
Upper Gastrointestinal Bleeding: (UGIB)
Upper Gastrointestinal Bleeding: (UGIB)
You might also like
- Faussette On Wilson Darwin CathedralDocument13 pagesFaussette On Wilson Darwin CathedralDavid Enrique De La Dolorosa Chi BritoNo ratings yet
- NAG 1/W5A580 Auto Transmission Diagnosis and RepairDocument42 pagesNAG 1/W5A580 Auto Transmission Diagnosis and RepairKamerom CunninghamNo ratings yet
- Upper Gastrointestinal Bleeding 2007Document43 pagesUpper Gastrointestinal Bleeding 2007Matthew ThompsonNo ratings yet
- Upper GIB Lecture and Presentation.Document75 pagesUpper GIB Lecture and Presentation.Williams Emmanuel AdeyeyeNo ratings yet
- Gastrointestinal Bleeding: Dr. Székely Hajnal 2nd Department of Internal Medicine 2015/16-IDocument74 pagesGastrointestinal Bleeding: Dr. Székely Hajnal 2nd Department of Internal Medicine 2015/16-ISutisna NisaNo ratings yet
- MX of COVID-19Document49 pagesMX of COVID-19anisNo ratings yet
- DR Sarah Hearnshaw - Early Management of The Patient With Acute GI BleedingDocument38 pagesDR Sarah Hearnshaw - Early Management of The Patient With Acute GI BleedingRico NovyantoNo ratings yet
- Gastrointestinal Bleeding: Rajeev Jain, M.DDocument51 pagesGastrointestinal Bleeding: Rajeev Jain, M.DNovita AnjaniNo ratings yet
- Approach To GI BleedDocument97 pagesApproach To GI BleedPankaj IngleNo ratings yet
- SL No Content NODocument12 pagesSL No Content NOPdianghunNo ratings yet
- DX Approach & MX of HMDocument8 pagesDX Approach & MX of HMjosephNo ratings yet
- Git Bleeding - Upper & Lower.Document36 pagesGit Bleeding - Upper & Lower.Muwanga faizoNo ratings yet
- Hematemesis, Melena, HematoscheziaDocument48 pagesHematemesis, Melena, HematoscheziaSyarifah FauziahNo ratings yet
- Liver, Pancreas and Biliary Tract Problems: Case StudyDocument62 pagesLiver, Pancreas and Biliary Tract Problems: Case StudyElaine Frances IlloNo ratings yet
- Upper GI BleedingDocument30 pagesUpper GI BleedingBibek GhimireNo ratings yet
- 5-Upper Gastro-Intestinal BleedingDocument33 pages5-Upper Gastro-Intestinal BleedingAbdulrahman NanakaliNo ratings yet
- Hamed Alabad BPHDocument47 pagesHamed Alabad BPHHamed AlabadNo ratings yet
- Benign Prostatic Hyperplasia-Gabrilia Geaby RoringDocument19 pagesBenign Prostatic Hyperplasia-Gabrilia Geaby RoringDedylihawaNo ratings yet
- Acute Pancreatitis: Sarvodaya College of Nursing BangaloreDocument45 pagesAcute Pancreatitis: Sarvodaya College of Nursing BangaloreJeo ThomasNo ratings yet
- Syok Hipovolemik PerbaikanDocument24 pagesSyok Hipovolemik Perbaikanyoelpurnama1991No ratings yet
- Management of Bleeding Peptic Ulcer: Alankar GuptaDocument72 pagesManagement of Bleeding Peptic Ulcer: Alankar Guptadalesantiago08No ratings yet
- Esophageal VaricesDocument23 pagesEsophageal VariceskrisNo ratings yet
- Acute Pancreatitis NewDocument34 pagesAcute Pancreatitis NewDrscottmccallNo ratings yet
- Variceal Bleeding FFH Med-2Document24 pagesVariceal Bleeding FFH Med-2Niaz AhmadNo ratings yet
- Deep Vein ThrombosisDocument38 pagesDeep Vein ThrombosisvincentthedyNo ratings yet
- Management of A PT With SisDocument34 pagesManagement of A PT With SisZulkarnaen PintarNo ratings yet
- Update On Clinical Management - PrivateDocument57 pagesUpdate On Clinical Management - PrivateJashveerBediNo ratings yet
- Abdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccDocument38 pagesAbdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccAis KonorasNo ratings yet
- Acute Lower Gastrointestinal Bleeding: Evaluation and Management p206Document7 pagesAcute Lower Gastrointestinal Bleeding: Evaluation and Management p206Ahmed AlhalwajiNo ratings yet
- HarrisonsDocument117 pagesHarrisonsEm TimbolNo ratings yet
- Acute PancreatitisDocument76 pagesAcute PancreatitisKamran Khan Khalil100% (1)
- Stomach and Duodenum (Forsharing)Document79 pagesStomach and Duodenum (Forsharing)adversal8avrikNo ratings yet
- Upper and Lower GIT Bleeding DR Moses KazeevuDocument20 pagesUpper and Lower GIT Bleeding DR Moses KazeevuMoses Jr KazevuNo ratings yet
- Management of Upper Gi Bleeding: Nikhar Singhal 13046Document36 pagesManagement of Upper Gi Bleeding: Nikhar Singhal 13046Nikhar SinghalNo ratings yet
- AMI PrintDocument4 pagesAMI PrintKim SquaredNo ratings yet
- Gastroenterology 0321Document12 pagesGastroenterology 0321laraib fatima0% (1)
- Acute PancreatitisDocument32 pagesAcute Pancreatitismarkgodwin22No ratings yet
- Acute Pancreatitis: Hassan Mohammad Alshehri 2051040006Document41 pagesAcute Pancreatitis: Hassan Mohammad Alshehri 2051040006Hassan.shehri100% (1)
- Acute and Chronic Gastrointestinal BleedingDocument7 pagesAcute and Chronic Gastrointestinal BleedingMarwan M.100% (1)
- Update On The Management of PancreatitisDocument92 pagesUpdate On The Management of Pancreatitisadamu mohammadNo ratings yet
- Clinical Clerk Seminar Series: Approach To Gi BleedsDocument11 pagesClinical Clerk Seminar Series: Approach To Gi BleedsAngel_Liboon_388No ratings yet
- Perforated Peptic Ulcer - Habib DanielluthDocument15 pagesPerforated Peptic Ulcer - Habib DanielluthDa JunNo ratings yet
- Et. 2.perdarhan Saluran CernaDocument69 pagesEt. 2.perdarhan Saluran CernaMarpaung LizaNo ratings yet
- 12-Liver Cirrhosis 2012Document73 pages12-Liver Cirrhosis 2012nadiaNo ratings yet
- Inpatient Management of Patients With Liver CirrhosisDocument52 pagesInpatient Management of Patients With Liver CirrhosisSophia DevtaNo ratings yet
- Management of Upper Gi Bleeding: Nikhar Singhal 13046Document36 pagesManagement of Upper Gi Bleeding: Nikhar Singhal 13046Nikhar SinghalNo ratings yet
- Acute Pancreatitis: Sudden Severe Abdominal Pain Systemic UpsetDocument40 pagesAcute Pancreatitis: Sudden Severe Abdominal Pain Systemic UpsetcoolcaesarNo ratings yet
- Astra End HipDocument47 pagesAstra End HipIlze KonrādeNo ratings yet
- Cholycystectomy FinalDocument53 pagesCholycystectomy FinalCharmie GandaNo ratings yet
- CPD Januari 2013Document36 pagesCPD Januari 2013ledyNo ratings yet
- UGIBDocument24 pagesUGIBayoub hasandNo ratings yet
- GIT BleedingDocument49 pagesGIT BleedingKISHAN NAIDUNo ratings yet
- Management of Upper Gastrointestinal BleedingDocument62 pagesManagement of Upper Gastrointestinal BleedingAgustinus FatollaNo ratings yet
- Haematemesis and MalenaDocument39 pagesHaematemesis and MalenaNikNo ratings yet
- PancreatitisDocument59 pagesPancreatitisAarif RanaNo ratings yet
- Suggested Algorithm For Patients With Acute Upper .: BleedingDocument4 pagesSuggested Algorithm For Patients With Acute Upper .: BleedingMimi Marjorie TecNo ratings yet
- Dynamic Practice Guidelines For Emergency General SurgeryDocument19 pagesDynamic Practice Guidelines For Emergency General SurgeryJolaine ValloNo ratings yet
- Pancreatitis AcuteDocument42 pagesPancreatitis AcutearistadevyaNo ratings yet
- Js - Case PresentationDocument61 pagesJs - Case Presentationapi-592676308No ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Respiration 3Document23 pagesRespiration 3api-19916399100% (1)
- Blood CoagulationDocument70 pagesBlood Coagulationapi-19916399No ratings yet
- Respiration TwoDocument58 pagesRespiration Twoapi-19916399No ratings yet
- Preload and AfterloadDocument28 pagesPreload and Afterloadapi-19916399100% (1)
- Nervous System 7Document20 pagesNervous System 7api-19916399No ratings yet
- Physiology - Retired QuestionsDocument12 pagesPhysiology - Retired Questionsapi-19916399No ratings yet
- Physiology Answers and ExDocument19 pagesPhysiology Answers and Exapi-19916399No ratings yet
- Jingying T.A. Department of PhysiologyDocument26 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- Physiology of Blood VesselDocument65 pagesPhysiology of Blood Vesselapi-19916399No ratings yet
- Nervous System 6Document27 pagesNervous System 6api-19916399No ratings yet
- Jingying T.A. Department of PhysiologyDocument19 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- Jingying T.A. Department of PhysiologyDocument22 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- Gastrointestinal PhysiologDocument133 pagesGastrointestinal Physiologapi-19916399100% (1)
- Neurophysiology: Run Fight Speak Think Watch Listen Taste SmellDocument22 pagesNeurophysiology: Run Fight Speak Think Watch Listen Taste Smellapi-19916399No ratings yet
- 01.introduction To PhysiologyDocument44 pages01.introduction To Physiologyapi-19916399No ratings yet
- Evaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac IndexDocument53 pagesEvaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac Indexapi-19916399No ratings yet
- Circulation4 5Document1 pageCirculation4 5api-19916399No ratings yet
- Physiology of Blood VesselDocument65 pagesPhysiology of Blood Vesselapi-19916399No ratings yet
- Gastrointestinal PhysiologyDocument134 pagesGastrointestinal Physiologyapi-19916399100% (1)
- Electrophysiological Properties of Cardiac MyocytesDocument39 pagesElectrophysiological Properties of Cardiac Myocytesapi-19916399No ratings yet
- Electrical Activity of The HeartDocument29 pagesElectrical Activity of The Heartapi-19916399No ratings yet
- Kyuhyun Wang, MD: What Is The Rhythm?Document43 pagesKyuhyun Wang, MD: What Is The Rhythm?api-19916399No ratings yet
- Rhythmical Excitation of The HeartDocument29 pagesRhythmical Excitation of The Heartapi-19916399No ratings yet
- Evaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac IndexDocument53 pagesEvaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac Indexapi-19916399No ratings yet
- Chapter 2 - 1 - ForeignerDocument35 pagesChapter 2 - 1 - Foreignerapi-19916399No ratings yet
- Skate 3Document2 pagesSkate 3Muhammad FaridNo ratings yet
- Operations and Supply Chain Strategy: ReservedDocument15 pagesOperations and Supply Chain Strategy: ReservedkevrysantosaNo ratings yet
- Introduccion Al SRM ATR72Document60 pagesIntroduccion Al SRM ATR72Daniel Hernandez100% (1)
- Amsafe Seatbelt Airbag: First-Responder Reference GuideDocument10 pagesAmsafe Seatbelt Airbag: First-Responder Reference GuideAngel MogrovejoNo ratings yet
- EM4SS21 - Book of AbstractsDocument110 pagesEM4SS21 - Book of AbstractsGenNo ratings yet
- Bridge Inspection: + Numericl Rating SystemDocument88 pagesBridge Inspection: + Numericl Rating SystemShivangi MishraNo ratings yet
- Il'tq FTWN: On Deworming Administr, Ation and Management Followng Deworming (Aefd)Document12 pagesIl'tq FTWN: On Deworming Administr, Ation and Management Followng Deworming (Aefd)Kristina Ruth Marie V. MoyaNo ratings yet
- PotentiometerDocument9 pagesPotentiometerManuel Aldrin PaularNo ratings yet
- Traditional Arts VS Contemporary Arts PDFDocument80 pagesTraditional Arts VS Contemporary Arts PDFTeresa Rivera PapaNo ratings yet
- Vectors - Past Paper Questions: Cambridge IGCSEDocument12 pagesVectors - Past Paper Questions: Cambridge IGCSElilly lordNo ratings yet
- SMD 357Document6 pagesSMD 357Marcoantonio AntonioNo ratings yet
- Presentation Urban DesignDocument17 pagesPresentation Urban DesignLGU GALIMUYODNo ratings yet
- Failure of DescentDocument39 pagesFailure of DescentfahlevyNo ratings yet
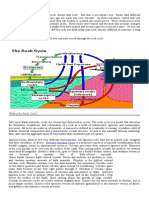
- The Rock CycleDocument3 pagesThe Rock CycleRODJHEN ANNE P. BARQUILLANo ratings yet
- CV FORMAT 2Document2 pagesCV FORMAT 2useforfreelanceworkNo ratings yet
- Hut, Hans. True BaptismDocument6 pagesHut, Hans. True BaptismCharles Cobalt ForsytheNo ratings yet
- Datasheet RACKOM 21U IP55 Outdoor CabinetDocument2 pagesDatasheet RACKOM 21U IP55 Outdoor CabinetPrem Singh MehtaNo ratings yet
- Getting Started Guide: Model Predictive Control Toolbox™Document174 pagesGetting Started Guide: Model Predictive Control Toolbox™porco gesuNo ratings yet
- Multiple Choice Questions: Sapkal Knowledge HubDocument11 pagesMultiple Choice Questions: Sapkal Knowledge HubMaqsood 9682619146No ratings yet
- User Manual: Retail ScalesDocument14 pagesUser Manual: Retail ScalesFernando Chacmana LinaresNo ratings yet
- 3 - Panel DataDocument35 pages3 - Panel DataDaniel PatraboyNo ratings yet
- TD 2106 4PG BW Oct2015Document4 pagesTD 2106 4PG BW Oct2015Patrick BrilhanteNo ratings yet
- Special Issue: An Exchange of Technical Information About Carrier Transicold Container ProductsDocument4 pagesSpecial Issue: An Exchange of Technical Information About Carrier Transicold Container ProductsCarlosAlbertoMirandaAndradesNo ratings yet
- Physics A: Unit: G484: The Newtonian WorldDocument9 pagesPhysics A: Unit: G484: The Newtonian Worldptscribd941No ratings yet
- Lms Template - Tutorial Chap 5Document4 pagesLms Template - Tutorial Chap 5LeticiaNo ratings yet
- Calvary Premadhara Jul-Aug2013Document36 pagesCalvary Premadhara Jul-Aug2013princejonnala100% (1)
- Ijfmpvol 12no 3jul-Sep2019Document116 pagesIjfmpvol 12no 3jul-Sep2019Grnitrv 22No ratings yet
- ThermodynamicasDocument21 pagesThermodynamicasTom Psy100% (1)















































































































Download as ppt, pdf, or txt
You might also like
- Faussette On Wilson Darwin CathedralDocument13 pagesFaussette On Wilson Darwin CathedralDavid Enrique De La Dolorosa Chi BritoNo ratings yet
- NAG 1/W5A580 Auto Transmission Diagnosis and RepairDocument42 pagesNAG 1/W5A580 Auto Transmission Diagnosis and RepairKamerom CunninghamNo ratings yet
- Upper Gastrointestinal Bleeding 2007Document43 pagesUpper Gastrointestinal Bleeding 2007Matthew ThompsonNo ratings yet
- Upper GIB Lecture and Presentation.Document75 pagesUpper GIB Lecture and Presentation.Williams Emmanuel AdeyeyeNo ratings yet
- Gastrointestinal Bleeding: Dr. Székely Hajnal 2nd Department of Internal Medicine 2015/16-IDocument74 pagesGastrointestinal Bleeding: Dr. Székely Hajnal 2nd Department of Internal Medicine 2015/16-ISutisna NisaNo ratings yet
- MX of COVID-19Document49 pagesMX of COVID-19anisNo ratings yet
- DR Sarah Hearnshaw - Early Management of The Patient With Acute GI BleedingDocument38 pagesDR Sarah Hearnshaw - Early Management of The Patient With Acute GI BleedingRico NovyantoNo ratings yet
- Gastrointestinal Bleeding: Rajeev Jain, M.DDocument51 pagesGastrointestinal Bleeding: Rajeev Jain, M.DNovita AnjaniNo ratings yet
- Approach To GI BleedDocument97 pagesApproach To GI BleedPankaj IngleNo ratings yet
- SL No Content NODocument12 pagesSL No Content NOPdianghunNo ratings yet
- DX Approach & MX of HMDocument8 pagesDX Approach & MX of HMjosephNo ratings yet
- Git Bleeding - Upper & Lower.Document36 pagesGit Bleeding - Upper & Lower.Muwanga faizoNo ratings yet
- Hematemesis, Melena, HematoscheziaDocument48 pagesHematemesis, Melena, HematoscheziaSyarifah FauziahNo ratings yet
- Liver, Pancreas and Biliary Tract Problems: Case StudyDocument62 pagesLiver, Pancreas and Biliary Tract Problems: Case StudyElaine Frances IlloNo ratings yet
- Upper GI BleedingDocument30 pagesUpper GI BleedingBibek GhimireNo ratings yet
- 5-Upper Gastro-Intestinal BleedingDocument33 pages5-Upper Gastro-Intestinal BleedingAbdulrahman NanakaliNo ratings yet
- Hamed Alabad BPHDocument47 pagesHamed Alabad BPHHamed AlabadNo ratings yet
- Benign Prostatic Hyperplasia-Gabrilia Geaby RoringDocument19 pagesBenign Prostatic Hyperplasia-Gabrilia Geaby RoringDedylihawaNo ratings yet
- Acute Pancreatitis: Sarvodaya College of Nursing BangaloreDocument45 pagesAcute Pancreatitis: Sarvodaya College of Nursing BangaloreJeo ThomasNo ratings yet
- Syok Hipovolemik PerbaikanDocument24 pagesSyok Hipovolemik Perbaikanyoelpurnama1991No ratings yet
- Management of Bleeding Peptic Ulcer: Alankar GuptaDocument72 pagesManagement of Bleeding Peptic Ulcer: Alankar Guptadalesantiago08No ratings yet
- Esophageal VaricesDocument23 pagesEsophageal VariceskrisNo ratings yet
- Acute Pancreatitis NewDocument34 pagesAcute Pancreatitis NewDrscottmccallNo ratings yet
- Variceal Bleeding FFH Med-2Document24 pagesVariceal Bleeding FFH Med-2Niaz AhmadNo ratings yet
- Deep Vein ThrombosisDocument38 pagesDeep Vein ThrombosisvincentthedyNo ratings yet
- Management of A PT With SisDocument34 pagesManagement of A PT With SisZulkarnaen PintarNo ratings yet
- Update On Clinical Management - PrivateDocument57 pagesUpdate On Clinical Management - PrivateJashveerBediNo ratings yet
- Abdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccDocument38 pagesAbdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccAis KonorasNo ratings yet
- Acute Lower Gastrointestinal Bleeding: Evaluation and Management p206Document7 pagesAcute Lower Gastrointestinal Bleeding: Evaluation and Management p206Ahmed AlhalwajiNo ratings yet
- HarrisonsDocument117 pagesHarrisonsEm TimbolNo ratings yet
- Acute PancreatitisDocument76 pagesAcute PancreatitisKamran Khan Khalil100% (1)
- Stomach and Duodenum (Forsharing)Document79 pagesStomach and Duodenum (Forsharing)adversal8avrikNo ratings yet
- Upper and Lower GIT Bleeding DR Moses KazeevuDocument20 pagesUpper and Lower GIT Bleeding DR Moses KazeevuMoses Jr KazevuNo ratings yet
- Management of Upper Gi Bleeding: Nikhar Singhal 13046Document36 pagesManagement of Upper Gi Bleeding: Nikhar Singhal 13046Nikhar SinghalNo ratings yet
- AMI PrintDocument4 pagesAMI PrintKim SquaredNo ratings yet
- Gastroenterology 0321Document12 pagesGastroenterology 0321laraib fatima0% (1)
- Acute PancreatitisDocument32 pagesAcute Pancreatitismarkgodwin22No ratings yet
- Acute Pancreatitis: Hassan Mohammad Alshehri 2051040006Document41 pagesAcute Pancreatitis: Hassan Mohammad Alshehri 2051040006Hassan.shehri100% (1)
- Acute and Chronic Gastrointestinal BleedingDocument7 pagesAcute and Chronic Gastrointestinal BleedingMarwan M.100% (1)
- Update On The Management of PancreatitisDocument92 pagesUpdate On The Management of Pancreatitisadamu mohammadNo ratings yet
- Clinical Clerk Seminar Series: Approach To Gi BleedsDocument11 pagesClinical Clerk Seminar Series: Approach To Gi BleedsAngel_Liboon_388No ratings yet
- Perforated Peptic Ulcer - Habib DanielluthDocument15 pagesPerforated Peptic Ulcer - Habib DanielluthDa JunNo ratings yet
- Et. 2.perdarhan Saluran CernaDocument69 pagesEt. 2.perdarhan Saluran CernaMarpaung LizaNo ratings yet
- 12-Liver Cirrhosis 2012Document73 pages12-Liver Cirrhosis 2012nadiaNo ratings yet
- Inpatient Management of Patients With Liver CirrhosisDocument52 pagesInpatient Management of Patients With Liver CirrhosisSophia DevtaNo ratings yet
- Management of Upper Gi Bleeding: Nikhar Singhal 13046Document36 pagesManagement of Upper Gi Bleeding: Nikhar Singhal 13046Nikhar SinghalNo ratings yet
- Acute Pancreatitis: Sudden Severe Abdominal Pain Systemic UpsetDocument40 pagesAcute Pancreatitis: Sudden Severe Abdominal Pain Systemic UpsetcoolcaesarNo ratings yet
- Astra End HipDocument47 pagesAstra End HipIlze KonrādeNo ratings yet
- Cholycystectomy FinalDocument53 pagesCholycystectomy FinalCharmie GandaNo ratings yet
- CPD Januari 2013Document36 pagesCPD Januari 2013ledyNo ratings yet
- UGIBDocument24 pagesUGIBayoub hasandNo ratings yet
- GIT BleedingDocument49 pagesGIT BleedingKISHAN NAIDUNo ratings yet
- Management of Upper Gastrointestinal BleedingDocument62 pagesManagement of Upper Gastrointestinal BleedingAgustinus FatollaNo ratings yet
- Haematemesis and MalenaDocument39 pagesHaematemesis and MalenaNikNo ratings yet
- PancreatitisDocument59 pagesPancreatitisAarif RanaNo ratings yet
- Suggested Algorithm For Patients With Acute Upper .: BleedingDocument4 pagesSuggested Algorithm For Patients With Acute Upper .: BleedingMimi Marjorie TecNo ratings yet
- Dynamic Practice Guidelines For Emergency General SurgeryDocument19 pagesDynamic Practice Guidelines For Emergency General SurgeryJolaine ValloNo ratings yet
- Pancreatitis AcuteDocument42 pagesPancreatitis AcutearistadevyaNo ratings yet
- Js - Case PresentationDocument61 pagesJs - Case Presentationapi-592676308No ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Respiration 3Document23 pagesRespiration 3api-19916399100% (1)
- Blood CoagulationDocument70 pagesBlood Coagulationapi-19916399No ratings yet
- Respiration TwoDocument58 pagesRespiration Twoapi-19916399No ratings yet
- Preload and AfterloadDocument28 pagesPreload and Afterloadapi-19916399100% (1)
- Nervous System 7Document20 pagesNervous System 7api-19916399No ratings yet
- Physiology - Retired QuestionsDocument12 pagesPhysiology - Retired Questionsapi-19916399No ratings yet
- Physiology Answers and ExDocument19 pagesPhysiology Answers and Exapi-19916399No ratings yet
- Jingying T.A. Department of PhysiologyDocument26 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- Physiology of Blood VesselDocument65 pagesPhysiology of Blood Vesselapi-19916399No ratings yet
- Nervous System 6Document27 pagesNervous System 6api-19916399No ratings yet
- Jingying T.A. Department of PhysiologyDocument19 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- Jingying T.A. Department of PhysiologyDocument22 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- Gastrointestinal PhysiologDocument133 pagesGastrointestinal Physiologapi-19916399100% (1)
- Neurophysiology: Run Fight Speak Think Watch Listen Taste SmellDocument22 pagesNeurophysiology: Run Fight Speak Think Watch Listen Taste Smellapi-19916399No ratings yet
- 01.introduction To PhysiologyDocument44 pages01.introduction To Physiologyapi-19916399No ratings yet
- Evaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac IndexDocument53 pagesEvaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac Indexapi-19916399No ratings yet
- Circulation4 5Document1 pageCirculation4 5api-19916399No ratings yet
- Physiology of Blood VesselDocument65 pagesPhysiology of Blood Vesselapi-19916399No ratings yet
- Gastrointestinal PhysiologyDocument134 pagesGastrointestinal Physiologyapi-19916399100% (1)
- Electrophysiological Properties of Cardiac MyocytesDocument39 pagesElectrophysiological Properties of Cardiac Myocytesapi-19916399No ratings yet
- Electrical Activity of The HeartDocument29 pagesElectrical Activity of The Heartapi-19916399No ratings yet
- Kyuhyun Wang, MD: What Is The Rhythm?Document43 pagesKyuhyun Wang, MD: What Is The Rhythm?api-19916399No ratings yet
- Rhythmical Excitation of The HeartDocument29 pagesRhythmical Excitation of The Heartapi-19916399No ratings yet
- Evaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac IndexDocument53 pagesEvaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac Indexapi-19916399No ratings yet
- Chapter 2 - 1 - ForeignerDocument35 pagesChapter 2 - 1 - Foreignerapi-19916399No ratings yet
- Skate 3Document2 pagesSkate 3Muhammad FaridNo ratings yet
- Operations and Supply Chain Strategy: ReservedDocument15 pagesOperations and Supply Chain Strategy: ReservedkevrysantosaNo ratings yet
- Introduccion Al SRM ATR72Document60 pagesIntroduccion Al SRM ATR72Daniel Hernandez100% (1)
- Amsafe Seatbelt Airbag: First-Responder Reference GuideDocument10 pagesAmsafe Seatbelt Airbag: First-Responder Reference GuideAngel MogrovejoNo ratings yet
- EM4SS21 - Book of AbstractsDocument110 pagesEM4SS21 - Book of AbstractsGenNo ratings yet
- Bridge Inspection: + Numericl Rating SystemDocument88 pagesBridge Inspection: + Numericl Rating SystemShivangi MishraNo ratings yet
- Il'tq FTWN: On Deworming Administr, Ation and Management Followng Deworming (Aefd)Document12 pagesIl'tq FTWN: On Deworming Administr, Ation and Management Followng Deworming (Aefd)Kristina Ruth Marie V. MoyaNo ratings yet
- PotentiometerDocument9 pagesPotentiometerManuel Aldrin PaularNo ratings yet
- Traditional Arts VS Contemporary Arts PDFDocument80 pagesTraditional Arts VS Contemporary Arts PDFTeresa Rivera PapaNo ratings yet
- Vectors - Past Paper Questions: Cambridge IGCSEDocument12 pagesVectors - Past Paper Questions: Cambridge IGCSElilly lordNo ratings yet
- SMD 357Document6 pagesSMD 357Marcoantonio AntonioNo ratings yet
- Presentation Urban DesignDocument17 pagesPresentation Urban DesignLGU GALIMUYODNo ratings yet
- Failure of DescentDocument39 pagesFailure of DescentfahlevyNo ratings yet
- The Rock CycleDocument3 pagesThe Rock CycleRODJHEN ANNE P. BARQUILLANo ratings yet
- CV FORMAT 2Document2 pagesCV FORMAT 2useforfreelanceworkNo ratings yet
- Hut, Hans. True BaptismDocument6 pagesHut, Hans. True BaptismCharles Cobalt ForsytheNo ratings yet
- Datasheet RACKOM 21U IP55 Outdoor CabinetDocument2 pagesDatasheet RACKOM 21U IP55 Outdoor CabinetPrem Singh MehtaNo ratings yet
- Getting Started Guide: Model Predictive Control Toolbox™Document174 pagesGetting Started Guide: Model Predictive Control Toolbox™porco gesuNo ratings yet
- Multiple Choice Questions: Sapkal Knowledge HubDocument11 pagesMultiple Choice Questions: Sapkal Knowledge HubMaqsood 9682619146No ratings yet
- User Manual: Retail ScalesDocument14 pagesUser Manual: Retail ScalesFernando Chacmana LinaresNo ratings yet
- 3 - Panel DataDocument35 pages3 - Panel DataDaniel PatraboyNo ratings yet
- TD 2106 4PG BW Oct2015Document4 pagesTD 2106 4PG BW Oct2015Patrick BrilhanteNo ratings yet
- