Professional Documents
Culture Documents
Pediatrics 2010 Spee E651 69
Pediatrics 2010 Spee E651 69
Uploaded by
ivanhariachandraOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Pediatrics 2010 Spee E651 69
Pediatrics 2010 Spee E651 69
Uploaded by
ivanhariachandraCopyright:
Available Formats
DOI: 10.1542/peds.
2010-0941
; originally published online February 15, 2010; 2010;125;e651 Pediatrics
Marjolein Y. Berger
Leo A. A. Spee, Marieke B. Madderom, Maaike Pijpers, Yvonne van Leeuwen and
Children
and Gastrointestinal Symptoms in Helicobacter pylori Association Between
http://pediatrics.aappublications.org/content/125/3/e651.full.html
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Boulevard, Elk Grove Village, Illinois, 60007. Copyright 2010 by the American Academy
published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point
publication, it has been published continuously since 1948. PEDIATRICS is owned,
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
Association Between Helicobacter pylori and
Gastrointestinal Symptoms in Children
abstract
OBJECTIVE: Recurrent abdominal pain (RAP) and other gastrointesti-
nal (GI) symptoms are common complaints among children. The role of
Helicobacter pylori in the cause of these complaints remains contro-
versial. Nevertheless, there is an increasing pressure on primary care
clinicians to screen for H pylori infection in symptomatic children. We
systematically reviewed the published evidence for an association be-
tween H pylori infection and GI symptoms in children.
METHODS: Medline and Embase databases up to July 2009 were
searched to identify studies that evaluated the association between
H pylori and GI symptoms in children aged up to 18 years. When studies
reported on abdominal pain without additional denition, thus not
fullling Apleys criteria, we grouped these outcomes as unspecied
abdominal pain (UAP). Methodologic quality was scored by using a
standardized list of criteria, and crude odds ratios (ORs) with 95%
condence intervals (CIs) were calculated and pooled.
RESULTS: Thirty-eight studies met our inclusion criteria: 23 case-
control studies, 14 cross-sectional studies, and 1 prospective cohort
study. The overall methodologic quality was low. Pooled ORs for the
association between RAP and H pylori infection in children were 1.21
(95% CI: 0.821.78) in 12 case-control studies and 1.00 (95% CI: 0.76
1.31) in 7 cross-sectional studies. Meta-analysis of the association be-
tween UAP and H pylori infection in 6 hospital-based studies resulted in
a pooled OR of 2.87 (95% CI: 1.625.09) compared with 0.99 (95% CI:
0.462.11) in 5 population-based studies. Two of 3 studies concerning
epigastric pain reported a statistically signicant positive association
with H pylori infection.
CONCLUSIONS: We found no association between RAP and H pylori
infection in children and conicting evidence for an association be-
tween epigastric pain and H pylori infection. We found evidence for an
association between UAP but could not conrm this nding in children
seen in primary care. Pediatrics 2010;125:e651e669
AUTHORS: Leo A. A. Spee, MD, Marieke B. Madderom,
MSc, Maaike Pijpers, MD, Yvonne van Leeuwen, PhD, and
Marjolein Y. Berger, MD, PhD
Department of General Practice, Erasmus Medical
CenterUniversity Medical Center, Rotterdam, Netherlands
KEY WORDS
Helicobacter pylori, signs and symptoms, digestive, meta-
analysis, review
ABBREVIATIONS
GIgastrointestinal
RAPrecurrent abdominal pain
ORodds ratio
CIcondence interval
UAPunspecied abdominal pain
SRAPshort-term recurrent abdominal pain
GPgeneral practitioner
www.pediatrics.org/cgi/doi/10.1542/peds.2010-0941
doi:10.1542/peds.2010-0941
Accepted for publication Oct 21, 2009
Address correspondence to Marjolein Y. Berger, MD, PhD,
Erasmus MC, Department of General Practice, PO Box 2040, 3000
CA Rotterdam, Netherlands. E-mail: m.berger@erasmusmc.nl
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright 2010 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have
no nancial relationships relevant to this article to disclose.
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e651
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
Helicobacter pylori is 1 of the most
common bacterial pathogens in hu-
mans and affects 50% of the worlds
population.
1
The prevalence of H pylori
infection varies greatly between devel-
oping countries and developed coun-
tries (respectively, 90% vs 40% at the
age of 40),
1
and infection is mainly ac-
quired in early childhood.
2
In adults,
H pylori infection is associated with
conditions such as chronic active gas-
tritis and peptic ulcer disease,
1
and
H pylori has been conrmed as the
most important risk factor for non-
cardia gastric adenocarcinomas and
gastric mucosa-associated lymphoid
tissue lymphomas.
3
Despite this knowl-
edge, the natural history of H pylori
infection in children, such as the mode
of acquisition and signs of infection, is
poorly understood.
Guidelines on screening for H pylori
in children contradict. Recommenda-
tions vary from no need to screen chil-
dren with gastrointestinal (GI) symp-
toms
4
and no need to screen children
with recurrent abdominal pain (RAP)
5
to all children with upper GI symptoms
should be tested for H pylori infection
(Maastricht III).
6
These recommenda-
tions are based on the lack of proof
that infection with H pylori is a signi-
cant cause of GI symptoms.
In addition, nowadays, a lot of diagnos-
tic tests for H pylori are available.
Some of them, such as the 13C-urea
breath test, detection of H pylori anti-
gen in stool, and detection of specic
antibodies in serum,
7
are suitable for
use in primary care. Thus, this in-
creased availability is likely to result in
increased number of children to be
tested. This emphasizes the need for
up-to-date guidelines with indications
for investigating and treating children
for H pylori infection.
Good-quality studies, preferably sum-
marized in a systematic review, form
the basis for evidence-based screen-
ing guidelines. Previous reviews
8,9
re-
garding this topic were limited to the
association between H pylori and spe-
cic symptoms, such as RAP. Because
of the limitations of previous system-
atic reviews and the several studies
published after the publication of these
analyses, we performed a new system-
atic literature review to review sys-
tematically the extent and the quality
of the current published evidence for a
relationship between GI symptoms and
H pylori infection in children.
METHODS
To identify relevant publications, we
performed a Medline database search
from1966 to July 27, 2009, by using the
following key words: Helicobacter py-
lori, Campylobacter pylori, abdo-
minal pain, and dyspepsia. A search
strategy for follow-up studies recom-
mended by Altman
10
was added. The
Embase database was searched from
1980 to July 27, 2009; the search strat-
egy for Medline was adapted for Em-
base with the assistance of a librarian
(Appendix 1). To identify additional
potentially relevant publications, we
hand searched the reference lists of
included studies, of published review
articles, and of articles written by ex-
perts in the eld. No language restric-
tion was used.
Study Selection
We limited our search to studies that
compared children who did have
symptoms with children who did not
have symptoms. All abstracts of
identied articles were screened for
eligibility, and decisions regarding in-
clusion of studies were made indepen-
dently by 2 reviewers (L.A.A.S. and
M.B.M. or Y.vL.). We used 4 criteria to
select relevant studies: (1) the study
had a case-control, cross-sectional, or
prospective cohort design; (2) 1 of its
aims was to evaluate the association
between Hpylori infection and GI symp-
toms; (3) the study group included chil-
dren aged 0 to 18 years; and (4) at least
30 children were included and sepa-
rately analyzed. Because of an in-
creased risk for acquiring an H pylori
infection, studies concerning exclu-
sively children with relevant comorbid-
ity such as mental disabilities, immu-
nodecient disorders, and diabetes
were excluded.
Interobserver reliability of the eligibil-
ity screening was calculated with Co-
hens .
11
Any disagreements between
both reviewers were resolved through
consensus or by arbitration of a third
person (M.B.M. or Y.vL.). Full-text arti-
cles of all selected titles were re-
trieved or in case the abstract gave in-
sufcient information on the inclusion
criteria. When an included study or the
data of a study were not available, rst
authors were contacted.
Quality Assessment
To rate the risk for bias of the included
studies, we scored 9 identical method-
ologic criteria with 1 additional crite-
rion for case-control/cross-sectional
studies and 2 additional criteria for
prospective cohort studies (Appendix
2). The criteria were adapted from Alt-
man,
10
Lievense et al,
12
Hayden et al,
13
and the STROBE Statement
14
and were
modied to cover the topic of this re-
view. Criteria could be answered with
yes (), no (). or dont know
(?). One point was given to a criterion
answered with yes, and no points
were given when answered with no
or dont know. Equal weights were
applied to all items, resulting in a max-
imum score of 10 points for case-
control/cross-sectional studies and 11
points for prospective cohort studies.
Low risk for bias was dened as a
score of 7 points. Two reviewers
scored all included articles indepen-
dently (L.A.A.S. and M.B.M.). Interob-
server variability was calculated with
Cohens . In case of disagreement be-
tween both reviewers, a third reviewer
(Y.vL.) made the nal decision.
e652 SPEE et al
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
Data Extraction and Analysis
Two reviewers performed data extrac-
tion on a structured list independently.
Extracted data included demograph-
ics, description of the study popula-
tion, inclusion and exclusion criteria,
baseline characteristics, type of symp-
toms analyzed, diagnostic tests used,
and outcome data. As a measure for
the association between GI symptoms
and H pylori, odds ratios (ORs) with
95% condence intervals (CIs) were
calculated for each symptom on the
basis of unadjusted data presented in
individual studies.
Data analysis was performed by using
Review Manager 5.0 (RevMan). The
weight given to each study was based
on the inverse of the variance. Hetero-
geneity was quantied by Z
2
and I
2
,
which can be interpreted as the per-
centage of the total variation between
studies that is attributable to hetero-
geneity rather than to chance. A value
of 0% indicates no heterogeneity.
When statistically signicant heteroge-
neity (P .05) was observed, the re-
sults of the random-effects model are
presented. When there was statisti-
cally signicant heterogeneity in out-
comes across studies, subgroup anal-
yses according to the level of risk for
bias and different geographic loca-
tions (ie, low-prevalence areas [West-
ern countries, United States, Canada]
versus high-prevalence areas [Medi-
terranean, African, and Asian coun-
tries]) were performed. In addition,
the effect of outliers on the results was
evaluated.
When in studies the term RAP was
used, we considered it conformApleys
criteria,
15
when there was a reference
to Apley or the denition used by the
authors was almost similar in time
spectrumto the denition proposed by
Apley (ie, at least 3 discrete episodes
of abdominal pain of sufcient severity
to interrupt normal daily activities or
performance over a period of not
less than 3 months). When studies re-
ported on unspecied abdominal
pain, abdominal pain, symptomatic
patients, or GI-referral patients in
relation to H pylori infection and
thus not fullling Apleys criteria, we
grouped these outcomes as unspeci-
ed abdominal pain (UAP).
RESULTS
In total, 1120 potentially relevant ab-
stracts were identied. After removing
duplicates, we were left with 880
unique abstracts. After screening all
abstracts, 39 publications met our in-
clusion criteria and none of the exclu-
sion criteria.
1654
By searching the ref-
erence lists of previous reviewarticles
and included studies, we identied 1
additional study.
55
The interobserver
agreement of the overall eligibility was
0.826.
One study could not be retrieved and
thus could not be included in our anal-
ysis.
49
After reading full-text articles,
we excluded another article because
the study population did not include
children who were aged 0 to 18 years.
50
Finally, 38 articles were reviewed: 23
case-control studies,
1635,53,54
14 cross-
sectional studies,
3647,51,52
and 1 pro-
spective cohort study.
48
Of 23 in-
cluded case-control studies, 19 were
hospital based
16,17,1921,2335,55
, 3 were
population-based,
18,53,54
and 1 was
primary care based.
22
All cross-
sectional studies were population
based,
3642,4447,51,55
except for 1 that in-
cluded children in whom infection was
successfully eradicated previously.
43
The only included prospective cohort
study was population based.
48
Results of the Methodologic
Quality Assessment
The 2 reviewers (L.A.A.S. and M.B.M.)
initially agreed on 89.5% of all quality
items scored. The interobserver
agreement of the assessment of risk
for bias was high ( 0.789).
Mean score of risk for bias of all 38
included studies was 6.03, ranging
from 3.00 to 10.00. The mean quality
score of case-control studies and
cross-sectional studies separately
was 5.35 (range: 3.0010.00) vs 6.93
(range: 5.009.00), respectively. This
difference was mainly caused by the
lack of equal assessment of GI symp-
toms for both case patients and con-
trol subjects in 19 of 23 case-control
studies, whereas all 14 cross-sectional
studies used equal symptom assess-
ment. Furthermore, 12 case-control
studies did not draw case patients and
control subjects from a population at
the same risk for exposure, whereas
the studied populations of all cross-
sectional studies did. The only prospec-
tive cohort study scored 9 of 11 points.
In total 8 case-control stud-
ies,
1719,22,28,29,30,53
7 cross-sectional
studies,
36,37,39,41,45,46,52
and the prospec-
tive cohort study
48
were categorized as
having lowrisk for bias. The most prev-
alent shortcomings of case-control
and cross-sectional studies were a
lack of blinded assessment of GI symp-
toms and H pylori infection (n 31),
no use of multivariate analysis (n
27), and that prognostic factors were
not comparable at baseline and no
correction for these factors was ap-
plied in the analysis (n 29).
Prevalence of H pylori
The prevalence of H pylori in population-
based cross-sectional studies ranged
from 9.4% to 56.6% with a mean prev-
alence of 28.0% (SD: 16.2%). The prev-
alence in high-prevalence areas (n
8) ranged from 15.8%
47
to 56.6%
36
with
a mean prevalence of 37.0%. The prev-
alence in low-prevalence areas (n 6)
ranged from 9.4%
41
to 28.9%,
42
with a
mean prevalence of 16.1%. The effect
of different tests on the prevalence of
H pylori could not be evaluated be-
cause a large diversity of (combina-
tions of) diagnostic tests for H pylori
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e653
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
with different cutoff points were used,
although the vast majority of studies
included serology testing.
RAP and H pylori
Fourteen case-control studies, involv-
ing 3253 participants, reported on the
relationship between RAP and H pylori
infection in children.* Six had low risk
for bias
17,18,22,26,30,53
and 8 had high risk
for bias.
23,25,3134,54,55
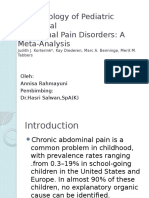
Figure 1 presents
the meta-analysis of the OR of an H py-
lori infection given the presence of
RAP. Because of statistically signicant
heterogeneity (P .00001), the
random-effects model is presented.
The pooled OR for all case-control stud-
ies was 1.69 (95% CI: 0.992.86).
When we excluded the 2 outlier stud-
ies of Mendez Nieto et al
32
and
Mukherjee et al.
34
the pooled OR be-
came 1.21 (95% CI: 0.821.78), but
statistical heterogeneity remained
signicant. In all additional analyses, the
aforementioned outliers remained ex-
cluded. Evaluation of heterogeneity ex-
plained some of it but did not alter the
estimated effect size.
Ten cross-sectional studies, involving
3980 participants, reported on the re-
lation between RAP and H pylori. Four
had low risk for bias
36,37,39,45
and 6 high
risk.
38,4244,47,51
However, the study of
Ertem et al,
44
reporting an OR of 1.33,
could not be pooled due to missing the
pooled OR for the remaining studies
was 1.69 (95% CI: 0.833.44; random
effects-model; P .00001; Fig 2). The
studies of Leandro Liberato et al
47
and
Telmesani
51
explained statistical heter-
ogeneity; excluding these outliers re-
sulted in a pooled OR of 1.00 (95% CI:
0.761.31; xed model; P .60). In ad-
ditional analyses, these outliers re-
mained excluded.
The pooled OR for the 4 studies with
low risk for bias was 0.95 (95% CI:
0.661.37; xed model; P .24). The
relationship between RAP and H pylori
infection was not inuenced by risk for
bias, setting, or geographic location.
Two case-control studies
22,30
and 2
cross-sectional studies
37,46
concerning
RAP reported ORs adjusted for con-
founders (Tables 1 and 2) ; however, all
adjusted ORs are comparable to the
pooled unadjusted ORs presented and
remained nonsignicant.
UAP and H pylori
Six hospital-based case-control stud-
ies
16,19,21,24,28,35
that included 3142 partici-
pants reported on the association be-
tween UAP and H pylori infection. Two
studies with low risk for bias
19,28
and 4
with high risk
16,21,24,35
had a pooled OR of
2.87 (95% CI: 1.625.09; random-effects
model; P .0001; Fig 3). In the studies
with lowrisk for bias only, the pooled OR
was 1.66 (95% CI: 1.212.28; xed model;
P .23). Pooling the 4 studies with high
riskfor bias resultedinapooledORof 4.69
(95%CI: 3.356.57; xed model; P .36).
