Download as docx, pdf, or txt
You might also like
- Employment Job ApplicationDocument4 pagesEmployment Job Applicationapi-294681692No ratings yet
- Pest Analysis of Bata PakistanDocument5 pagesPest Analysis of Bata PakistanOsama ButtNo ratings yet
- Taking Anthropometric MeasurementsDocument8 pagesTaking Anthropometric MeasurementsRaja Kumar100% (6)
- Eng102 Fallacy HandoutsDocument2 pagesEng102 Fallacy Handoutsjeanninestanko0% (1)
- New Leave Form ADocument1 pageNew Leave Form ASaadat AliNo ratings yet
- Leave Application FormDocument1 pageLeave Application FormBasir Usman100% (1)
- Casual Leave Application Form District Government JhangDocument1 pageCasual Leave Application Form District Government Jhangamir100% (1)
- Leave Application FormDocument2 pagesLeave Application Formfahadahmad111111No ratings yet
- Leave Application Form: Employee DetailsDocument1 pageLeave Application Form: Employee DetailsMsKhan0078No ratings yet
- Staff Leave Application Form: DateDocument1 pageStaff Leave Application Form: Datemichael cheeNo ratings yet
- Leave Application FormDocument1 pageLeave Application FormMuhammad Arfat YameenNo ratings yet
- Description: Tags: Ann982bDocument2 pagesDescription: Tags: Ann982banon-842073No ratings yet
- Leave Form SimpleDocument1 pageLeave Form SimpleZulqarnain ZiaNo ratings yet
- Leave FormDocument1 pageLeave FormbkgboqdraftsmanNo ratings yet
- LeaveDocument1 pageLeaveCASADIQUENo ratings yet
- University of Management and Technology: Leave Application FormDocument1 pageUniversity of Management and Technology: Leave Application FormAnonymous Sr1L35Ye4No ratings yet
- Hirtii Angajare OshawaDocument1 pageHirtii Angajare Oshawahutira1decembrieNo ratings yet
- Emergency Student Release Form p46Document1 pageEmergency Student Release Form p46Rhem Rick CorpuzNo ratings yet
- BDB Job Application Form PDFDocument4 pagesBDB Job Application Form PDFpema dekiNo ratings yet
- Leave ApplicationDocument1 pageLeave ApplicationFaraz Anwar AbroNo ratings yet
- Louisiana Standing Order Change Request FormDocument1 pageLouisiana Standing Order Change Request FormkdlkfaNo ratings yet
- AG Leave FormDocument1 pageAG Leave FormWolf PixelNo ratings yet
- Payroll Enrolment FormDocument1 pagePayroll Enrolment FormDarakasi InternationalNo ratings yet
- Clinical Information Services Authorization For Disclosure ofDocument2 pagesClinical Information Services Authorization For Disclosure ofRIchard RobertsNo ratings yet
- Faisalabad Medical University Faisalabad: Application Form For Faculty (For Appointing On Contract/Adhoc Basis)Document1 pageFaisalabad Medical University Faisalabad: Application Form For Faculty (For Appointing On Contract/Adhoc Basis)Rabie TahirNo ratings yet
- Leave Application Form: To Be Filled by Applicant (A)Document1 pageLeave Application Form: To Be Filled by Applicant (A)Omair Abbas100% (4)
- Co NameDocument1 pageCo NameAlisha ZaidiNo ratings yet
- JBSL Leave Application Form - 1Document1 pageJBSL Leave Application Form - 1Waleed ButtNo ratings yet
- 210 050 ReportForm TyphoidDocument7 pages210 050 ReportForm TyphoidSaurabh NainNo ratings yet
- New Student Registration FormDocument1 pageNew Student Registration FormleeNo ratings yet
- Leave LetterDocument1 pageLeave LetterPrabina kumar SahuNo ratings yet
- General Scholarship Application Form: First LastDocument3 pagesGeneral Scholarship Application Form: First LastKen BiNo ratings yet
- Casual Leave Application Form For InchargesDocument1 pageCasual Leave Application Form For InchargesZubair HussainNo ratings yet
