PDFDocument10 pagesChapter 12 Drugs and The Autonomic Nervous System PDFMaha KhanNo ratings yet
- Medical Pharmacology Ovidius 2014 1st TestDocument19 pagesMedical Pharmacology Ovidius 2014 1st TestWissam DadiNo ratings yet
- Autonomic Nervous System PharmacologyDocument13 pagesAutonomic Nervous System PharmacologySam BotNo ratings yet
- Autonomic Nervous System PharmacologyDocument7 pagesAutonomic Nervous System Pharmacologydonordarah93No ratings yet
- Chapter 2 230327072253 9bf1fc09Document23 pagesChapter 2 230327072253 9bf1fc09parmarkeval1610No ratings yet
- Adrenergic Agonists and AntagonistsDocument9 pagesAdrenergic Agonists and Antagonistsstephanienwafor18No ratings yet
- Assignment On Adrenergic ReceptorDocument13 pagesAssignment On Adrenergic ReceptoryannaingNo ratings yet
- Neuropathophysiology I Synaptic Transmission and What Can Go WrongDocument12 pagesNeuropathophysiology I Synaptic Transmission and What Can Go Wrongmaestrojedi33No ratings yet
- Al-Bayan University Pharmacy College 3 Stage Pharmacy: 5 Drugs Acting On ANS DR - Khulood SaadoonDocument42 pagesAl-Bayan University Pharmacy College 3 Stage Pharmacy: 5 Drugs Acting On ANS DR - Khulood SaadoonAsdar LeaqerNo ratings yet
- Cholinergic DrugsDocument44 pagesCholinergic DrugsJohn MahiyaNo ratings yet
- Inotropic Agents: Submitted ToDocument87 pagesInotropic Agents: Submitted Toraman kumariNo ratings yet
- Adrenergic Agonists 1Document90 pagesAdrenergic Agonists 1OMAR NASSERNo ratings yet
- Subject: Pharmacology Topic: ANS 2 Lecturer: Maria Luisa D. Delacruz, M.D. Date of Lecture:August 3, 2011 Transcriptionist: Anonymous Pages: 16Document16 pagesSubject: Pharmacology Topic: ANS 2 Lecturer: Maria Luisa D. Delacruz, M.D. Date of Lecture:August 3, 2011 Transcriptionist: Anonymous Pages: 16dtimtimanNo ratings yet
- SympathomimeticsDocument25 pagesSympathomimeticsMirza Shaharyar BaigNo ratings yet
- HPHY 225 Assignment - FinalDocument5 pagesHPHY 225 Assignment - FinalSylvester MathiasNo ratings yet
- PCOL CHP 4-6 (Situational Analysis)Document2 pagesPCOL CHP 4-6 (Situational Analysis)Sunshine_Bacla_4275No ratings yet
- Cardiovascular Pharmacology PDFDocument20 pagesCardiovascular Pharmacology PDFMelanie PrinceNo ratings yet
- Camille I BSM 3 Phama Midterm ActivityDocument8 pagesCamille I BSM 3 Phama Midterm ActivityJanine VegaNo ratings yet
- Table of NeurotransmittersDocument10 pagesTable of NeurotransmittersAmanda Shabrina PutriNo ratings yet
- PHARMACOLOGY of ANS (Synopsis For Students)Document16 pagesPHARMACOLOGY of ANS (Synopsis For Students)JIEHASMARTNo ratings yet
- Jelie Rose BSM 3 Phama Midterm ActivityDocument8 pagesJelie Rose BSM 3 Phama Midterm ActivityJanine VegaNo ratings yet
- Chapter 2 PharmacologyDocument18 pagesChapter 2 Pharmacologynikhilkhatker2020No ratings yet
- Skeletal Muscle RelaxantDocument18 pagesSkeletal Muscle Relaxantswaroop ranjan nandaNo ratings yet
- Pharmacology Table For Cardiovascular LectureDocument10 pagesPharmacology Table For Cardiovascular LecturemuhammadridhwanNo ratings yet
- Soal AnfismanDocument5 pagesSoal AnfismanDike IrvaniNo ratings yet
- Tutorial On ANS PharmacologyDocument23 pagesTutorial On ANS PharmacologyRomaine-Ricardo FrancisNo ratings yet
- Practical Guidance Introduction of The PracticalDocument4 pagesPractical Guidance Introduction of The PracticalNella Rosyalina DamayantiNo ratings yet
- Autonomic Nervous System PharmacologyDocument97 pagesAutonomic Nervous System PharmacologyKarun Kumar Shingari100% (1)
- CristineBSM 3 Phama Midterm ActivityDocument7 pagesCristineBSM 3 Phama Midterm ActivityJanine VegaNo ratings yet
- Antagonis KolinergikDocument49 pagesAntagonis KolinergikGde Ananda ArmanditaNo ratings yet
- L19 - Adrenergic IVDocument7 pagesL19 - Adrenergic IVyasaira707No ratings yet
- First Page PDFDocument1 pageFirst Page PDFferhanmu419No ratings yet
- The Cholinergic Antagonists: PharmacologyDocument5 pagesThe Cholinergic Antagonists: PharmacologyDr-Dalya ShakirNo ratings yet
- 08 Autonomic Nervous SystemDocument0 pages08 Autonomic Nervous SystemjuniorebindaNo ratings yet
- Adrenergic PharmacologyDocument17 pagesAdrenergic PharmacologyCatNo ratings yet
- Autonomic DrugsDocument2 pagesAutonomic DrugsDouglas Greg CookNo ratings yet
- Anticholinergic AgentsDocument36 pagesAnticholinergic AgentsNicole GalvezNo ratings yet
- ANS Dan FD Gizi 2012Document31 pagesANS Dan FD Gizi 2012indahNo ratings yet
- Intro To Pharmacology Study GuideDocument93 pagesIntro To Pharmacology Study GuideMichelle Morgan LongstrethNo ratings yet
- Selfassessment QuestionsPharmBasicsDocument7 pagesSelfassessment QuestionsPharmBasicsTsukikage12No ratings yet
- Ans 7 Local Anaesthetic AgentDocument40 pagesAns 7 Local Anaesthetic Agentyounas63No ratings yet
- Cholinergic ReceptorsDocument67 pagesCholinergic ReceptorsShynne RPhNo ratings yet
- Pharmacology Test 1Document39 pagesPharmacology Test 1Niki BolinNo ratings yet
- Nervous SystemDocument12 pagesNervous Systemjanelle asiongNo ratings yet
- Lec 16Document3 pagesLec 16Abdullahayad farouqNo ratings yet
- Cholinoceptor AntagonistDocument21 pagesCholinoceptor Antagonistraafat mohammedNo ratings yet
- Pharmacology: Drugs Acting On The Autonomic Nervous SystemDocument9 pagesPharmacology: Drugs Acting On The Autonomic Nervous SystemShun Reigh SumilangNo ratings yet
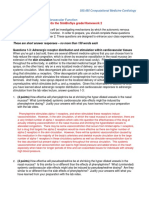
- Total Point Value: 20 Towards The Simbiosys Grade/Homework 2Document6 pagesTotal Point Value: 20 Towards The Simbiosys Grade/Homework 2Katia KovalenkaNo ratings yet
- Allergy - October 1980 - NornDocument9 pagesAllergy - October 1980 - NornGloria Stefani TeniwutNo ratings yet
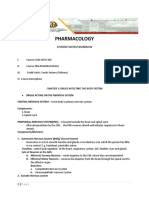
- Pharmacology: Students Notes/ WorkbookDocument50 pagesPharmacology: Students Notes/ WorkbookPABLO, JACKSON P.No ratings yet
- Type of Neurotransmitter, Synthesis-Activation-Termination and Comparison Between Normal and DisorderDocument9 pagesType of Neurotransmitter, Synthesis-Activation-Termination and Comparison Between Normal and DisorderNehasish SahuNo ratings yet
- Pharma Script 5Document12 pagesPharma Script 5Hashim GhazoNo ratings yet
- Cardiac PharmacologyDocument23 pagesCardiac PharmacologyRavi Kant IyerNo ratings yet
- Autonomic Nervous System - 2Document45 pagesAutonomic Nervous System - 2salahnwsNo ratings yet
- L17 - Adrenergics IIDocument6 pagesL17 - Adrenergics IIyasaira707No ratings yet
- Pharm Assign 3Document7 pagesPharm Assign 3mjamie12345No ratings yet
- Pharm QuestionsDocument5 pagesPharm Questionsvaroon525No ratings yet
- Lec #10 Introduction To CNS Pharmacology: 1. Voltage-GatedDocument13 pagesLec #10 Introduction To CNS Pharmacology: 1. Voltage-GatedAya ShahrouriNo ratings yet