Five population-based cross-sectional
studies
36,37,39,41,52
that included 3251
participants and reported on UAP in
children who were seen in primary
care all had low risk for bias. The
pooled OR was 0.99 (95% CI: 0.462.11;
random-effects model; P .00001; Fig 4).
Three studies, 1 hospital-based case-
control study
16
and 2 population-based
cross-sectional studies,
37,52
adjusted
for confounders (Tables 1 and 2). The
adjusted ORs were comparable to the
pooled ORs presented.
Epigastric Pain and H pylori
Epigastric pain was evaluated in 2
case-control studies
18,20
and 1 cross-
sectional study.
43
Because of the diver-
sity of outcome denitions, we were
not able to pool data. The population-
based case-control study of Yang et
al
18
had low risk for bias and included *Refs 17, 18, 22, 23, 25, 26, 3034, and 5355.
FIGURE 1
Meta-analysis of case-control studies concerning RAP related to H pylori infection. Events indicates number children with H pylori infection.
e654 SPEE et al
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
253 participants. They reported on
short-term recurrent abdominal pain
(SRAP): abdominal pain that met Ap-
leys criteria
15
but with a shorter dura-
tion in a range from 2 weeks to 3
months. The prevalence of H pylori
infection was higher in children with
SRAP than in healthy control subjects
(OR: 3.4 [95%CI: 1.67.2]). They further
assessed whether specic clinical
presentations were associated with
H pylori infection in the children with
SRAP or RAP. Children who presented
with abdominal pain in the epigastric
area had a signicantly higher preva-
lence of H pylori infection when they
had SRAP but not when they had RAP;
the OR could not be calculated with the
available data.
The hospital-based case-control study
of Ng et al
20
had high risk for bias.
The study, which included 1088 par-
ticipants, reported an OR of 2.03
(95% CI: 1.353.06) given the pres-
ence of epigastric pain. The OR of
the 1 hospital-based cross-sectional
study with high risk for bias
43
was 3.2
(95% CI: 0.7713.35).
Diarrhea and H pylori
Two case-control studies
18,27
and 3
population-based cross-sectional stud-
ies
36,39,40
reported outcomes on the
association between diarrhea and
H pylori infection in children. One case-
control study
18
and 2 cross-sectional
studies
36,39
had low risk for bias. All
studies that reported on diarrhea, ex-
cept for the 1 by Bode et al,
39
were per-
formed in high-prevalence areas. The
pooled OR in case-control studies that
included 365 participants, 1 of which
was population based
18
and 1 of which
was hospital based,
27
was 0.95 (95%CI:
0.471.90; xed model; P .32). In the
cross-sectional studies that included
999 participants, the pooled OR was
0.70 (95%CI: 0.133.96; random-effects
model; P .01).
Vomiting and H pylori
Three population-based cross-sectional
studies, all of which were at low risk
for bias, included 2054 participants
and investigated the association be-
tween vomiting and H pylori infec-
tion
36,39,52
; the pooled OR was 1.05 (95%
CI: 0.402.75; random-effects model;
P .0002). Two studies
36,52
were per-
formed in high-prevalence areas, and
1 study
39
was performed in low-
prevalence areas.
Other Symptoms and H pylori
Several studies reported on various
other GI symptoms, such as perium-
bilical pain,
18
atus,
18
constipation,
18,37
nausea,
43
loose stools,
37
postprandial
fullness,
18,43
halitosis,
43
dyspepsia,
29,36
and regurgitation,
37
but none of these
symptoms was associated with H py-
lori infection.
The only prospective cohort study with
a follow-up period from 6 months to 11
years
48
included 305 participants and
had low risk for bias. The authors con-
cluded that UAP during childhood was
reported more often in children with
H pylori seropositivity at some point
during the study than for seronegative
children (adjusted OR: 2.2 [95%CI: 1.0
4.4). Children who were seropositive at
some point during the study more of-
ten reported RAP at 11 years of age
than did seronegative children, but the
difference was not statistically signi-
cant (OR adjusted for gender: 2.0 [95%
CI: 0.84.6) (Table 3). Spontaneous
clearance of H pylori infection was re-
ported in 80% of previously infected
children at the end of the study.
DISCUSSION
We found evidence for an association
between UAP (ie, patients with abdom-
inal pain, symptoms, or GI referral)
and H pylori infection in referred chil-
dren (pooled OR: 2.87 [95% CI: 1.62
5.09) but could not conrm this nding
in children who were seen in primary
care (pooled OR: 0.99 [95% CI: 0.46
2.11). Two studies
16,37
adjusted for
known risk factors for H pylori, but this
did not change this results. In addition,
we found conicting evidence for an
FIGURE 2
Meta-analysis of cross-sectional studies concerning RAP related to H pylori infection. Events indicates number children with H pylori infection.
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e655
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
T
A
B
L
E
1
S
t
u
d
y
C
h
a
r
a
c
t
e
r
i
s
t
i
c
s
o
f
I
n
c
l
u
d
e
d
C
a
s
e
-
C
o
n
t
r
o
l
S
t
u
d
i
e
s
S
o
u
r
c
e
S
e
t
t
i
n
g
,
P
l
a
c
e
,
C
o
u
n
t
r
y
,
P
e
r
i
o
d
C
a
s
e
P
a
t
i
e
n
t
s
C
o
n
t
r
o
l
S
u
b
j
e
c
t
s
D
i
a
g
n
o
s
t
i
c
T
e
s
t
U
s
e
d
f
o
r
D
e
t
e
r
m
i
n
a
t
i
o
n
o
f
H
p
y
l
o
r
i
I
n
f
e
c
t
i
o
n
(
C
u
t
o
f
f
P
o
i
n
t
)
O
R
(
9
5
%
C
I
)
Q
u
a
l
i
t
y
S
c
o
r
e
D
a
u
g
u
l
e
e
t
a
l
,
1
6
2
0
0
7
D
i
a
g
n
o
s
t
i
c
C
e
n
t
r
e
o
f
R
i
g
a
,
L
a
t
v
i
a
,
1
9
9
8
2
0
0
0
4
0
c
o
n
s
e
c
u
t
i
v
e
c
h
i
l
d
r
e
n
w
i
t
h
i
n
d
i
c
a
t
i
o
n
f
o
r
u
p
p
e
r
G
I
e
n
d
o
s
c
o
p
y
,
a
g
e
r
a
n
g
e
8
1
2
y
,
3
9
%
m
a
l
e
5
5
a
s
y
m
p
t
o
m
a
t
i
c
c
h
i
l
d
r
e
n
w
h
o
v
i
s
i
t
e
d
t
h
e
i
r
d
o
c
t
o
r
f
o
r
g
e
n
e
r
a
l
c
h
e
c
k
u
p
o
r
m
i
n
o
r
h
e
a
l
t
h
p
r
o
b
l
e
m
s
,
a
g
e
d
7
1
2
,
5
5
%
m
a
l
e
C
a
s
e
s
:
R
U
T
a
n
d
/
o
r
c
u
l
t
u
r
e
p
o
s
i
t
i
v
e
C
o
n
t
r
o
l
s
:
1
3
C
-
U
B
T
U
A
P
:
1
.
8
0
(
0
.
6
2
5
.
1
4
)
(
a
d
j
u
s
t
e
d
f
o
r
a
g
e
)
4
M
a
l
a
t
y
e
t
a
l
,
1
7
2
0
0
6
P
e
d
i
a
t
r
i
c
G
a
s
t
r
o
e
n
t
e
r
o
l
o
g
y
C
l
i
n
i
c
T
e
x
a
s
C
h
i
l
d
r
e
n
s
H
o
s
p
i
t
a
l
a
n
d
6
p
r
i
m
a
r
y
c
a
r
e
p
e
d
i
a
t
r
i
c
c
l
i
n
i
c
s
,
H
o
u
s
t
o
n
,
T
X
,
J
u
n
2
0
0
1
D
e
c
2
0
0
2
2
4
3
c
o
n
s
e
c
u
t
i
v
e
c
h
i
l
d
r
e
n
r
e
f
e
r
r
e
d
w
i
t
h
a
b
d
o
m
i
n
a
l
p
a
i
n
,
a
g
e
r
a
n
g
e
3
1
8
y
,
4
0
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
c
h
i
l
d
r
e
n
w
i
t
h
c
h
r
o
n
i
c
i
l
l
n
e
s
s
/
o
t
h
e
r
m
e
d
i
c
a
l
c
o
n
d
i
t
i
o
n
s
3
3
0
a
s
y
m
p
t
o
m
a
t
i
c
c
h
i
l
d
r
e
n
a
t
t
e
n
d
i
n
g
1
3
l
i
c
e
n
s
e
d
c
h
i
l
d
c
a
r
e
c
e
n
t
e
r
s
i
n
H
o
u
s
t
o
n
,
T
X
,
a
g
e
d
3
1
8
y
,
4
5
%
m
a
l
e
C
a
s
e
s
:
1
3
C
-
U
B
T
C
o
n
t
r
o
l
s
:
1
3
C
-
U
B
T
(
i
n
c
r
e
a
s
e
o
f
1
3
C
a
b
u
n
d
a
n
c
e
o
f
1
0
g
o
f
u
r
e
a
h
y
d
r
o
l
y
z
e
d
p
e
r
m
i
n
)
R
A
P
:
0
.
6
1
(
9
.
3
7
1
.
0
0
)
7
Y
a
n
g
e
t
a
l
,
1
8
2
0
0
5
E
l
e
m
e
n
t
a
r
y
s
c
h
o
o
l
a
n
d
a
s
s
o
c
i
a
t
e
d
p
r
e
s
c
h
o
o
l
k
i
n
d
e
r
g
a
r
t
e
n
,
T
a
i
n
a
n
,
T
a
i
w
a
n
1
7
8
c
h
i
l
d
r
e
n
w
h
o
f
u
l
l
l
e
d
t
h
e
c
r
i
t
e
r
i
a
o
f
R
A
P
o
r
S
R
A
P
(
R
A
P
d
u
r
i
n
g
2
w
k
3
m
o
)
;
a
g
e
r
a
n
g
e
4
1
2
y
,
m
e
a
n
:
9
.
2
y
,
5
2
%
m
a
l
e
2
1
2
a
g
e
-
a
n
d
g
e
n
d
e
r
-
m
a
t
c
h
e
d
,
a
s
y
m
p
t
o
m
a
t
i
c
c
h
i
l
d
r
e
n
f
r
o
m
t
h
e
s
a
m
e
s
c
h
o
o
l
C
a
s
e
s
:
E
L
I
S
A
C
o
n
t
r
o
l
s
:
E
L
I
S
A
(
a
b
s
o
r
b
a
n
c
e
i
n
d
e
x
o
f
0
.
1
4
)
R
A
P
:
0
.
5
4
(
0
.
2
1
1
.
4
0
)
S
R
A
P
:
3
.
3
9
(
1
.
6
0
7
.
1
7
)
7
C
h
o
n
g
e
t
a
l
,
1
9
2
0
0
3
1
2
c
h
i
l
d
r
e
n
s
h
o
s
p
i
t
a
l
s
o
r
m
e
d
i
c
a
l
c
e
n
t
e
r
s
t
h
r
o
u
g
h
o
u
t
t
h
e
U
n
i
t
e
d
S
t
a
t
e
s
,
J
u
n
1
9
9
6
D
e
c
1
9
9
7
3
7
3
s
y
m
p
t
o
m
a
t
i
c
G
I
r
e
f
e
r
r
a
l
c
h
i
l
d
r
e
n
e
v
a
l
u
a
t
e
d
i
n
a
G
I
c
l
i
n
i
c
f
o
r
a
b
d
o
m
i
n
a
l
p
a
i
n
a
n
d
v
o
m
i
t
i
n
g
,
a
g
e
r
a
n
g
e
:
1
1
8
y
,
m
e
a
n
:
1
0
.
1
y
,
4
8
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
c
h
i
l
d
r
e
n
w
i
t
h
i
n
t
a
k
e
o
f
a
n
t
i
b
i
o
t
i
c
s
,
h
i
s
t
a
m
i
n
e
-
2
b
l
o
c
k
e
r
s
,
o
r
p
r
o
t
o
n
p
u
m
p
i
n
h
i
b
i
t
o
r
s
1
m
o
b
e
f
o
r
e
e
n
t
e
r
i
n
g
t
h
e
s
t
u
d
y
6
1
8
c
h
i
l
d
r
e
n
s
e
e
n
i
n
a
c
l
i
n
i
c
a
l
s
e
t
t
i
n
g
,
w
h
o
r
e
q
u
i
r
e
d
b
l
o
o
d
d
r
a
w
i
n
g
a
s
p
a
r
t
o
f
s
t
a
n
d
a
r
d
c
l
i
n
i
c
a
l
m
a
n
a
g
e
m
e
n
t
,
w
i
t
h
o
u
t
G
I
c
o
m
p
l
a
i
n
t
s
a
g
e
r
a
n
g
e
:
2
m
o
1
8
y
,
m
e
a
n
a
g
e
:
7
.
7
y
,
5
6
%
m
a
l
e
C
a
s
e
s
:
E
I
A
C
o
n
t
r
o
l
s
:
E
I
A
R
e
f
e
r
r
e
d
(
s
y
m
p
t
o
m
a
t
i
c
)
:
1
.
7
7
(
1
.
2
7
2
.
4
7
)
8
N
g
e
t
a
l
,
2
0
2
0
0
3
N
a
t
i
o
n
a
l
U
n
i
v
e
r
s
i
t
y
H
o
s
p
i
t
a
l
,
S
i
n
g
a
p
o
r
e
,
R
e
p
u
b
l
i
c
o
f
S
i
n
g
a
p
o
r
e
4
8
9
c
o
n
s
e
c
u
t
i
v
e
p
a
t
i
e
n
t
s
w
i
t
h
e
p
i
g
a
s
t
r
i
c
p
a
i
n
;
o
u
t
p
a
t
i
e
n
t
r
e
f
e
r
r
a
l
s
t
o
p
e
d
i
a
t
r
i
c
G
I
c
l
i
n
i
c
,
m
e
a
n
a
g
e
:
8
.
5
3
.
3
y
,
4
6
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
c
h
i
l
d
r
e
n
w
h
o
u
s
e
d
a
n
t
i
b
i
o
t
i
c
s
w
i
t
h
i
n
4
w
k
o
f
t
h
e
s
t
u
d
y
5
9
9
s
c
h
o
o
l
c
h
i
l
d
r
e
n
p
a
r
t
i
c
i
p
a
t
i
n
g
i
n
a
s
e
r
o
e
p
i
d
e
m
i
o
l
o
g
i
c
s
u
r
v
e
y
o
f
D
e
n
g
u
e
i
n
t
h
e
e
a
s
t
e
r
n
p
a
r
t
o
f
S
i
n
g
a
p
o
r
e
,
m
e
a
n
a
g
e
:
9
.
0
0
.
5
y
C
a
s
e
s
:
E
L
I
S
A
C
o
n
t
r
o
l
s
:
E
L
I
S
A
(
2
S
D
a
b
o
v
e
v
a
l
u
e
f
o
r
h
i
s
t
o
l
o
g
y
-
c
o
n
r
m
e
d
n
e
g
a
t
i
v
e
s
e
r
a
)
E
p
i
g
a
s
t
r
i
c
p
a
i
n
(
s
p
i
r
a
l
)
:
2
.
0
3
(
1
.
3
5
3
.
0
6
)
5
P
l
e
b
a
n
i
e
t
a
l
,
2
1
1
9
9
9
P
e
d
i
a
t
r
i
c
D
e
p
a
r
t
m
e
n
t
,
P
a
d
u
a
U
n
i
v
e
r
s
i
t
y
H
o
s
p
i
t
a
l
,
I
t
a
l
y
1
8
3
c
o
n
s
e
c
u
t
i
v
e
s
y
m
p
t
o
m
a
t
i
c
c
h
i
l
d
r
e
n
w
h
o
u
n
d
e
r
w
e
n
t
u
p
p
e
r
G
I
e
n
d
o
s
c
o
p
y
,
a
g
e
r
a
n
g
e
:
1
1
6
y
,
4
3
%
m
a
l
e
9
2
1
r
a
n
d
o
m
l
y
s
e
l
e
c
t
e
d
f
r
o
m
t
h
o
s
e
p
r
e
s
e
n
t
a
t
t
h
e
s
e
c
o
n
d
-
d
e
g
r
e
e
s
c
h
o
o
l
s
o
f
P
a
d
u
a
,
a
g
e
r
a
n
g
e
:
1
1
1
4
y
,
5
3
%
m
a
l
e
C
a
s
e
s
:
a
t
l
e
a
s
t
h
i
s
t
o
l
o
g
y
p
o
s
i
t
i
v
e
C
o
n
t
r
o
l
s
:
a
n
t
i
H
p
-
I
g
G
U
A
P
:
4
.
9
8
(
3
.
0
3
8
.
1
6
)
3
M
a
c
A
r
t
h
u
r
e
t
a
l
,
2
2
1
9
9
9
6
p
r
i
m
a
r
y
c
a
r
e
p
e
d
i
a
t
r
i
c
i
a
n
s
,
T
o
r
o
n
t
o
,
C
a
n
a
d
a
1
0
0
c
h
i
l
d
r
e
n
p
r
e
s
e
n
t
i
n
g
w
i
t
h
R
A
P
,
a
g
e
r
a
n
g
e
:
5
1
5
y
,
m
e
a
n
:
9
.
0
2
.
7
y
,
3
7
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
c
h
i
l
d
r
e
n
w
i
t
h
c
o
n
c
u
r
r
e
n
t
d
i
s
e
a
s
e
,
s
u
s
p
e
c
t
e
d
o
r
g
a
n
i
c
d
i
s
e
a
s
e
,
a
g
e
d
5
y
,
o
r
h
a
d
u
s
e
d
b
i
s
m
u
t
h
i
n
t
h
e
p
r
e
v
i
o
u
s
m
o
n
t
h
1
0
0
h
e
a
l
t
h
y
c
h
i
l
d
r
e
n
u
n
d
e
r
g
o
i
n
g
a
r
o
u
t
i
n
e
c
h
e
c
k
u
p
o
r
v
a
c
c
i
n
a
t
i
o
n
,
m
e
a
n
a
g
e
:
1
0
.
0
3
.
2
y
,
5
7
%
m
a
l
e
C
a
s
e
s
:
s
e
r
o
l
o
g
y
a
n
d
/
o
r
1
3
C
-
U
B
T
C
o
n
t
r
o
l
s
:
s
e
r
o
l
o
g
y
a
n
d
/
o
r
1
3
C
-
U
B
T
R
A
P
:
0
.
6
5
(
0
.
0
8
2
.
5
6
)
(
a
d
j
u
s
t
m
e
n
t
n
o
t
m
e
n
t
i
o
n
e
d
)
1
0
G
u
n
e
l
e
t
a
l
,
2
3
1
9
9
8
D
e
p
a
r
t
m
e
n
t
s
o
f
P
e
d
i
a
t
r
i
c
S
u
r
g
e
r
y
a
n
d
P
e
d
i
a
t
r
i
c
s
,
K
o
n
y
a
,
T
u
r
k
e
y
,
d
u
r
i
n
g
1
2
-
m
o
p
e
r
i
o
d
4
2
c
h
i
l
d
r
e
n
w
i
t
h
R
A
P
,
a
g
e
r
a
n
g
e
9
1
5
y
,
m
e
a
n
:
9
.
4
3
.
2
y
;
e
x
c
l
u
d
e
d
:
i
f
o
r
g
a
n
i
c
c
a
u
s
e
f
o
r
R
A
P
(
e
g
,
p
e
p
t
i
c
d
i
s
e
a
s
e
,
I
B
D
,
e
n
z
y
m
e
d
e
c
i
e
n
c
i
e
s
)
w
a
s
f
o
u
n
d
5
0
h
e
a
l
t
h
y
c
h
i
l
d
r
e
n
a
t
t
e
n
d
i
n
g
r
o
u
t
i
n
e
d
a
y
s
u
r
g
e
r
y
,
m
e
a
n
a
g
e
:
9
.
6
5
3
.
1
5
y
C
a
s
e
s
:
I
g
G
a
n
t
i
b
o
d
y
t
e
s
t
C
o
n
t
r
o
l
s
:
I
g
G
a
n
t
i
b
o
d
y
t
e
s
t
R
A
P
:
1
.
4
1
(
0
.
5
8
3
.
4
0
)
3
B
l
u
m
e
l
e
t
a
l
,
2
4
1
9
9
8
K
i
n
d
e
r
s
p
i
t
a
l
d
e
r
S
t
a
d
t
W
i
e
n
,
A
u
s
t
r
i
a
3
1
c
h
i
l
d
r
e
n
p
r
e
s
e
n
t
i
n
g
w
i
t
h
c
h
r
o
n
i
c
a
b
d
o
m
i
n
a
l
p
a
i
n
4
w
k
w
i
t
h
n
e
g
a
t
i
v
e
s
t
o
o
l
c
u
l
t
u
r
e
,
n
o
r
m
a
l
b
l
o
o
d
c
o
u
n
t
s
,
a
n
d
n
o
r
m
a
l
a
b
d
o
m
i
n
a
l
e
c
h
o
,
a
g
e
r
a
n
g
e
:
6
1
4
y
,
m
e
a
n
:
1
0
.
5
1
y
,
5
2
%
m
a
l
e
3
1
a
g
e
-
a
n
d
n
a
t
i
o
n
a
l
i
t
y
-
m
a
t
c
h
e
d
a
s
y
m
p
t
o
m
a
t
i
c
c
h
i
l
d
r
e
n
w
h
o
w
e
r
e
u
n
d
e
r
g
o
i
n
g
e
l
e
c
t
i
v
e
/
a
c
u
t
e
s
u
r
g
e
r
y
o
r
o
u
t
p
a
t
i
e
n
t
c
h
i
l
d
r
e
n
w
h
o
r
e
c
e
i
v
e
d
t
r
e
a
t
m
e
n
t
f
o
r
n
o
n
i
n
f
e
c
t
i
o
u
s
d
i
s
e
a
s
e
s
,
m
e
a
n
a
g
e
:
1
0
.
5
y
C
a
s
e
s
:
H
p
I
g
G
-
A
K
(
3
S
D
a
b
o
v
e
t
h
e
m
e
a
n
o
f
a
l
l
n
e
g
a
t
i
v
e
t
e
s
t
s
)
C
o
n
t
r
o
l
s
:
H
p
I
g
G
-
A
K
U
A
P
:
2
.
5
2
(
0
.
9
0
7
.
0
2
)
5
e656 SPEE et al
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
T
A
B
L
E
1
C
o
n
t
i
n
u
e
d
S
o
u
r
c
e
S
e
t
t
i
n
g
,
P
l
a
c
e
,
C
o
u
n
t
r
y
,
P
e
r
i
o
d
C
a
s
e
P
a
t
i
e
n
t
s
C
o
n
t
r
o
l
S
u
b
j
e
c
t
s
D
i
a
g
n
o
s
t
i
c
T
e
s
t
U
s
e
d
f
o
r
D
e
t
e
r
m
i
n
a
t
i
o
n
o
f
H
p
y
l
o
r
i
I
n
f
e
c
t
i
o
n
(
C
u
t
o
f
f
P
o
i
n
t
)
O
R
(
9
5
%
C
I
)
Q
u
a
l
i
t
y
S
c
o
r
e
B
a
n
s
a
l
e
t
a
l
,
2
5
1
9
9
8
K
a
l
a
w
a
t
i
C
h
i
l
d
r
e
n
H
o
s
p
i
t
a
l
,
D
i
v
i
s
i
o
n
o
f
P
e
d
i
a
t
r
i
c
G
a
s
t
r
o
e
n
t
e
r
o
l
o
g
y
a
n
d
N
u
t
r
i
t
i
o
n
,
N
e
w
D
e
l
h
i
,
I
n
d
i
a
7
2
c
h
i
l
d
r
e
n
r
e
f
e
r
r
e
d
w
i
t
h
c
o
m
p
l
a
i
n
t
s
o
f
R
A
P
;
n
o
o
r
g
a
n
i
c
c
a
u
s
e
w
a
s
f
o
u
n
d
a
f
t
e
r
s
t
o
o
l
a
n
d
u
r
i
n
e
e
x
a
m
i
n
a
t
i
o
n
s
a
n
d
a
p
s
y
c
h
o
l
o
g
i
c
a
l
e
v
a
l
u
a
t
i
o
n
;
a
g
e
r
a
n
g
e
:
3
1
2
y
,
5
5
%
m
a
l
e
2
6
a
g
e
-
a
n
d
g
e
n
d
e
r
-
m
a
t
c
h
e
d
c
h
i
l
d
r
e
n
w
i
t
h
c
o
m
p
l
a
i
n
t
s
o
t
h
e
r
t
h
a
n
t
h
o
s
e
r
e
l
a
t
e
d
t
o
t
h
e
G
I
t
r
a
c
t
,
a
g
e
r
a
n
g
e
:
3
1
4
y
C
a
s
e
s
:
R
U
T
a
n
d
/
o
r
h
i
s
t
o
l
o
g
y
p
o
s
i
t
i
v
e
C
o
n
t
r
o
l
s
:
s
e
r
o
l
o
g
y
(
H
p
-
I
g
G
2
0
U
/
m
L
)
R
A
P
:
1
.
2
3
(
0
.
3
4
4
.
4
4
)
3
W
e
w
e
r
e
t
a
l
,
2
6
1
9
9
8
H
v
i
d
o
v
r
e
H
o
s
p
i
t
a
l
,
U
n
i
v
e
r
s
i
t
y
o
f
C
o
p
e
n
h
a
g
e
n
,
D
e
n
m
a
r
k
4
5
0
c
h
i
l
d
r
e
n
w
i
t
h
R
A
P
w
i
t
h
n
o
o
t
h
e
r
o
b
v
i
o
u
s
c
a
u
s
e
s
o
f
R
A
P
,
a
g
e
r
a
n
g
e
3
.
1
1
7
.
0
y
,
m
e
a
n
:
9
.
0
y
,
4
0
%
m
a
l
e
9
3
c
h
i
l
d
r
e
n
a
d
m
i
t
t
e
d
f
o
r
m
i
n
o
r
e
l
e
c
t
i
v
e
s
u
r
g
e
r
y
,
o
t
h
e
r
w
i
s
e
i
n
g
o
o
d
h
e
a
l
t
h
a
n
d
d
i
d
n
o
t
s
u
f
f
e
r
f
r
o
m
G
I
c
o
m
p
l
a
i
n
t
s
,
a
g
e
r
a
n
g
e
:
3
1
5
y
,
m
e
a
n
a
g
e
:
6
.
3
y
,
8
2
%
m
a
l
e
C
a
s
e
s
:
E
L
I
S
A
(
2
0
0
E
U
)
a
n
d
W
e
s
t
e
r
n
b
l
o
t
p
o
s
i
t
i
v
e
C
o
n
t
r
o
l
s
:
E
L
I
S
A
a
n
d
W
e
s
t
e
r
n
b
l
o
t
p
o
s
i
t
i
v
e
R
A
P
(
W
e
s
t
e
r
n
b
l
o
t
)
:
2
.
3
6
(
1
.
1
4
4
.
8
7
)
R
A
P
(
E
L
I
S
A
)
:
2
.
0
9
(
1
.
1
6
3
.
7
8
)
7
K
e
h
r
t
e
t
a
l
,
2
7
1
9
9
7
H
e
a
l
t
h
C
e
n
t
e
r
,
T
i
p
i
t
a
p
a
,
N
i
c
a
r
a
g
u
a
,
S
e
p
1
9
9
3
D
e
c
1
9
9
3
5
9
c
h
i
l
d
r
e
n
w
i
t
h
p
e
r
s
i
s
t
e
n
t
d
i
a
r
r
h
e
a
r
e
c
r
u
i
t
e
d
f
r
o
m
t
h
e
U
R
O
o
f
t
h
e
h
e
a
l
t
h
c
e
n
t
e
r
w
i
t
h
n
o
h
i
s
t
o
r
y
o
f
a
n
t
i
b
i
o
t
i
c
u
s
e
i
n
t
h
e
p
r
e
v
i
o
u
s
m
o
n
t
h
,
a
g
e
r
a
n
g
e
:
2
5
6
m
o
,
5
3
%
m
a
l
e
6
4
r
a
n
d
o
m
l
y
s
e
l
e
c
t
e
d
a
g
e
-
m
a
t
c
h
e
d
a
s
y
m
p
t
o
m
a
t
i
c
c
h
i
l
d
r
e
n
r
e
f
e
r
r
e
d
f
r
o
m
p
e
d
i
a
t
r
i
c
i
a
n
s
o
f
t
h
e
c
e
n
t
e
r
,
a
g
e
r
a
n
g
e
:
1
6
5
m
o
,
4
1
%
m
a
l
e
C
a
s
e
s
:
1
3
C
-
U
B
T
(
1
3
C
/
1
2
C
r
a
t
i
o
a
t
6
0
m
i
n
o
v
e
r
b
a
s
e
l
i
n
e
)
C
o
n
t
r
o
l
s
:
1
3
C
-
U
B
T
P
e
r
s
i
s
t
e
n
t
d
i
a
r
r
h
e
a
:
0
.
7
5
(
0
.
3
2
1
.
7
4
)
6
O
z
t
u
r
k
e
t
a
l
,
2
8
1
9
9
6
D
a
y
S
u
r
g
e
r
y
C
l
i
n
i
c
,
H
a
c
e
t
t
e
p
e
U
n
i
v
e
r
s
i
t
y
C
h
i
l
d
r
e
n
s
H
o
s
p
i
t
a
l
,
A
n
k
a
r
a
,
T
u
r
k
e
y
,
M
a
r
1
9
9
3
J
u
n
1
9
9
3
2
9
c
h
i
l
d
r
e
n
w
h
o
h
a
d
G
I
s
y
m
p
t
o
m
s
a
n
d
r
e
p
o
r
t
e
d
t
o
t
h
e
d
a
y
s
u
r
g
e
r
y
c
l
i
n
i
c
,
t
h
e
l
a
t
t
e
r
f
o
r
m
i
n
o
r
o
u
t
p
a
t
i
e
n
t
s
u
r
g
i
c
a
l
p
r
o
c
e
d
u
r
e
s
o
f
n
o
n
-
G
I
o
r
i
g
i
n
,
a
g
e
r
a
n
g
e
:
1
1
7
,
5
9
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
c
h
i
l
d
r
e
n
w
h
o
u
s
e
d
a
n
t
i
b
i
o
t
i
c
s
,
B
i
s
m
u
t
h
-
c
o
n
t
a
i
n
i
n
g
c
o
m
p
o
u
n
d
s
,
N
S
A
I
D
s
,
o
r
a
n
t
a
c
i
d
s
d
u
r
i
n
g
p
r
e
c
e
d
i
n
g
2
m
o
3
2
c
h
i
l
d
r
e
n
w
i
t
h
o
u
t
G
I
s
y
m
p
t
o
m
s
w
h
o
r
e
p
o
r
t
e
d
t
o
t
h
e
d
a
y
s
u
r
g
e
r
y
c
l
i
n
i
c
,
t
h
e
l
a
t
t
e
r
f
o
r
m
i
n
o
r
o
u
t
p
a
t
i
e
n
t
s
u
r
g
i
c
a
l
o
f
n
o
n
-
G
I
o
r
i
g
i
n
,
a
g
e
r
a
n
g
e
:
1
1
7
y
,
8
1
%
m
a
l
e
C
a
s
e
s
:
a
t
l
e
a
s
t
2
o
f
4
f
o
l
l
o
w
i
n
g
t
e
s
t
s
p
o
s
i
t
i
v
e
:
s
e
r
o
l
o
g
y
,
R
U
T
,
h
i
s
t
o
l
o
g
y
,
b
a
c
t
e
r
i
a
l
c
u
l
t
u
r
e
C
o
n
t
r
o
l
s
:
a
t
l
e
a
s
t
2
o
f
4
f
o
l
l
o
w
i
n
g
t
e
s
t
s
p
o
s
i
t
i
v
e
:
s
e
r
o
l
o
g
y
,
R
U
T
,
h
i
s
t
o
l
o
g
y
,
b
a
c
t
e
r
i
a
l
c
u
l
t
u
r
e
U
A
P
:
0
.
9
3
(
0
.
3
4
2
.
5
5
)
7
G
u
r
a
k
a
n
e
t
a
l
,
2
9
1
9
9
6
P
e
d
i
a
t
r
i
c
G
a
s
t
r
o
e
n
t
e
r
o
l
o
g
y
U
n
i
t
,
A
n
k
a
r
a
,
T
u
r
k
e
y
,
N
o
v
1
9
9
3
M
a
y
1
9
9
4
5
9
c
h
i
l
d
r
e
n
r
e
f
e
r
r
e
d
f
o
r
e
v
a
l
u
a
t
i
o
n
o
f
e
p
i
g
a
s
t
r
i
c
o
r
p
e
r
i
u
m
b
i
l
i
c
a
l
p
a
i
n
a
n
d
/
o
r
n
a
u
s
e
a
,
v
o
m
i
t
i
n
g
,
o
r
r
e
g
u
r
g
i
t
a
t
i
o
n
f
o
r
a
t
l
e
a
s
t
1
m
o
,
a
g
e
r
a
n
g
e
:
5
1
7
y
,
m
e
a
n
:
1
1
.
1
3
.
4
,
5
3
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
u
s
e
o
f
a
n
t
i
b
i
o
t
i
c
s
,
H
2
-
a
n
t
a
g
o
n
i
s
t
s
,
B
i
s
m
u
t
h
-
s
a
l
t
1
m
o
b
e
f
o
r
e
s
e
r
o
l
o
g
i
c
e
x
a
m
i
n
a
t
i
o
n
4
8
c
h
i
l
d
r
e
n
w
h
o
w
e
r
e
s
e
e
n
i
n
t
h
e
o
u
t
p
a
t
i
e
n
t
c
l
i
n
i
c
s
f
o
r
n
o
n
-
G
I
c
o
m
p
l
a
i
n
t
s
,
a
g
e
r
a
n
g
e
:
5
1
7
y
,
m
e
a
n
a
g
e
:
1
0
.
7
3
3
.
6
3
,
5
0
%
m
a
l
e
C
a
s
e
s
:
s
e
r
o
l
o
g
y
(
I
g
G
2
S
D
a
b
o
v
e
t
h
e
m
e
a
n
o
f
a
l
l
n
e
g
a
t
i
v
e
t
i
t
e
r
s
:
O
D
u
n
i
t
s
a
t
4
5
0
n
m
)
C
o
n
t
r
o
l
s
:
s
e
r
o
l
o
g
y
D
y
s
p
e
p
s
i
a
:
1
.
5
5
(
0
.
7
2
3
.
3
4
)
6
H
a
r
d
i
k
a
r
e
t
a
l
,
3
0
1
9
9
6
R
A
P
C
l
i
n
i
c
a
t
R
o
y
a
l
C
h
i
l
d
r
e
n
s
H
o
s
p
i
t
a
l
,
M
e
l
b
o
u
r
n
e
,
A
u
s
t
r
a
l
i
a
,
F
e
b
1
9
9
0
F
e
b
1
9
9
1
1
1
1
c
h
i
l
d
r
e
n
b
e
t
w
e
e
n
5
a
n
d
1
2
y
w
h
o
h
a
d
R
A
P
a
n
d
h
a
d
n
o
t
b
e
e
n
s
e
e
n
p
r
e
v
i
o
u
s
l
y
b
y
a
p
e
d
i
a
t
r
i
c
i
a
n
o
r
s
u
b
s
p
e
c
i
a
l
i
s
t
,
m
e
a
n
a
g
e
:
8
.
5
2
.
1
y
,
3
3
%
m
a
l
e
1
0
3
c
o
n
s
e
c
u
t
i
v
e
c
h
i
l
d
r
e
n
b
e
t
w
e
e
n
5
a
n
d
1
2
y
a
t
t
e
n
d
i
n
g
d
a
y
s
u
r
g
e
r
y
u
n
i
t
f
o
r
c
o
m
m
o
n
s
u
r
g
i
c
a
l
d
i
s
o
r
d
e
r
s
,
o
t
h
e
r
w
i
s
e
i
n
g
o
o
d
h
e
a
l
t
h
a
n
d
w
i
t
h
o
u
t
G
I
s
y
m
p
t
o
m
s
,
m
e
a
n
a
g
e
:
7
.
7
2
.
1
y
,
7
4
%
m
a
l
e
C
a
s
e
s
:
I
g
G
a
n
t
i
b
o
d
y
t
e
s
t
(
8
U
o
f
a
n
t
i
-
H
p
I
g
G
/
m
L
)
C
o
n
t
r
o
l
s
:
I
g
G
a
n
t
i
b
o
d
y
t
e
s
t
R
A
P
:
0
.
2
1
(
0
.
0
5
0
.
8
5
)
(
a
d
j
u
s
t
e
d
f
o
r
g
e
n
d
e
r
,
a
g
e
,
a
n
d
p
a
r
e
n
t
a
l
e
t
h
n
i
c
i
t
y
a
n
d
o
c
c
u
p
a
t
i
o
n
)
7
C
h
o
n
g
e
t
a
l
,
3
1
1
9
9
5
G
I
D
i
s
e
a
s
e
O
u
t
p
a
t
i
e
n
t
C
l
i
n
i
c
,
J
W
h
i
t
c
o
m
b
,
R
i
l
e
y
H
o
s
p
i
t
a
l
f
o
r
C
h
i
l
d
r
e
n
,
I
n
d
i
a
n
a
U
n
i
v
e
r
s
i
t
y
,
I
N
,
J
a
n
1
9
9
1
D
e
c
1
9
9
3
2
1
8
c
h
i
l
d
r
e
n
w
h
o
f
u
l
l
l
e
d
c
r
i
t
e
r
i
a
o
f
R
A
P
a
n
d
w
e
r
e
s
e
e
n
i
n
t
h
e
G
I
d
i
s
e
a
s
e
o
u
t
p
a
t
i
e
n
t
c
l
i
n
i
c
(
R
A
P
g
r
o
u
p
)
,
a
g
e
r
a
n
g
e
:
3
1
8
y
,
m
e
a
n
a
g
e
:
9
.
5
y
,
4
9
%
m
a
l
e
2
3
8
c
h
i
l
d
r
e
n
,
n
o
t
f
u
l
l
l
i
n
g
c
r
i
t
e
r
i
a
o
f
R
A
P
,
w
h
o
w
e
r
e
s
e
e
n
i
n
t
h
e
G
I
d
i
s
e
a
s
e
o
u
t
p
a
t
i
e
n
t
c
l
i
n
i
c
(
n
o
n
-
R
A
P
g
r
o
u
p
)
a
g
e
r
a
n
g
e
:
3
1
8
y
,
m
e
a
n
a
g
e
:
9
.
8
y
,
5
5
%
m
a
l
e
C
a
s
e
s
:
s
e
r
o
l
o
g
y
C
o
n
t
r
o
l
s
:
s
e
r
o
l
o
g
y
R
A
P
:
1
.
8
0
(
1
.
0
5
3
.
1
0
)
5
M
e
n
d
e
z
N
i
e
t
o
e
t
a
l
,
3
2
1
9
9
4
G
a
s
t
r
o
e
n
t
e
r
o
l
o
g
y
D
e
p
a
r
t
m
e
n
t
,
N
a
t
i
o
n
a
l
P
e
d
i
a
t
r
i
c
I
n
s
t
i
t
u
t
e
o
f
M
e
x
i
c
o
,
J
a
n
J
u
n
1
9
9
3
4
0
c
h
i
l
d
r
e
n
r
e
f
e
r
r
e
d
f
o
r
r
e
c
u
r
r
e
n
t
a
b
d
o
m
i
n
a
l
p
a
i
n
,
a
g
e
r
a
n
g
e
5
1
8
y
,
m
e
a
n
a
g
e
:
1
0
.
3
y
4
0
h
e
a
l
t
h
y
c
h
i
l
d
r
e
n
w
i
t
h
o
u
t
G
I
c
o
m
p
l
a
i
n
t
s
C
a
s
e
s
:
h
i
s
t
o
l
o
g
y
a
n
d
r
a
p
i
d
u
r
e
a
s
e
t
e
s
t
C
o
n
t
r
o
l
s
:
E
L
I
S
A
(
O
D
o
f
2
S
D
o
f
t
h
e
m
e
a
n
o
f
h
e
a
l
t
h
y
c
h
i
l
d
r
e
n
)
R
A
P
:
2
1
.
0
0
(
4
.
4
5
9
9
.
0
8
)
3
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e657
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
T
A
B
L
E
1
C
o
n
t
i
n
u
e
d
S
o
u
r
c
e
S
e
t
t
i
n
g
,
P
l
a
c
e
,
C
o
u
n
t
r
y
,
P
e
r
i
o
d
C
a
s
e
P
a
t
i
e
n
t
s
C
o
n
t
r
o
l
S
u
b
j
e
c
t
s
D
i
a
g
n
o
s
t
i
c
T
e
s
t
U
s
e
d
f
o
r
D
e
t
e
r
m
i
n
a
t
i
o
n
o
f
H
p
y
l
o
r
i
I
n
f
e
c
t
i
o
n
(
C
u
t
o
f
f
P
o
i
n
t
)
O
R
(
9
5
%
C
I
)
Q
u
a
l
i
t
y
S
c
o
r
e
v
a
n
d
e
r
M
e
e
r
e
t
a
l
,
3
3
1
9
9
2
A
c
a
d
e
m
i
c
H
o
s
p
i
t
a
l
M
a
a
s
t
r
i
c
h
t
,
N
e
t
h
e
r
l
a
n
d
s
,
d
u
r
i
n
g
6
-
m
o
p
e
r
i
o
d
8
2
c
h
i
l
d
r
e
n
b
e
t
w
e
e
n
5
.
5
a
n
d
1
2
.
0
y
,
w
i
t
h
a
t
l
e
a
s
t
a
6
-
m
o
p
e
r
i
o
d
o
f
R
A
P
o
f
u
n
k
n
o
w
n
o
r
i
g
i
n
,
a
t
t
a
c
k
s
o
f
p
a
i
n
v
a
r
y
i
n
g
i
n
s
e
v
e
r
i
t
y
,
d
u
r
a
t
i
o
n
,
a
n
d
f
r
e
q
u
e
n
c
y
,
s
o
m
e
t
i
m
e
s
a
c
c
o
m
p
a
n
i
e
d
b
y
v
e
g
e
t
a
t
i
v
e
s
y
m
p
t
o
m
s
s
u
c
h
a
s
p
a
l
e
n
e
s
s
,
n
a
u
s
e
a
,
o
r
v
o
m
i
t
i
n
g
,
m
e
a
n
a
g
e
:
1
0
.
8
y
,
3
4
%
m
a
l
e
3
9
p
r
e
o
p
e
r
a
t
i
v
e
c
h
i
l
d
r
e
n
o
r
c
h
i
l
d
r
e
n
a
t
t
e
n
d
i
n
g
t
h
e
o
u
t
p
a
t
i
e
n
t
c
l
i
n
i
c
s
f
o
r
o
t
h
e
r
t
h
a
n
G
I
d
i
s
e
a
s
e
s
,
m
e
a
n
a
g
e
:
6
.
6
y
,
6
4
%
m
a
l
e
C
a
s
e
s
:
E
L
I
S
A
(
1
.
4
0
O
D
u
n
i
t
s
)
C
o
n
t
r
o
l
s
:
E
L
I
S
A
R
A
P
:
1
.
7
0
(
0
.
3
4
8
.
7
3
)
4
M
u
k
h
e
r
j
e
e
e
t
a
l
,
3
4
2
0
0
5
O
u
t
p
a
t
i
e
n
t
D
e
p
a
r
t
m
e
n
t
o
f
a
t
e
a
c
h
i
n
g
h
o
s
p
i
t
a
l
,
P
u
n
j
a
b
,
I
n
d
i
a
6
8
c
h
i
l
d
r
e
n
3
y
o
f
a
g
e
a
t
t
e
n
d
i
n
g
t
h
e
o
u
t
p
a
t
i
e
n
t
d
e
p
a
r
t
m
e
n
t
o
f
a
t
e
a
c
h
i
n
g
h
o
s
p
i
t
a
l
b
e
c
a
u
s
e
o
f
R
A
P
w
i
t
h
n
o
o
b
v
i
o
u
s
c
a
u
s
e
o
f
p
a
i
n
,
a
g
e
r
a
n
g
e
:
3
1
2
y
,
5
2
%
m
a
l
e
9
0
n
o
r
m
a
l
c
o
n
t
r
o
l
s
u
b
j
e
c
t
s
,
a
g
e
r
a
n
g
e
:
3
1
2
y
,
7
4
%
m
a
l
e
C
a
s
e
s
:
I
g
G
a
n
t
i
b
o
d
y
t
e
s
t
C
o
n
t
r
o
l
s
:
I
g
G
a
n
t
i
b
o
d
y
t
e
s
t
R
A
P
:
1
3
.
6
7
(
5
.
8
8
3
1
.
7
0
)
5
S
e
d
l
a
c
k
o
v
a
e
t
a
l
,
3
5
2
0
0
3
H
o
s
p
i
t
a
l
i
n
M
o
r
v
i
a
,
C
z
e
c
h
R
e
p
u
b
l
i
c
,
1
9
9
4
1
9
9
9
8
2
9
c
h
i
l
d
r
e
n
b
e
t
w
e
e
n
2
a
n
d
1
8
y
,
w
h
o
w
e
r
e
r
e
f
e
r
r
e
d
f
o
r
G
I
e
n
d
o
s
c
o
p
y
b
e
c
a
u
s
e
o
f
R
A
P
a
n
d
/
o
r
d
y
s
p
e
p
s
i
a
2
0
5
A
g
e
-
,
g
e
n
d
e
r
-
,
a
n
d
S
E
S
-
m
a
t
c
h
e
d
c
h
i
l
d
r
e
n
a
t
t
e
n
d
i
n
g
t
h
e
h
o
s
p
i
t
a
l
i
n
M
o
r
v
i
a
f
o
r
o
t
h
e
r
r
e
a
s
o
n
s
t
h
a
n
G
I
c
o
m
p
l
a
i
n
t
s
C
a
s
e
s
:
s
e
r
o
l
o
g
y
C
o
n
t
r
o
l
s
:
s
e
r
o
l
o
g
y
U
n
s
p
e
c
i
e
d
(
s
y
m
p
t
o
m
a
t
i
c
)
:
6
.
2
0
4
C
a
m
o
r
l
i
n
g
a
e
t
a
l
,
5
5
1
9
9
8
N
a
t
i
o
n
a
l
M
e
d
i
c
a
l
C
e
n
t
e
r
o
f
t
h
e
I
n
s
t
i
t
u
t
o
M
e
x
i
c
a
n
o
d
e
l
S
e
g
u
r
o
R
o
y
a
l
,
M
e
x
i
c
o
C
i
t
y
,
M
e
x
i
c
o
,
J
a
n
1
9
9
5
S
e
p
1
9
9
6
8
2
c
o
n
s
e
c
u
t
i
v
e
c
h
i
l
d
r
e
n
s
e
e
k
i
n
g
m
e
d
i
c
a
l
a
t
t
e
n
t
i
o
n
b
e
c
a
u
s
e
o
f
R
A
P
,
a
g
e
r
a
n
g
e
:
1
1
7
y
,
m
e
a
n
a
g
e
i
n
f
e
c
t
e
d
c
a
s
e
s
:
9
.
1
3
.
9
y
,
4
2
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
c
h
i
l
d
r
e
n
w
h
o
r
e
c
e
i
v
e
d
a
n
t
i
b
i
o
t
i
c
s
,
H
2
b
l
o
c
k
e
r
s
,
o
r
p
r
o
t
o
n
p
u
m
p
i
n
h
i
b
i
t
o
r
s
d
u
r
i
n
g
t
h
e
p
r
e
v
i
o
u
s
3
0
d
2
4
6
a
g
e
-
a
n
d
g
e
n
d
e
r
-
m
a
t
c
h
e
d
,
a
s
y
m
p
t
o
m
a
t
i
c
p
a
t
i
e
n
t
s
s
e
l
e
c
t
e
d
u
s
i
n
g
a
m
a
s
t
e
r
s
a
m
p
l
i
n
g
f
r
a
m
e
b
a
s
e
d
o
n
g
e
n
e
r
a
l
p
o
p
u
l
a
t
i
o
n
c
e
n
s
u
s
d
a
t
a
,
a
g
e
r
a
n
g
e
:
2
1
7
y
,
m
e
a
n
a
g
e
i
n
f
e
c
t
e
d
c
o
n
t
r
o
l
s
:
1
0
.
6
3
.
7
y
,
3
5
%
m
a
l
e
C
a
s
e
s
:
E
L
I
S
A
(
m
e
a
n
v
a
l
u
e
3
S
D
o
f
t
h
e
O
D
o
f
3
0
u
n
i
n
f
e
c
t
e
d
p
a
t
i
e
n
t
s
)
C
o
n
t
r
o
l
s
:
E
L
I
S
A
R
A
P
:
2
.
0
2
(
1
.
2
0
3
.
3
8
)
3
M
a
s
o
o
d
p
o
o
r
e
t
a
l
,
5
3
2
0
0
8
G
u
i
d
a
n
c
e
s
c
h
o
o
l
s
i
n
R
a
f
s
a
n
j
a
n
C
i
t
y
,
I
r
a
n
,
J
a
n
2
0
0
6
J
a
n
2
0
0
7
4
0
c
h
i
l
d
r
e
n
f
u
l
l
l
i
n
g
c
r
i
t
e
r
i
a
o
f
R
A
P
,
a
t
t
e
n
d
i
n
g
t
h
e
g
u
i
d
a
n
c
e
s
c
h
o
o
l
,
m
e
a
n
a
g
e
:
1
2
.
7
1
.
0
y
,
5
0
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
c
h
i
l
d
r
e
n
w
h
o
r
e
c
e
i
v
e
d
a
n
t
i
b
i
o
t
i
c
t
r
e
a
t
m
e
n
t
,
H
2
b
l
o
c
k
e
r
s
,
o
r
p
r
o
t
o
n
p
u
m
p
i
n
h
i
b
i
t
o
r
s
b
e
f
o
r
e
e
n
t
e
r
i
n
g
s
t
u
d
y
6
0
r
a
n
d
o
m
l
y
s
e
l
e
c
t
e
d
,
a
g
e
-
,
s
c
h
o
o
l
-
,
a
n
d
g
e
n
d
e
r
-
m
a
t
c
h
e
d
h
e
a
l
t
h
y
c
h
i
l
d
r
e
n
w
h
o
h
a
d
n
o
c
l
i
n
i
c
a
l
m
a
n
i
f
e
s
t
a
t
i
o
n
s
o
f
R
A
P
a
n
d
w
e
r
e
n
o
r
m
a
l
o
n
p
h
y
s
i
c
a
l
e
x
a
m
i
n
a
t
i
o
n
,
m
e
a
n
a
g
e
:
1
2
.
9
1
.
1
y
,
5
0
%
m
a
l
e
C
a
s
e
s
:
H
p
S
A
E
L
I
S
A
s
t
o
o
l
a
n
t
i
g
e
n
t
e
s
t
(
a
n
a
b
s
o
r
b
a
n
c
e
a
t
4
5
0
/
6
3
0
o
f
0
.
1
2
0
)
C
o
n
t
r
o
l
s
:
H
p
S
A
E
L
I
S
A
s
t
o
o
l
a
n
t
i
g
e
n
t
e
s
t
R
A
P
:
2
.
0
0
(
0
.
8
5
4
.
7
3
)
7
D
e
v
a
n
a
r
a
y
a
n
a
e
t
a
l
,
5
4
2
0
0
7
S
c
h
o
o
l
i
n
G
a
m
p
a
h
a
D
i
s
t
r
i
c
t
o
f
S
r
i
L
a
n
k
a
5
5
c
h
i
l
d
r
e
n
i
d
e
n
t
i
e
d
a
s
f
u
l
l
l
i
n
g
c
r
i
t
e
r
i
a
o
f
R
A
P
w
e
r
e
r
e
c
r
u
i
t
e
d
d
u
r
i
n
g
a
s
c
h
o
o
l
s
u
r
v
e
y
,
m
e
a
n
a
g
e
:
7
.
9
3
y
,
a
g
e
r
a
n
g
e
:
5
1
5
y
,
4
1
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
c
h
i
l
d
r
e
n
w
h
o
r
e
c
e
i
v
e
d
a
n
t
i
b
i
o
t
i
c
s
,
a
c
i
d
s
u
p
p
r
e
s
s
i
o
n
,
o
r
a
n
t
i
H
p
y
l
o
r
i
t
h
e
r
a
p
y
w
i
t
h
i
n
3
m
o
b
e
f
o
r
e
i
n
c
l
u
s
i
o
n
2
0
h
e
a
l
t
h
y
c
h
i
l
d
r
e
n
r
e
c
r
u
i
t
e
d
f
r
o
m
t
h
e
s
a
m
e
a
r
e
a
,
m
e
a
n
a
g
e
:
9
.
0
2
.
7
y
,
a
g
e
r
a
n
g
e
:
5
1
5
y
,
5
0
%
m
a
l
e
C
a
s
e
s
:
M
i
c
r
o
w
e
l
l
-
b
a
s
e
d
E
I
A
t
h
a
t
d
e
t
e
c
t
e
d
H
p
y
l
o
r
i
a
n
t
i
g
e
n
s
i
n
s
t
o
o
l
(
a
b
s
o
r
b
a
n
c
e
v
a
l
u
e
1
9
0
)
C
o
n
t
r
o
l
s
:
a
n
t
i
g
e
n
s
i
n
s
t
o
o
l
R
A
P
:
1
.
0
3
(
0
.
0
9
1
2
.
0
0
)
4
R
U
T
i
n
d
i
c
a
t
e
s
r
a
p
i
d
u
r
e
a
s
e
t
e
s
t
;
1
3
C
-
U
B
T
,
1
3
C
-
u
r
e
a
b
r
e
a
t
h
t
e
s
t
;
E
I
A
,
e
n
z
y
m
e
i
m
m
u
n
o
a
s
s
a
y
;
E
L
I
S
A
,
e
n
z
y
m
e
-
l
i
n
k
e
d
i
m
m
u
n
o
s
o
r
b
e
n
t
a
s
s
a
y
;
S
E
S
,
s
o
c
i
o
e
c
o
n
o
m
i
c
s
t
a
t
u
s
;
I
B
D
,
i
r
r
i
t
a
b
l
e
b
o
w
e
l
s
y
n
d
r
o
m
e
;
U
R
O
,
o
r
a
l
r
e
h
y
d
r
a
t
i
o
n
u
n
i
t
;
N
S
A
I
D
,
n
o
n
s
t
e
r
o
i
d
a
l
a
n
t
i
-
i
n
a
m
m
a
t
o
r
y
d
r
u
g
;
O
D
,
o
p
t
i
c
d
e
n
s
i
t
y
.
e658 SPEE et al
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
T
A
B
L
E
2
S
t
u
d
y
C
h
a
r
a
c
t
e
r
i
s
t
i
c
s
o
f
I
n
c
l
u
d
e
d
C
r
o
s
s
-
S
e
c
t
i
o
n
a
l
S
t
u
d
i
e
s
S
o
u
r
c
e
S
e
t
t
i
n
g
,
P
l
a
c
e
,
C
o
u
n
t
r
y
,
P
e
r
i
o
d
S
t
u
d
y
P
o
p
u
l
a
t
i
o
n
D
i
a
g
n
o
s
t
i
c
T
e
s
t
U
s
e
d
f
o
r
D
e
t
e
r
m
i
n
a
t
i
o
n
o
f
H
p
y
l
o
r
i
I
n
f
e
c
t
i
o
n
(
C
u
t
o
f
f
P
o
i
n
t
)
N
(
P
r
e
v
a
l
e
n
c
e
)
O
R
(
9
5
%
C
I
)
Q
u
a
l
i
t
y
S
c
o
r
e
O
z
e
n
e
t
a
l
,
3
6
2
0
0
6
P
r
e
s
c
h
o
o
l
s
a
n
d
s
c
h
o
o
l
s
,
T
u
r
k
e
y
,
2
0
0
4
1
3
6
c
h
i
l
d
r
e
n
w
h
o
p
a
r
t
i
c
i
p
a
t
e
d
i
n
a
p
r
e
v
i
o
u
s
s
t
u
d
y
(
E
r
t
e
m
e
t
a
l
)
,
m
e
a
n
a
g
e
:
1
3
.
4
5
1
.
9
0
y
,
r
a
n
g
e
:
8
1
7
y
,
4
7
%
m
a
l
e
1
3
C
-
U
B
T
(
a
c
h
a
n
g
e
i
n
t
h
e
1
3
C
v
a
l
u
e
o
v
e
r
b
a
s
e
l
i
n
e
o
f
)
1
3
6
(
5
6
.
6
%
)
R
A
P
:
1
.
0
5
(
0
.
4
8
2
.
2
8
)
U
A
P
:
0
.
4
9
(
0
.
1
7
1
.
3
8
)
V
o
m
i
t
i
n
g
/
d
i
a
r
r
h
e
a
:
1
.
8
0
(
0
.
6
8
4
.
7
4
)
D
y
s
p
e
p
s
i
a
:
1
.
0
6
(
0
.
4
4
2
.
5
1
)
9
T
i
n
d
b
e
r
g
e
t
a
l
,
3
7
2
0
0
5
1
1
l
o
c
a
l
p
u
b
l
i
c
s
c
h
o
o
l
s
i
n
S
t
o
c
k
h
o
l
m
,
S
w
e
d
e
n
,
J
a
n
1
9
9
8
6
9
5
c
h
i
l
d
r
e
n
,
b
e
t
w
e
e
n
1
0
a
n
d
1
2
y
,
a
t
t
e
n
d
i
n
g
1
o
f
t
h
e
p
a
r
t
i
c
i
p
a
t
i
n
g
l
o
c
a
l
p
u
b
l
i
c
s
c
h
o
o
l
s
,
m
e
a
n
a
g
e
:
1
1
.
2
1
.
0
y
,
r
a
n
g
e
:
9
1
3
y
,
4
8
%
m
a
l
e
P
o
s
i
t
i
v
e
i
f
E
L
I
S
A
(
0
.
2
2
O
D
v
a
l
u
e
)
p
o
s
i
t
i
v
e
a
n
d
a
t
l
e
a
s
t
1
o
f
2
o
f
t
h
e
f
o
l
l
o
w
i
n
g
t
e
s
t
s
w
a
s
p
o
s
i
t
i
v
e
:
i
m
m
u
n
o
b
l
o
t
(
C
a
g
A
1
1
6
k
D
a
,
V
a
c
A
8
9
k
D
a
)
,
1
3
C
-
U
B
T
6
9
5
(
1
6
.
1
%
)
R
A
P
:
1
.
0
0
(
0
.
5
0
2
.
1
0
)
U
A
P
:
0
.
5
0
(
0
.
3
0
0
.
8
0
)
R
e
g
u
r
g
i
t
a
t
i
o
n
:
0
.
5
0
(
0
.
3
0
0
.
9
0
)
C
o
n
s
t
i
p
a
t
i
o
n
:
0
.
7
0
(
0
.
4
0
1
.
5
0
)
W
e
e
k
l
y
A
P
:
1
.
5
0
(
0
.
7
0
3
.
3
0
)
L
o
o
s
e
s
t
o
o
l
s
:
0
.
9
0
(
0
.
5
0
1
.
6
0
)
(
a
d
j
u
s
t
e
d
f
o
r
a
g
e
,
g
e
n
d
e
r
,
S
E
S
,
f
a
m
i
l
y
s
i
z
e
,
a
n
d
i
m
m
i
g
r
a
n
t
b
a
c
k
g
r
o
u
n
d
)
8
L
i
n
e
t
a
l
,
3
8
2
0
0
5
1
p
r
i
m
a
r
y
s
c
h
o
o
l
,
D
a
n
s
h
u
e
i
,
T
a
i
p
e
i
,
T
a
i
w
a
n
,
2
0
0
3
2
8
9
r
a
n
d
o
m
l
y
s
e
l
e
c
t
e
d
g
r
a
d
e
s
1
t
o
6
p
r
i
m
a
r
y
s
c
h
o
o
l
s
t
u
d
e
n
t
s
w
h
o
v
o
l
u
n
t
e
e
r
e
d
f
o
r
b
l
o
o
d
-
t
e
s
t
s
f
o
r
H
p
y
l
o
r
i
I
g
G
a
n
d
a
n
t
i
h
e
p
a
t
i
t
i
s
A
a
n
t
i
b
o
d
y
,
m
e
a
n
a
g
e
:
9
.
2
1
,
5
1
%
m
a
l
e
E
L
I
S
A
2
8
9
(
2
1
.
5
%
)
R
A
P
:
0
.
8
9
(
0
.
4
7
1
.
6
7
)
6
B
o
d
e
e
t
a
l
,
3
9
1
9
9
8
S
c
h
o
o
l
s
i
n
U
l
m
,
S
o
u
t
h
e
r
n
G
e
r
m
a
n
y
,
1
9
9
6
9
4
5
p
r
e
s
c
h
o
o
l
c
h
i
l
d
r
e
n
,
a
g
e
d
5
8
,
w
h
o
w
e
r
e
e
x
a
m
i
n
e
d
f
o
r
s
c
h
o
o
l
t
n
e
s
s
b
y
t
h
e
P
u
b
l
i
c
H
e
a
l
t
h
S
e
r
v
i
c
e
,
m
e
a
n
a
g
e
:
5
.
8
4
y
,
r
a
n
g
e
:
5
8
y
,
5
0
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
c
h
i
l
d
r
e
n
w
h
o
r
e
c
e
i
v
e
d
a
n
t
i
b
i
o
t
i
c
t
r
e
a
t
m
e
n
t
w
i
t
h
i
n
t
h
e
l
a
s
t
4
w
k
1
3
C
-
U
B
T
(
d
i
f
f
e
r
e
n
c
e
b
e
t
w
e
e
n
b
a
s
e
l
i
n
e
1
3
C
O
2
/
1
2
C
O
2
r
a
t
i
o
a
n
d
3
0
m
i
n
r
a
t
i
o
)
9
4
5
(
1
3
.
7
%
)
U
A
P
:
0
.
4
8
(
0
.
3
3
0
.
7
2
)
V
o
m
i
t
i
n
g
:
0
.
4
5
(
0
.
2
9
0
.
7
2
)
D
i
a
r
r
h
e
a
:
0
.
3
1
(
0
.
2
0
0
.
4
8
)
8
R
a
h
m
a
n
e
t
a
l
,
4
0
1
9
9
8
P
e
r
i
u
r
b
a
n
c
o
m
m
u
n
i
t
y
a
d
j
a
c
e
n
t
t
o
t
h
e
c
a
p
i
t
a
l
c
i
t
y
o
f
B
a
n
g
l
a
d
e
s
h
,
J
a
n
O
c
t
1
9
9
3
1
5
1
c
h
i
l
d
r
e
n
w
h
o
w
e
r
e
f
r
e
e
f
r
o
m
s
y
s
t
e
m
i
c
i
n
f
e
c
t
i
o
n
c
a
u
s
i
n
g
d
i
a
r
r
h
e
a
,
r
e
s
p
i
r
a
t
o
r
y
i
n
f
e
c
t
i
o
n
,
a
n
d
o
t
h
e
r
i
n
f
e
c
t
i
o
n
s
a
t
t
i
m
e
o
f
e
n
r
o
l
l
m
e
n
t
,
m
e
a
n
a
g
e
H
p
p
o
s
:
8
.
9
7
.
0
m
o
,
H
p
n
e
g
:
9
.
9
6
.
7
,
r
a
n
g
e
:
1
2
3
m
o
,
5
0
%
m
a
l
e
1
3
C
-
U
B
T
(
t
h
e
e
x
c
e
s
s
o
v
e
r
b
a
s
e
l
i
n
e
v
a
l
u
e
o
f
1
3
C
O
2
w
a
s
e
x
p
r
e
s
s
e
d
a
s
p
a
r
t
s
p
e
r
t
h
o
u
s
a
n
d
(
%
)
;
a
c
u
t
o
f
f
p
o
i
n
t
o
f
5
i
n
t
h
e
r
a
t
i
o
w
a
s
r
e
g
a
r
d
e
d
a
s
p
o
s
i
t
i
v
e
)
1
5
1
(
4
5
.
0
%
)
D
i
a
r
r
h
e
a
:
(
a
f
t
e
r
1
m
o
)
:
0
.
9
1
(
0
.
2
0
4
.
2
2
)
D
i
a
r
r
h
e
a
(
a
f
t
e
r
6
m
o
)
:
1
.
0
8
(
0
.
5
6
2
.
0
9
)
6
G
r
i
m
m
e
t
a
l
,
4
1
2
0
0
3
S
c
h
o
o
l
s
i
n
A
s
c
h
a
f
f
e
n
b
u
r
g
a
n
d
s
u
r
r
o
u
n
d
i
n
g
s
,
G
e
r
m
a
n
y
,
s
c
h
o
o
l
y
e
a
r
1
9
9
7
/
1
9
9
8
5
4
0
s
c
h
o
o
l
c
h
i
l
d
r
e
n
,
a
g
e
d
7
9
,
1
1
1
5
,
a
n
d
1
6
2
0
,
w
h
o
v
o
l
u
n
t
a
r
i
l
y
t
o
o
k
p
a
r
t
,
a
g
e
r
a
n
g
e
:
7
2
0
y
,
4
6
%
m
a
l
e
1
3
C
-
U
B
T
(
t
h
e
D
O
B
v
a
l
u
e
s
w
e
r
e
e
l
e
v
a
t
e
d
a
b
o
v
e
3
.
5
)
5
4
0
P
r
e
v
a
l
e
n
c
e
9
.
4
U
A
P
:
5
.
4
3
(
2
.
6
4
1
1
.
1
3
)
7
M
c
C
a
l
l
i
o
n
e
t
a
l
,
4
2
1
9
9
5
R
o
y
a
l
B
e
l
f
a
s
t
H
o
s
p
i
t
a
l
f
o
r
S
i
c
k
C
h
i
l
d
r
e
n
,
I
r
e
l
a
n
d
,
d
u
r
i
n
g
6
-
m
o
p
e
r
i
o
d
4
3
9
c
h
i
l
d
r
e
n
a
t
t
e
n
d
i
n
g
f
o
r
r
o
u
t
i
n
e
d
a
y
s
u
r
g
e
r
y
,
m
e
a
n
a
g
e
:
7
.
3
y
,
r
a
n
g
e
:
4
1
3
y
E
L
I
S
A
4
3
9
(
2
8
.
9
%
)
R
A
P
:
1
.
1
0
(
0
.
6
3
1
.
9
0
)
6
M
a
g
i
s
t
a
e
t
a
l
,
4
3
2
0
0
5
D
e
p
a
r
t
m
e
n
t
o
f
P
e
d
i
a
t
r
i
c
G
a
s
t
r
o
e
n
t
e
r
o
l
o
g
y
,
U
n
i
v
e
r
s
i
t
y
o
f
B
a
r
i
,
I
t
a
l
y
,
1
9
9
8
2
0
0
0
5
2
c
h
i
l
d
r
e
n
i
n
w
h
o
m
i
n
f
e
c
t
i
o
n
w
a
s
s
u
c
c
e
s
s
f
u
l
l
y
e
r
a
d
i
c
a
t
e
d
p
r
e
v
i
o
u
s
l
y
,
m
e
a
n
a
g
e
:
1
2
y
,
r
a
n
g
e
:
4
.
9
1
9
.
0
y
,
5
2
%
m
a
l
e
P
o
s
i
t
i
v
e
w
h
e
n
a
l
l
3
t
e
s
t
s
w
e
r
e
p
o
s
i
t
i
v
e
:
1
3
C
-
U
B
T
(
c
h
a
n
g
e
o
f
3
.
5
p
e
r
t
h
o
u
s
a
n
d
o
r
m
o
r
e
r
e
l
a
t
e
d
t
o
b
a
s
e
l
i
n
e
s
i
g
n
a
l
)
,
R
U
T
,
a
n
d
h
i
s
t
o
l
o
g
y
5
2
(
2
8
.
8
%
)
E
p
i
g
a
s
t
r
i
c
p
a
i
n
:
3
.
2
0
(
0
.
7
7
1
3
.
3
5
)
N
a
u
s
e
a
:
4
.
3
8
(
0
.
6
5
2
9
.
4
0
)
R
A
P
:
1
.
2
9
(
0
.
2
8
6
.
0
1
)
H
a
l
i
t
o
s
i
s
:
(
4
.
2
8
(
0
.
6
5
2
9
.
4
0
)
P
o
s
t
p
r
a
n
d
i
a
l
f
u
l
l
n
e
s
s
:
1
.
2
7
(
0
.
2
1
7
.
7
9
)
6
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e659
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
T
A
B
L
E
2
C
o
n
t
i
n
u
e
d
S
o
u
r
c
e
S
e
t
t
i
n
g
,
P
l
a
c
e
,
C
o
u
n
t
r
y
,
P
e
r
i
o
d
S
t
u
d
y
P
o
p
u
l
a
t
i
o
n
D
i
a
g
n
o
s
t
i
c
T
e
s
t
U
s
e
d
f
o
r
D
e
t
e
r
m
i
n
a
t
i
o
n
o
f
H
p
y
l
o
r
i
I
n
f
e
c
t
i
o
n
(
C
u
t
o
f
f
P
o
i
n
t
)
N
(
P
r
e
v
a
l
e
n
c
e
)
O
R
(
9
5
%
C
I
)
Q
u
a
l
i
t
y
S
c
o
r
e
E
r
t
e
m
e
t
a
l
,
4
4
2
0
0
3
P
r
e
s
c
h
o
o
l
s
a
n
d
s
c
h
o
o
l
s
,
T
u
r
k
e
y
3
2
7
p
r
e
s
c
h
o
o
l
a
n
d
s
c
h
o
o
l
-
a
g
e
d
h
e
a
l
t
h
y
c
h
i
l
d
r
e
n
,
m
e
a
n
a
g
e
:
8
.
2
2
.
1
y
,
r
a
n
g
e
:
3
1
2
y
,
5
2
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
c
h
i
l
d
r
e
n
w
h
o
r
e
c
e
i
v
e
d
o
r
a
l
o
r
p
a
r
e
n
t
e
r
a
l
a
n
t
i
b
i
o
t
i
c
s
w
i
t
h
i
n
4
w
k
b
e
f
o
r
e
t
h
e
i
n
v
e
s
t
i
g
a
t
i
o
n
1
3
C
-
U
B
T
(
a
c
h
a
n
g
e
i
n
t
h
e
1
3
C
v
a
l
u
e
o
v
e
r
b
a
s
e
l
i
n
e
o
f
)
3
2
7
(
4
9
.
5
%
)
R
A
P
:
1
.
3
3
(
9
5
%
C
I
c
o
u
l
d
n
o
t
b
e
c
a
l
c
u
l
a
t
e
d
)
5
O
D
o
n
o
h
o
e
e
t
a
l
,
4
5
1
9
9
5
7
s
c
h
o
o
l
s
i
n
1
c
e
n
t
r
a
l
L
o
n
d
o
n
D
i
s
t
r
i
c
t
,
E
n
g
l
a
n
d
6
4
0
s
t
a
t
e
s
c
h
o
o
l
a
n
d
p
r
i
v
a
t
e
s
c
h
o
o
l
c
h
i
l
d
r
e
n
w
h
o
v
o
l
u
n
t
a
r
i
l
y
p
a
r
t
i
c
i
p
a
t
e
d
,
m
e
a
n
a
g
e
:
9
.
1
5
y
,
r
a
n
g
e
:
4
1
3
y
,
6
0
%
m
a
l
e
I
g
G
E
L
I
S
A
(
1
0
U
/
m
L
)
6
4
0
(
1
6
.
7
%
)
R
A
P
:
0
.
4
9
(
0
.
2
3
1
.
0
7
)
7
B
o
d
e
e
t
a
l
,
4
6
2
0
0
3
S
c
h
o
o
l
s
i
n
U
l
m
,
E
r
b
a
c
h
,
a
n
d
E
h
i
n
g
e
n
,
s
o
u
t
h
G
e
r
m
a
n
y
,
J
a
n
J
u
l
1
9
9
7
1
1
4
3
p
r
e
s
c
h
o
o
l
c
h
i
l
d
r
e
n
a
g
e
d
5
8
y
w
h
o
w
e
r
e
t
o
a
t
t
e
n
d
r
s
t
g
r
a
d
e
a
n
d
u
n
d
e
r
w
e
n
t
a
n
s
c
h
o
o
l
t
n
e
s
s
e
x
a
m
i
n
a
t
i
o
n
b
y
t
h
e
P
u
b
l
i
c
H
e
a
l
t
h
S
e
r
v
i
c
e
,
m
e
a
n
a
g
e
:
5
.
8
8
y
,
r
a
n
g
e
:
5
8
y
,
4
9
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
c
h
i
l
d
r
e
n
w
h
o
u
s
e
d
a
n
t
i
b
i
o
t
i
c
s
w
i
t
h
i
n
t
h
e
p
a
s
t
4
w
k
1
3
C
-
U
B
T
(
a
c
h
a
n
g
e
o
f
t
h
e
1
3
C
v
a
l
u
e
o
v
e
r
b
a
s
e
l
i
n
e
o
f
)
1
1
4
3
(
1
1
.
3
%
)
R
A
P
:
1
.
6
0
(
0
.
5
0
5
.
5
5
)
(
a
d
j
u
s
t
e
d
f
o
r
n
a
t
i
o
n
a
l
i
t
y
,
s
i
n
g
l
e
-
p
a
r
e
n
t
h
o
u
s
e
h
o
l
d
,
h
i
s
t
o
r
y
o
f
p
e
p
t
i
c
u
l
c
e
r
s
o
f
p
a
r
e
n
t
s
,
a
n
d
h
i
s
t
o
r
y
o
f
G
I
d
i
s
o
r
d
e
r
s
o
f
p
a
r
e
n
t
s
)
8
L
e
a
n
d
r
o
e
t
a
l
,
4
7
2
0
0
5
H
e
a
l
t
h
c
a
r
e
c
e
n
t
e
r
,
F
o
r
a
l
d
e
N
a
v
a
r
r
a
,
S
p
a
i
n
,
J
a
n
2
0
0
3
M
a
r
2
0
0
4
R
a
n
d
o
m
s
a
m
p
l
e
o
f
c
h
i
l
d
r
e
n
a
g
e
d
1
1
4
y
,
v
i
s
i
t
i
n
g
a
r
e
g
u
l
a
r
h
e
a
l
t
h
c
a
r
e
p
r
o
g
r
a
m
,
m
e
a
n
a
g
e
:
6
.
8
9
4
.
2
5
y
,
5
0
.
7
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
a
n
t
i
b
i
o
t
i
c
s
i
n
p
a
s
t
m
o
n
t
h
,
p
r
e
v
i
o
u
s
e
r
a
d
i
c
a
t
i
o
n
t
h
e
r
a
p
y
f
o
r
H
p
y
l
o
r
i
,
c
h
r
o
n
i
c
d
i
s
e
a
s
e
E
I
A
f
o
r
f
e
c
a
l
H
p
y
l
o
r
i
a
n
t
i
g
e
n
;
a
t
4
5
0
n
m
p
o
s
i
t
i
v
e
a
t
D
O
0
.
1
6
0
,
n
e
g
a
t
i
v
e
a
t
D
O
0
.
1
4
0
2
8
4
(
1
5
.
8
%
o
v
e
r
a
l
l
)
1
3
y
:
8
.
4
%
4
9
y
:
1
3
.
9
%
1
0
1
4
y
:
2
4
%
(
P
.
0
5
)
R
A
P
:
7
.
6
6
(
3
.
4
6
1
6
.
9
3
)
6
T
e
l
m
e
s
a
n
i
,
5
1
2
0
0
8
B
o
y
s
s
c
h
o
o
l
i
n
M
a
k
k
a
h
C
i
t
y
,
M
a
k
k
a
h
R
e
g
i
o
n
,
W
e
s
t
e
r
n
S
a
u
d
i
A
r
a
b
i
a
3
1
4
b
o
y
s
,
1
0
3
o
f
w
h
o
m
i
n
i
n
t
e
r
m
e
d
i
a
t
e
l
e
v
e
l
a
n
d
2
1
1
o
f
w
h
o
m
i
n
s
e
c
o
n
d
a
r
y
l
e
v
e
l
,
a
g
e
r
a
n
g
e
:
1
2
1
8
y
,
1
0
0
%
m
a
l
e
;
e
x
c
l
u
d
e
d
:
r
e
c
e
n
t
u
s
e
o
f
a
n
t
i
b
i
o
t
i
c
s
o
r
a
l
l
e
r
g
y
t
o
w
a
r
d
t
h
e
t
e
s
t
m
a
t
e
r
i
a
l
1
4
C
-
U
B
T
(
r
e
s
u
l
t
s
c
a
l
c
u
l
a
t
e
d
u
s
i
n
g
g
r
a
d
e
s
0
,
n
o
t
i
n
f
e
c
t
e
d
;
1
,
b
o
r
d
e
r
l
i
n
e
;
2
,
i
n
f
e
c
t
e
d
;
b
o
r
d
e
r
l
i
n
e
r
e
s
u
l
t
s
r
e
q
u
i
r
e
d
a
r
e
p
e
a
t
t
e
s
t
)
3
1
4
(
2
7
.
4
%
)
R
A
P
:
1
2
.
3
5
(
6
.
3
0
2
4
.
2
2
)
6
S
i
a
i
e
t
a
l
,
5
2
2
0
0
8
S
c
h
o
o
l
s
i
n
t
h
e
C
a
p
-
B
o
n
r
e
g
i
o
n
,
N
a
b
e
u
l
G
o
v
e
r
n
o
r
s
h
i
p
,
T
u
n
e
s
i
a
1
0
5
5
r
a
n
d
o
m
l
y
s
e
l
e
c
t
e
d
(
1
s
t
,
1
0
t
h
,
2
0
t
h
,
e
t
c
)
r
s
t
-
g
r
a
d
e
p
r
i
m
a
r
y
s
c
h
o
o
l
c
h
i
l
d
r
e
n
b
e
l
o
n
g
i
n
g
t
o
t
h
e
r
e
c
r
u
i
t
m
e
n
t
p
o
p
u
l
a
t
i
o
n
s
o
f
1
3
h
e
a
l
t
h
c
a
r
e
c
e
n
t
e
r
s
d
a
t
a
b
a
s
e
s
,
8
1
3
c
h
i
l
d
r
e
n
o
f
6
y
,
2
4
2
c
h
i
l
d
r
e
n
o
f
7
y
,
4
9
.
9
%
m
a
l
e
I
g
G
E
L
I
S
A
1
0
5
5
(
5
1
.
4
%
)
U
A
P
:
1
.
4
5
(
1
.
0
1
2
.
5
0
)
(
a
d
j
u
s
t
e
d
f
o
r
h
o
u
s
e
h
o
l
d
m
e
m
b
e
r
s
5
,
b
o
t
t
l
e
w
e
a
n
i
n
g
1
8
m
o
p
l
a
t
e
/
b
e
d
-
s
h
a
r
i
n
g
,
S
E
S
,
a
b
d
o
m
i
n
a
l
p
a
i
n
,
v
o
m
i
t
i
n
g
)
V
o
m
i
t
i
n
g
:
1
.
6
3
(
1
.
0
4
2
.
5
4
)
9
E
L
I
S
A
i
n
d
i
c
a
t
e
s
e
n
z
y
m
e
-
l
i
n
k
e
d
i
m
m
u
n
o
s
o
r
b
e
n
t
a
s
s
a
y
;
O
D
,
o
p
t
i
c
d
e
n
s
i
t
y
;
D
O
B
,
d
e
l
t
a
o
v
e
r
b
a
s
e
l
i
n
e
.
e660 SPEE et al
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
association between epigastric pain
and H pylori infection. In total, 2 of 3
studies showed a statistically signi-
cant association between epigastric
pain and H pylori infection. This nding
was independent of setting. Further-
more, there is strong evidence that
RAP is not related to H pylori.
The European Pediatric Task Force
4
concluded in their guidelines on man-
agement of H pylori infection that, in
children, H pylori infection is not re-
lated to GI symptoms. Our ndings con-
tradict this assumption but are in
agreement with ndings in adults, for
whom dyspepsia is thought to be
caused by H pylori. Our ndings par-
tially support the Consensus Report
of The European Helicobacter Study
Group; they reported that RAP is not an
indication for a test-and-treat strategy
for H pylori infection in children; how-
ever, children with upper GI symptoms
should be tested after exclusion of
other causes of the symptoms.
6
The nding for an association between
UAP and H pylori infection in referred
children but not in children who were
seen in primary care is in agreement
with our nding of evidence that RAP
and Hpylori are not related. Abdominal
pain in a child who sees a general
practitioner (GP) has a different differ-
ential diagnosis than abdominal pain
in a child who is seen in secondary
care. Abdominal pain in primary care
more often will be functional. In a set-
ting where a symptom is dominantly
related to functional disease, an asso-
ciation between the symptom and a
low-prevalent disorder might be too
weak to detect. In addition, a GP will
FIGURE 3
Meta-analysis of case-control studies concerning UAP related to H pylori infection. Events indicates number children with H pylori infection.
FIGURE 4
Meta-analysis of cross-sectional studies concerning UAP related to H pylori infection. Events indicates number children with H pylori infection.
TABLE 3 Study Characteristics of Included Prospective Cohort Study
Source Setting, Place, Country,
Period
Study Population Diagnostic Test Used for
Determination of
H pylori Infection
(Cutoff Point)
Patients Lost to Follow-up,
%
OR (95% CI) Quality
Score
Tindberg et al,
48
1999
Vaccine trial, Southern
part of Sweden,
Stockholm,
19841995
305 children, born in 1984,
who participated in a
pertussis vaccine trial,
starting at 6 mo to 11 y;
mean age at end of
follow-up: 10.9 y (range:
10.512.3 y)
ELISA (0.360 A405 nm),
measured at 6 mo, 8
mo, 10 mo, 18 mo, 2 y,
4 y, and 11 y
Blood samples from 6 to 18
mo of age and at least 1
additional serum sample
drawn at 2, 4, or 11 y of
age were available from
294 children; lost to
follow-up: 11 (3.6%)
RAP (during last 6 mo):
2.0 (0.84.6) UAP
(during childhood):
1.4 (0.72.9) UAP
(last 6 mo):
2.2 (1.24.7)
9
ELISA indicates enzyme-linked immunosorbent assay.
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e661
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
refer only children in whom he sus-
pects underlying disease; therefore, in
referred children, the same symptom
is more likely to be related to a poten-
tial pathogen such as H pylori.
RAP as dened by Apley and Naish
15
is
thought to be related to functional
disease and should therefore theo-
retically preclude H pylori. We found
no evidence for any relation between
RAP by Apley and Naish and H pylori
infection in children in both case-
control studies (OR: 1.21 [95% CI:
0.821.78) and cross-sectional stud-
ies (OR: 1.00 [95% CI: 0.76 1.31). Sub-
group analyses of RAP in different
settings, high-quality studies, and
different geographic locations did
not alter this nding. In low-quality
case-control studies, the association
between RAP and H pylori was clini-
cally and statistically signicant (OR:
2.68 [95% CI: 1.474.89); however, we
believe that this OR is overestimated
because of a biased selection of con-
trol subjects. Whereas in 4 of 5 high-
quality studies case patients and
control subjects were drawn from a
population at a comparable risk for
exposure (ie, H pylori infection), this
was not the case in all of the low-
quality studies. The ORs suggest a se-
lection of control subjects in whom
not only GI symptoms but also H py-
lori infection was precluded. This
might have seriously biased these
outcomes.
After excluding the outlier studies of
Leandro Liberato et al
47
and Telme-
sani,
51
the pooled OR of cross-sectional
studies that evaluated the relation be-
tween RAP and H pylori was 1.00 (95%
CI: 0.761.31). This nding underlines
the absence of a relation between RAP
and H pylori infection in children as
found in the case-control studies. On
the basis of the data presented, we
could not explain the outlying results
of the study of Leandro Liberato et al
47
and Telmesani.
51
RAP is mainly dened by the duration
of abdominal pain. We assume that se-
lecting children with RAP is more than
a selection that is based on duration of
abdominal pain alone. Selection of
children with RAP will implicitly com-
prise the belief of the primary care cli-
nician that RAP in the long-term does
not affect growth and that develop-
ment of the child will be functional and
that in referred children it will com-
prise the (negative) results of previous
investigations. Because of these im-
plicit selection criteria, we assume
that the included children with RAP will
be at high risk for functional disease.
None of these selection mechanisms,
however, was described in the studies
on RAP that were included in this re-
view. That duration of pain may pre-
clude underlying disorders as a result
of the aforementioned mechanisms is
afrmed by the ndings of Yang et al.
18
That population-based study reported
a statistically signicant association
between SRAP (ie, abdominal pain that
met the criteria of Apley and Naish
15
but with a shorter duration in range
from 2 weeks to 3 months) in the epi-
gastric region and H pylori infection.
To our knowledge, this is the rst pub-
lished review to investigate the associ-
ation between GI symptoms in general
and H pylori infection in children. The
results of our review concerning RAP
are consistent with 2 previous system-
atic reviews that reported no obvious
association between RAP and H pylori
infection in children.
8,9
Although our literature search was
comprehensive, some published and
unpublished studies may have been
missed. Also, some information perti-
nent to the review and collected by the
reviewers may not have been provided
in the journal article, although we con-
tacted rst authors to request missing
data with variable success.
Cautious interpretation of pooled ORs
is necessary because we found a large
statistical and clinical heterogeneity
between studies and an overall poor
methodologic quality. Using a best evi-
dence synthesis to summarize the data
could overcome these problems, but
limited data exist on best evidence syn-
theses for observational studies, and
the possibility of misclassifying the re-
sults of studies with a small sample
size is large.
We found that children who are re-
ferred to a gastroenterologist with
UAP or pain in the epigastric region in
general are at two- to threefold higher
risk for H pylori infection than children
without these symptoms. Because we
are not aware of the criteria on which
a GP decides to refer a child with ab-
dominal pain to a pediatric gastroen-
terologist, a more specic clinical pic-
ture has yet to be established. Whether
to screen systematically referred chil-
dren with abdominal (epigastric) pain
depends on effectiveness and adverse
effects of eradication therapy. No opti-
mal treatment has yet been dened.
To conrm, disclaim, or specify our
ndings on UAP and epigastric pain,
additional research is necessary. If
there is an association between these
symptoms and H pylori infection, then
treating and thus eradicating H pylori
must lead to improvement or disap-
pearance of symptoms. Randomized,
placebo-controlled, double-blind trials
with minimal loss to follow-up and
standardized and validated outcome
measures are needed. To our knowl-
edge, no such trial has been published.
CONCLUSIONS
There is noassociationbetweenRAPand
H pylori infection in children; therefore,
screening children with this classical
symptom is not warranted, regardless
of setting and geographic location. Fur-
thermore, all other GI symptoms in-
vestigated in primary carebased or
population-based studies, except for epi-
gastric pain, were not associated with H
e662 SPEE et al
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
pylori infection in children; therefore, we
postulate that as long as no typical clini-
cal picture of a child with H pylori infec-
tion has been established and treatment
effectiveness is not known, referral to a
subspecialist for this matter is not
recommended.
Furthermore we postulate that UAP
in a hospital-based setting and epi-
gastric pain in general might be as-
sociated with an (acute) H pylori in-
fection. Data reporting on epigastric
pain, however, were limited, so addi-
tional research to investigate this as-
sociation is needed.
APPENDIX 1: SEARCH STRATEGIES
Medline search, 27th of July 2009 608 results
(epidemiologic-studies OR case-control OR cohort OR follow-up OR longitudinal OR prospective OR retrospective OR cross-
sectional) AND (helicobacter pylori OR campylobacter) AND (Signs and Symptoms, Digestive[mesh] OR abdominal pain OR
dyspepsia) AND (infant OR infant* OR child OR child* OR adolescent OR adolescen*)
Embase search, 27th of July 2009 512 results
((epidemiologic studies/exp OR epidemiologic studies) OR cross-sectional study OR case control study OR cohort analysis
OR (follow up/exp OR follow up) OR longitudinal OR prospective OR retrospective) AND ((helicobacter pylori/exp OR heli-
cobacter pylori) OR (campylobacter/exp OR campylobacter)) AND ((gastrointestinal symptom/exp OR signs and symp-
toms, digestive) OR (abdominal pain/exp OR abdominal pain) OR (dyspepsia/exp OR dyspepsia)) AND ((infant/exp OR
infant) OR infant* OR (child/exp OR child) OR child* OR (adolescent/exp OR adolescent) OR adolescen*)
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e663
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
APPENDIX 2: EXPLANATION OF CRITERIA
MB / YvL / LS / MM
General
Case control study / Cross-sectional study
Criteria Score
1.
2.
3.
4.
5.
6.
7.
*
8.
9.
10.
Total Score (10 points maximum)
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
*
e664 SPEE et al
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
Explanation of criteria: Case control study/Cross-sectional study
Study population
1.
2.
3.
Helicobacter pylori
4.
5.
6.
Study design
7.
Analysis and data presentation
8.
9.
10.
OR
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e665
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
MB / YvL / LS / MM
General
Prospective cohort study
Criteria Score
1.
2.
3.
4.
5.
6.
7. *
8.
9.
10.
11.
Total Score (11 points maximum)
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
+ / - / ?
.
*
e666 SPEE et al
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
Explanation of criteria: Prospective cohort study
Study population
1.
2.
3.
Helicobacter pylori
4.
5.
Gastrointestinal symptoms
6.
Study design
7.
8.
Analysis and data presentation
9.
10.
11
OR
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e667
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
REFERENCES
1. Logan RP, Walker MM. ABC of the upper gas-
trointestinal tract: epidemiology and diag-
nosis of Helicobacter pylori infection. BMJ.
2001;323(7318):920922
2. Malaty HM, El-Kasabany A, Graham DY, et al.
Age at acquisition of Helicobacter pylori
infection: a follow-up study from infancy to
adulthood. Lancet. 2002;359(9310):931935
3. Moss SF, Malfertheiner P. Helicobacter and
gastric malignancies. Helicobacter. 2007;
12(suppl 1):2330
4. Drumm B, Koletzko S, Oderda G. Helicobac-
ter pylori infection in children: a consensus
statement. European Paediatric Task Force
on Helicobacter pylori. J Pediatr Gastroen-
terol Nutr. 2000;30(2):207213
5. Gold BD, Colletti RB, Abbott M, et al. Helico-
bacter pylori infection in children: recom-
mendations for diagnosis and treatment.
J Pediatr Gastroenterol Nutr. 2000;31(5):
490497
6. Malfertheiner P, Megraud F, OMorain C, et
al. Current concepts in the management of
Helicobacter pylori infection: the Maas-
tricht III Consensus Report. Gut. 2007;56(6):
772781
7. Koletzko S. Noninvasive diagnostic tests for
Helicobacter pylori infection in children.
Can J Gastroenterol. 2005;19(7):433439
8. Macarthur C, Saunders N, Feldman W. Heli-
cobacter pylori, gastroduodenal disease,
and recurrent abdominal pain in children.
JAMA. 1995;273(9):729734
9. Macarthur C. Helicobacter pylori infection
and childhood recurrent abdominal pain:
lack of evidence for a cause and effect rela-
tionship. Can J Gastroenterol. 1999;13(7):
607610
10. Altman DG. Systematic reviews of evalua-
tions of prognostic variables. BMJ. 2001;
323(7306):224228
11. Landis JR, Koch GG. An application of hierar-
chical kappa-type statistics in the assess-
ment of majority agreement among multi-
ple observers. Biometrics. 1977;33(2):
363374
12. Lievense AM, Bierma-Zeinstra SM, Verhagen
AP, Verhaar JA, Koes BW. Prognostic factors
of progress of hip osteoarthritis: a system-
atic review. Arthritis Rheum. 2002;47(5):
556562
13. Hayden JA, Cote P, Bombardier C. Evaluation
of the quality of prognosis studies in sys-
tematic reviews. Ann Intern Med. 2006;
144(6):427437
14. von Elm E, Altman DG, Egger M, et al. The
Strengthening the Reporting of Observa-
tional Studies in Epidemiology (STROBE)
statement: guidelines for reporting obser-
vational studies. Lancet. 2007;370(9596):
14531457
15. Apley J, Naish N. Recurrent abdominal
pains: a eld survey of 1,000 school chil-
dren. Arch Dis Child. 1958;33(168):165170
16. Daugule I, Rumba I, Alksnis J, Ejderhamn J.
Helicobacter pylori infection among chil-
dren with gastrointestinal symptoms: a
high prevalence of infection among patients
with reux oesophagitis. Acta Paediatr.
2007;96(7):10471049
17. Malaty HM, Abudayyeh S, Graham DY, Gilger
MA, Rabeneck L, OMalley K. A prospective
study for the association of Helicobacter py-
lori infection to a multidimensional mea-
sure for recurrent abdominal pain in chil-
dren. Helicobacter. 2006;11(4):250257
18. Yang YJ, Sheu BS, Lee SC, Wu JJ. Short-term
recurrent abdominal pain related to Helico-
bacter pylori infection in children. J Gastro-
enterol Hepatol. 2005;20(3):395400
19. Chong SK, Lou Q, Zollinger TW, et al. The se-
roprevalence of Helicobacter pylori in a re-
ferral population of children in the United
States. Am J Gastroenterol. 2003;98(10):
21622168
20. Ng BL, Quak SH, Aw M, Goh KT, Ho B. Immune
responses to differentiated forms of Helico-
bacter pylori in children with epigastric
pain. Clin Diagn Lab Immunol. 2003;10(5):
866869
21. Plebani M, Guariso G, Fogar P, et al. Effect of
cagA status on the sensitivity of enzyme im-
munoassay in diagnosing Helicobacter
pylori-infected children. Helicobacter. 1999;
4(4):226232
22. Macarthur C, Saunders N, Feldman W, et al.
Helicobacter pylori and childhood recur-
rent abdominal pain: community based
case-control study. BMJ. 1999;319(7213):
822823
23. Gu nel E, Findik D, Caglayan O, Caglayan F,
Topgac Z. Helicobacter pylori and hypergas-
trinemia in children with recurrent abdom-
inal pain. Pediatr Surg Int. 1998;14(12):
4042
24. Blu mel P, David M, Hirschl AM, Konig H. Inci-
dence of increased serum Helicobacter py-
lori IgG antibodies in children with and with-
out chronic abdominal pain [in German].
Klin Padiatr. 1998;210(5):366369
25. Bansal D, Patwari AK, Malhotra VL, Malhotra
V, Anand VK. Helicobacter pylori infection in
recurrent abdominal pain. Indian Pediatr.
1998;35(4):329335
26. Wewer V, Andersen LP, Paerregaard A, et al.
The prevalence and related symptomatol-
ogy of Helicobacter pylori in children with
recurrent abdominal pain. Acta Paediatr.
1998;87(8):830835
27. Kehrt R, Becker M, Brosicke H, Kruger N,
Helge H. Prevalence of Helicobacter pylori
infection in Nicaraguan children with per-
sistent diarrhea, diagnosed by the 13C-urea
breath test. J Pediatr Gastroenterol Nutr.
1997;25(1):8488
28. Oztu rk H, Senocak ME, Uzunalimoglu B, Has-
celik G, Buyukpamukcu N, Hicsonmez A. Hel-
icobacter pylori infection in symptomatic
and asymptomatic children: a prospective
clinical study. Eur J Pediatr Surg. 1996;6(5):
265269
29. Gu rakan F, Kocak N, Yuce A. Helicobacter
pylori serology in childhood. Turk J Pediatr.
1996;38(3):329334
30. Hardikar W, Feekery C, Smith A, Oberklaid F,
Grimwood K. Helicobacter pylori and recur-
rent abdominal pain in children. J Pediatr
Gastroenterol Nutr. 1996;22(2):148152
31. Chong SK, Lou Q, Asnicar MA, et al. Helico-
bacter pylori infection in recurrent abdom-
inal pain in childhood: comparison of diag-
nostic tests and therapy. Pediatrics. 1995;
96(2 pt 1):211215
32. Me ndez Nieto CM, Ramirez Mayans J, Cer-
vantes Bustamente R, et al. Helicobacter py-
lori diagnosis in children with recurrent
abdominal pain [in Spanish]. Acta Gastro-
enterol Latinoam. 1994;24(3):169174
33. van der Meer SB, Forget PP, Loffeld RJ, Stob-
beringh E, Kuijten RH, Arends JW. The prev-
alence of Helicobacter pylori serum
antibodies in children with recurrent ab-
dominal pain. Eur J Pediatr. 1992;151(11):
799801
34. Mukherjee P, Chacko B, Singh T, Pawar G,
Kaur H. Prevalence of Helicobacter pylori in-
fection in children with recurrent abdomi-
nal pain. Trop Gastroenterol. 2005;26(2):
102104
35. Sedla ckova M, Malaty H, Volf V, et al. Helico-
bacter pylori infection in a group of symp-
tomatic and asymptomatic children and ad-
olescents in the Czech Republic [in Czech].
Cas Lek Cesk. 2003;142(2):102105
36. Ozen A, Ertem D, Pehlivanoglu E. Natural his-
tory and symptomatology of Helicobacter
pylori in childhood and factors determining
the epidemiology of infection. J Pediatr Gas-
troenterol Nutr. 2006;42(4):398404
37. Tindberg Y, Nyren O, Blennow M, Granstrom
M. Helicobacter pylori infection and abdom-
inal symptoms among Swedish school chil-
dren. J Pediatr Gastroenterol Nutr. 2005;
41(1):3338
38. Lin HY, Chuang CK, Lee HC, Chiu NC, Lin SP,
Yeung CY. A seroepidemiologic study of Hel-
icobacter pylori and hepatitis A virus infec-
tion in primary school students in Taipei. J
e668 SPEE et al
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
Microbiol Immunol Infect. 2005;38(3):
176182
39. Bode G, Rothenbacher D, Brenner H, Adler
G. Helicobacter pylori and abdominal
symptoms: a population-based study
among preschool children in southern Ger-
many. Pediatrics. 1998;101(4 pt 1):634637
40. Rahman MM, Mahalanabis D, Sarker SA, et
al. Helicobacter pylori colonization in in-
fants and young children is not necessarily
associated with diarrhoea. J Trop Pediatr.
1998;44(5):283287
41. Grimm W, Fischbach W. Helicobacter pylori
infection in children and juveniles: an epide-
miological study on prevalence, socio-
economic factors and symptoms [in Ger-
man]. Dtsch Med Wochenschr. 2003;
128(37):18781883
42. McCallion WA, Bailie AG, Ardill JE, Bamford
KB, Potts SR, Boston VE. Helicobacter pylori,
hypergastrinaemia, and recurrent abdomi-
nal pain in children. J Pediatr Surg. 1995;
30(3):427429
43. Magista` AM, Ierardi E, Castellaneta S, et al.
Helicobacter pylori status and symptom as-
sessment two years after eradication in pe-
diatric patients from a high prevalence
area. J Pediatr Gastroenterol Nutr. 2005;
40(3):312318
44. ErtemD, Harmanci H, Pehlivanoglu E. Helico-
bacter pylori infection in Turkish preschool
and school children: role of socioeconomic
factors and breast feeding. Turk J Pediatr.
2003;45(2):114122
45. ODonohoe JM, Sullivan PB, Scott R, Rogers
T, Brueton MJ, Barltrop D. Recurrent ab-
dominal pain and Helicobacter pylori in a
community-based sample of London chil-
dren. Acta Paediatr. 1996;85(8):961964
46. Bode G, Brenner H, Adler G, Rothenbacher D.
Recurrent abdominal pain in children: evi-
dence from a population-based study that
social and familial factors play a major role
but not Helicobacter pylori infection. J Psy-
chosom Res. 2003;54(5):417421
47. Leandro Liberato SV, Hernandez Galindo M,
Torroba Alvarez L, et al. Helicobacter pylori
infection in the child population in Spain:
prevalence, related factors and inuence
on growth [in Spanish]. An Pediatr (Barc).
2005;63(6):489494
48. Tindberg Y, Blennow M, Granstrom M. Clini-
cal symptoms and social factors in a cohort
of children spontaneously clearing Helico-
bacter pylori infection. Acta Paediatr. 1999;
88(6):631635
49. Kasirga E, Ertan P, Tosun S, Sanhdag T, Tan-
sug N, Onag A. Children with recurrent ab-
dominal pain in Manisa Region, Western
Turkey: an evaluation of serological preva-
lence of Helicobacter pylori. Int J Med. 2003;
5(1):3235
50. Reshetnikov OV, Haiva VM, Granberg C,
Kurilovich SA, Babin VP. Seroprevalence of
Helicobacter pylori infection in Siberia. Hel-
icobacter. 2001;6(4):331336
51. Telmesani AM. Helicobacter pylori: preva-
lence and relationship with abdominal pain
in school children in Makkah City, western
Saudi Arabia. Saudi J Gastroenterol. 2009;
15(2):100103
52. Siai K, Ghozzi M, Ezzine H, et al. Prevalence
and risk factors of Helicobacter pylori infec-
tion in Tunesian children: 1055 children in
Cap-Bon (northeastern Tunisia). Gastroen-
terol Clin Biol. 2008;32(11):881886
53. Masoodpoor N, Darakhshan, Sheikhvatan
M. Helicobacter pylori infection in Iranian
children with recurrent abdominal pain.
Trop Gastroenterol. 2008;29(4):221223
54. Devanarayana NM, de Silva DG, de Silva HJ.
Aetiology of recurrent abdominal pain in a
cohort of Sri Lankan children. J Paediatr
Child Health. 2008;44(4):195200
55. Camorlinga-Ponce M, Torres J, Perez-Perez
G, et al. Validation of a serologic test for the
diagnosis of Helicobacter pylori infection
and the immune response to urease and
CagA in children. Am J Gastroenterol. 1998;
93(8):12641270
REVIEW ARTICLES
PEDIATRICS Volume 125, Number 3, March 2010 e669
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
DOI: 10.1542/peds.2010-0941
; originally published online February 15, 2010; 2010;125;e651 Pediatrics
Marjolein Y. Berger
Leo A. A. Spee, Marieke B. Madderom, Maaike Pijpers, Yvonne van Leeuwen and
Children
and Gastrointestinal Symptoms in Helicobacter pylori Association Between
Services
Updated Information &
tml
http://pediatrics.aappublications.org/content/125/3/e651.full.h
including high resolution figures, can be found at:
References
tml#ref-list-1
http://pediatrics.aappublications.org/content/125/3/e651.full.h
at:
This article cites 55 articles, 8 of which can be accessed free
Citations
tml#related-urls
http://pediatrics.aappublications.org/content/125/3/e651.full.h
This article has been cited by 7 HighWire-hosted articles:
Subspecialty Collections
ology_sub
http://pediatrics.aappublications.org/cgi/collection/gastroenter
Gastroenterology
the following collection(s):
This article, along with others on similar topics, appears in
Permissions & Licensing
ml
http://pediatrics.aappublications.org/site/misc/Permissions.xht
tables) or in its entirety can be found online at:
Information about reproducing this article in parts (figures,
Reprints
http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Grove Village, Illinois, 60007. Copyright 2010 by the American Academy of Pediatrics. All
and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk
publication, it has been published continuously since 1948. PEDIATRICS is owned, published,
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on March 19, 2014 pediatrics.aappublications.org Downloaded from
You might also like
- Is A Vegetarian Diet Safe To Follow DuringDocument41 pagesIs A Vegetarian Diet Safe To Follow DuringyuliaNo ratings yet
- 1 Helicobacter PyloriDocument7 pages1 Helicobacter PyloriNear MtzNo ratings yet
- 2020 ArticleDocument15 pages2020 ArticleIan ChanNo ratings yet
- Gastroesophageal Reflux and Asthma in Children: A Systematic ReviewDocument8 pagesGastroesophageal Reflux and Asthma in Children: A Systematic Reviewcasti21No ratings yet
- Diag BronchiolitisDocument2 pagesDiag BronchiolitisoussamamusNo ratings yet
- Pediatrics 2010 Thakkar E925 30Document8 pagesPediatrics 2010 Thakkar E925 30ivanhariachandraNo ratings yet
- 1 s2.0 S2095754816000041 MainDocument6 pages1 s2.0 S2095754816000041 MainKang TianNo ratings yet
- HyperemesisDocument4 pagesHyperemesisadindadian12No ratings yet
- NIH Public Access: Gastrointestinal Microbiome Signatures of Pediatric Patients With Irritable Bowel SyndromeDocument19 pagesNIH Public Access: Gastrointestinal Microbiome Signatures of Pediatric Patients With Irritable Bowel SyndromesebaspezoaNo ratings yet
- 2011 32 267 Robert M. Lawrence and Ruth A. Lawrence: Breastfeeding: More Than Just Good NutritionDocument16 pages2011 32 267 Robert M. Lawrence and Ruth A. Lawrence: Breastfeeding: More Than Just Good NutritionMax RodriguezNo ratings yet
- Clinical Prediction Rule For RSV Bronchiolitis in Healthy Newborns Prognostic Birth Cohort StudyDocument9 pagesClinical Prediction Rule For RSV Bronchiolitis in Healthy Newborns Prognostic Birth Cohort StudyJuwita PratiwiNo ratings yet
- A Meta-Evaluation of Nutrition Education Intervention Research Among Pregnant WomenDocument19 pagesA Meta-Evaluation of Nutrition Education Intervention Research Among Pregnant WomenZhewen TangNo ratings yet
- Akbari2013 PDFDocument8 pagesAkbari2013 PDFyakoub bensaadaNo ratings yet
- The Relationship Between Oral Hygiene Status and Obesity Among Preschool Children in Hong KongDocument5 pagesThe Relationship Between Oral Hygiene Status and Obesity Among Preschool Children in Hong KongIvan CarranzaNo ratings yet
- Prevalence and Risk Factors of Helicobacter Pylori Infection in Asymptomatic Chinese Children: A Prospective, Cross-Sectional, Population-Based StudyDocument8 pagesPrevalence and Risk Factors of Helicobacter Pylori Infection in Asymptomatic Chinese Children: A Prospective, Cross-Sectional, Population-Based StudyyundaNo ratings yet
- Epidemiology of Pediatric Functional Abdominal Pain Disorders: A Meta-AnalysisDocument24 pagesEpidemiology of Pediatric Functional Abdominal Pain Disorders: A Meta-AnalysisLiana Alviah SaputriNo ratings yet
- Pediatrics 2013 Feuille S7 8Document4 pagesPediatrics 2013 Feuille S7 8yuliantiumurahNo ratings yet
- Review: Helicobacter Pylori Infection in Paediatrics: J. Nguyen, K. Kotilea, V.Y. Miendje Deyi, P. BontemsDocument8 pagesReview: Helicobacter Pylori Infection in Paediatrics: J. Nguyen, K. Kotilea, V.Y. Miendje Deyi, P. Bontemsps piasNo ratings yet
- Skrining GiziDocument7 pagesSkrining GiziifaNo ratings yet
- Pediatrics-2011-Hauck-Peds 2010-3000Document10 pagesPediatrics-2011-Hauck-Peds 2010-3000api-285797257No ratings yet
- Comparison of Body Mass Index On Children With Functional Constipation and Healthy ControlsDocument5 pagesComparison of Body Mass Index On Children With Functional Constipation and Healthy ControlsGita TrisnawatiNo ratings yet
- ResearchintegrativereviewDocument17 pagesResearchintegrativereviewapi-315402591No ratings yet
- Nutritional Neuroscience and Education5Document14 pagesNutritional Neuroscience and Education5Ingrid DíazNo ratings yet
- Nonpharmacologic Treatments For Childhood Constipation: Systematic ReviewDocument9 pagesNonpharmacologic Treatments For Childhood Constipation: Systematic ReviewSardito PhanNo ratings yet
- Effect of A Probiotic Infant Formula On Infections in Child Care Centers Pediatrics-2005-Weizman-5-9Document7 pagesEffect of A Probiotic Infant Formula On Infections in Child Care Centers Pediatrics-2005-Weizman-5-9Yuktika RiYuNo ratings yet
- Downloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Document28 pagesDownloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Indah Putri permatasariNo ratings yet
- Clinical Pediatrics: Parental Perspectives of Early Childhood CariesDocument10 pagesClinical Pediatrics: Parental Perspectives of Early Childhood CariesBasant ShamsNo ratings yet
- 06 Original 02Document7 pages06 Original 02normanahmad92No ratings yet
- Practice: How Best To Diagnose Urinary Tract Infection in Preschool Children in Primary Care?Document4 pagesPractice: How Best To Diagnose Urinary Tract Infection in Preschool Children in Primary Care?naseeruddin04No ratings yet
- Zhou 2013fgDocument9 pagesZhou 2013fgMuhammad Wim AdhitamaNo ratings yet
- 10 1053@j Gastro 2020 01 024Document64 pages10 1053@j Gastro 2020 01 024Billis ParaschouNo ratings yet
- The Children's Eating Behavior InventoryDocument14 pagesThe Children's Eating Behavior Inventoryguilherme augusto paroNo ratings yet
- Reflex Anal Dilatation An Observational Study On Non-Abused ChildrenDocument5 pagesReflex Anal Dilatation An Observational Study On Non-Abused Childrenaniendyawijaya0% (1)
- Lung Ultrasound For The Diagnosis of Pneumonia in Children: A Meta-AnalysisDocument11 pagesLung Ultrasound For The Diagnosis of Pneumonia in Children: A Meta-AnalysisSilvia LaurentsNo ratings yet
- Effect of Breastfeeding On MorbidityDocument47 pagesEffect of Breastfeeding On MorbiditySarah QueenzzNo ratings yet
- Integrative Review BreastfeedingDocument19 pagesIntegrative Review Breastfeedingapi-430575435No ratings yet
- The Effect of Thickened-Feed Interventions On Gastroesophageal RefluxDocument13 pagesThe Effect of Thickened-Feed Interventions On Gastroesophageal Refluxminerva_stanciuNo ratings yet
- Oral Antibiotics For Neonatal Infections: A Systematic Review and Meta-AnalysisDocument12 pagesOral Antibiotics For Neonatal Infections: A Systematic Review and Meta-AnalysisAzaliRiccoNo ratings yet
- Measuring Quality of Life in The Parents of Children With AsthmaDocument8 pagesMeasuring Quality of Life in The Parents of Children With AsthmaTeodora VioletaNo ratings yet
- An Overview of Systematic Reviews of ComplementaryDocument16 pagesAn Overview of Systematic Reviews of ComplementaryDanilo VasconcelosNo ratings yet
- Infant Feeding Practices and Reported Food Allergies at 6 Years of AgeDocument10 pagesInfant Feeding Practices and Reported Food Allergies at 6 Years of AgeLia ApriliaNo ratings yet
- QoL Obese ChildrenDocument7 pagesQoL Obese ChildrenLiga Sabatina de BaloncestoNo ratings yet
- Lactobacillus Therapy For Acute Infectious Diarrhea in Children A Meta-AnalysisDocument9 pagesLactobacillus Therapy For Acute Infectious Diarrhea in Children A Meta-AnalysisfahrunisaNo ratings yet
- GastritisDocument9 pagesGastritisaby adyNo ratings yet
- Meta-Analysis: Proton Pump Inhibitors Moderately Increase The Risk of Small Intestinal Bacterial OvergrowthDocument10 pagesMeta-Analysis: Proton Pump Inhibitors Moderately Increase The Risk of Small Intestinal Bacterial OvergrowthOeoep Qurtubi AliNo ratings yet
- Boyd - UHP - GSM - Thesis - June 2020 SIGNED PDFDocument27 pagesBoyd - UHP - GSM - Thesis - June 2020 SIGNED PDFSavannah BoydNo ratings yet
- Pneumonia Comparative Effectiveness of Empiric Antibiotics For Community-AcquiredDocument9 pagesPneumonia Comparative Effectiveness of Empiric Antibiotics For Community-AcquiredSulis Na EndutzNo ratings yet
- Vitamin A and Carotenoids During Pregnancy and MaternalDocument20 pagesVitamin A and Carotenoids During Pregnancy and MaternalLalu SahdanNo ratings yet
- BurrowsDocument10 pagesBurrowsBenja NGNo ratings yet
- Jurnal LaktasiDocument7 pagesJurnal Laktasimuhammad firashNo ratings yet
- The Relationship Between Otitis Media With Effusion and Gastroesophageal Reflux Disease: A Meta-AnalysisDocument9 pagesThe Relationship Between Otitis Media With Effusion and Gastroesophageal Reflux Disease: A Meta-Analysisputri balqisNo ratings yet
- Anemia de PrematDocument7 pagesAnemia de Prematmedibase12No ratings yet
- Clinical-Epidemiological Considerations Regarding Primary Peptic Ulcer in Children - 5 Years Retrospective StudyDocument10 pagesClinical-Epidemiological Considerations Regarding Primary Peptic Ulcer in Children - 5 Years Retrospective StudySilvia PoamăneagrăNo ratings yet
- Williams Et Al-2019-Cochrane Database of Systematic ReviewsDocument4 pagesWilliams Et Al-2019-Cochrane Database of Systematic ReviewsErlinda AlfaNo ratings yet
- Assessment of Nutritional Status in Children and Adolescents With Post-Infectious Bronchiolitis ObliteransDocument8 pagesAssessment of Nutritional Status in Children and Adolescents With Post-Infectious Bronchiolitis ObliteranswwwigunaNo ratings yet
- Prevelance of Infection in Daibetic Children With H. Pylori Bacteria and Risk Factors of H. Pylori in Diabetic ChildrenDocument3 pagesPrevelance of Infection in Daibetic Children With H. Pylori Bacteria and Risk Factors of H. Pylori in Diabetic ChildrenBaru Chandrasekhar RaoNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Pediatric Food Allergy: A Clinical GuideFrom EverandPediatric Food Allergy: A Clinical GuideRuchi S. GuptaNo ratings yet
- Food Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementFrom EverandFood Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementTerri Faye Brown-WhitehornNo ratings yet
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsFrom EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsNo ratings yet
- 1471 230X 7 9 PDFDocument5 pages1471 230X 7 9 PDFivanhariachandraNo ratings yet
- En V52n2a11 PDFDocument11 pagesEn V52n2a11 PDFivanhariachandraNo ratings yet
- Pediatrics 2010 Thakkar E925 30Document8 pagesPediatrics 2010 Thakkar E925 30ivanhariachandraNo ratings yet
- Breastfeeding Issues Associated With HyperbilirubinemiaDocument11 pagesBreastfeeding Issues Associated With HyperbilirubinemiaivanhariachandraNo ratings yet