- Employment Application Form 09Document3 pagesEmployment Application Form 09api-19987040No ratings yet
- Leave FormDocument1 pageLeave FormSohail BahadurNo ratings yet
- Emergency Loan Form 2018Document1 pageEmergency Loan Form 2018Jansen TanNo ratings yet
- Sick Leave Application FormDocument2 pagesSick Leave Application FormEmerald MedranoNo ratings yet
- Application Form: FSL, 18 Waldstock Road, London, SE28 8SF Section 1Document5 pagesApplication Form: FSL, 18 Waldstock Road, London, SE28 8SF Section 1Niaz KhanNo ratings yet
- RX Incident Report FormDocument2 pagesRX Incident Report FormArthur KrichevskyNo ratings yet
- Student Registration Form - Sample: (Institute Name)Document1 pageStudent Registration Form - Sample: (Institute Name)shweta vermaNo ratings yet
- Application For Program EntryDocument6 pagesApplication For Program EntryAngela FrizellNo ratings yet
- XregDocument1 pageXregntyt4qzdpxNo ratings yet
- Leave FormDocument2 pagesLeave FormKyaw Myo HtetNo ratings yet
- Leave Application Form WriteableDocument1 pageLeave Application Form WriteableBilly Eres100% (1)
- Leave Application Form For EmployeeDocument2 pagesLeave Application Form For EmployeeEmerald MedranoNo ratings yet
- PESFA Application FormDocument1 pagePESFA Application FormIDesign CebuNo ratings yet
- Draft Pro Forma: For Development of Your Health Service's Own PolicyDocument2 pagesDraft Pro Forma: For Development of Your Health Service's Own PolicyOlaitan MayNo ratings yet
- New Patient Forms PacketDocument4 pagesNew Patient Forms PacketCarrboro Family MedicineNo ratings yet
- KZN COGTA Bursary Application Form 2024Document7 pagesKZN COGTA Bursary Application Form 2024thabisileNo ratings yet
- Peace Corps PC-440P Notice of Volunteer or Trainee Action PostDocument1 pagePeace Corps PC-440P Notice of Volunteer or Trainee Action PostAccessible Journal Media: Peace Corps DocumentsNo ratings yet
- Hrmis FormDocument5 pagesHrmis FormMuhammad Nasir Rao40% (5)
- Target Job Application Form PrintableDocument5 pagesTarget Job Application Form PrintableDom HilliardNo ratings yet
- Full and Final Form - GeniusDocument3 pagesFull and Final Form - GeniusHrishikesh.0% (1)
- Dube Trade Port Application FormDocument7 pagesDube Trade Port Application FormNcediswaNo ratings yet
- Leave Form PDFDocument1 pageLeave Form PDFsubhasriNo ratings yet
- Volunteer Application Form: Please Read Below and SignDocument1 pageVolunteer Application Form: Please Read Below and SignLisaMarieNo ratings yet
- FHR01 - Employee Requisition FormDocument1 pageFHR01 - Employee Requisition Formangelicaa.atanozaNo ratings yet
- Borang Permohonan Cuti Clinic & PharmacyDocument1 pageBorang Permohonan Cuti Clinic & PharmacyectoclinicNo ratings yet
- Application FormsDocument2 pagesApplication Formsadisontakke7777No ratings yet
- MPC Member AppDocument3 pagesMPC Member Appdee6665No ratings yet
- Iowa Statewide Universal Practitioner Credentialing Application (PDFDrive)Document26 pagesIowa Statewide Universal Practitioner Credentialing Application (PDFDrive)marko.sokolovski84No ratings yet
- Personal Profile FormDocument6 pagesPersonal Profile FormSwapnil KhadeNo ratings yet
- Performance ManagementDocument29 pagesPerformance ManagementOsama Butt100% (1)
- PestDocument9 pagesPestOsama ButtNo ratings yet
- The Secrets To Successful Strategy ExecutionDocument3 pagesThe Secrets To Successful Strategy ExecutionOsama ButtNo ratings yet
- Ethernet Transport Over PDH Networks With Virtual Concatenation TutorialDocument15 pagesEthernet Transport Over PDH Networks With Virtual Concatenation TutorialAnovar_ebooksNo ratings yet
- Weather and ClimateDocument2 pagesWeather and ClimateLouise GermaineNo ratings yet
- Erp Case StudyDocument2 pagesErp Case StudymehakNo ratings yet
- 2.7 2012 Influence of Implant Neck Design and Implant-Abutment Connection Type On Peri-Implant Health. Radiological StudyDocument9 pages2.7 2012 Influence of Implant Neck Design and Implant-Abutment Connection Type On Peri-Implant Health. Radiological StudyDuilioJrNo ratings yet
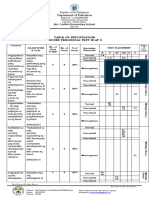
- SECOND Periodic Test in AP 4 With TOS SY 2022 2023Document6 pagesSECOND Periodic Test in AP 4 With TOS SY 2022 2023MICHAEL VERINANo ratings yet
- PNR Metro Commuter PDFDocument5 pagesPNR Metro Commuter PDFABCDNo ratings yet
- QuestionsDocument20 pagesQuestionsmaheshNo ratings yet
- Cttplus HandbookDocument36 pagesCttplus HandbookgcarreongNo ratings yet
- Tomlinson - What Was The Third WorldDocument16 pagesTomlinson - What Was The Third WorldMaría Camila Valbuena LondoñoNo ratings yet
- Vent-O-Mat - Nozzle Check ValveDocument8 pagesVent-O-Mat - Nozzle Check Valvefrankz89No ratings yet
- Actividad Integradora 6. Opening Ceremony Name: Mariela Pérez Pardiño Adviser: Cristina Peña Rodriguez Group: M7C1G32-017 Date: 29/05/2022Document3 pagesActividad Integradora 6. Opening Ceremony Name: Mariela Pérez Pardiño Adviser: Cristina Peña Rodriguez Group: M7C1G32-017 Date: 29/05/2022marielaNo ratings yet
- CAAP Telephone Public Directory PDFDocument4 pagesCAAP Telephone Public Directory PDFMaria Angelica Rodriguez AlonsoNo ratings yet
- 501a 17 PDFDocument28 pages501a 17 PDFhikary2.032100% (1)
- Role of Critical Care NursingDocument8 pagesRole of Critical Care NursingHari Mas KuncoroNo ratings yet
- Malhotra, Garg, and Rai - Analysing The NDHM Health Data Management PolicyDocument30 pagesMalhotra, Garg, and Rai - Analysing The NDHM Health Data Management Policysimran sabharwalNo ratings yet
- Full Chapter Nitride Semiconductor Light Emitting Diodes Leds Materials Technologies and Applications Woodhead Publishing Series in Electronic and Optical Materials 1St Edition Huang PDFDocument54 pagesFull Chapter Nitride Semiconductor Light Emitting Diodes Leds Materials Technologies and Applications Woodhead Publishing Series in Electronic and Optical Materials 1St Edition Huang PDFwilliam.laudenslager880100% (6)
- 1-2 JuneDocument46 pages1-2 JuneAbhinav JainNo ratings yet
- Lesson 2: Cultural and Sociopolitical EvolutionDocument7 pagesLesson 2: Cultural and Sociopolitical EvolutionAmanda FlowerNo ratings yet
- Jsu PT3 ENGLISHDocument2 pagesJsu PT3 ENGLISHDineswari SelvamNo ratings yet
- Otis Software Basic DataDocument23 pagesOtis Software Basic Datanr1wolf_co_6952990682% (17)
- Indotech Power Transformers BrochureDocument2 pagesIndotech Power Transformers BrochurenmanjNo ratings yet
- ESP Lesson Plan Argumentation and DebateDocument4 pagesESP Lesson Plan Argumentation and DebateAJ Cruz AzoresNo ratings yet
- ART300Document45 pagesART300Gerlyn OrdonioNo ratings yet
- Values Development: Lesson IiDocument15 pagesValues Development: Lesson IiSheena Clata67% (3)
- Sem 1 QP Chart Work Paper A Prelim Nov 2019 With SolutionDocument4 pagesSem 1 QP Chart Work Paper A Prelim Nov 2019 With SolutionASHISH KUMAR SAHUNo ratings yet
- Lead Acid BatteryDocument23 pagesLead Acid BatteryBrahmpal BhardwajNo ratings yet
- Economics:Presentation On Law of Equi Marginal Utility...Document11 pagesEconomics:Presentation On Law of Equi Marginal Utility...vinay rakshithNo ratings yet
- Cpim BrochureDocument4 pagesCpim BrochureMuhammadNo ratings yet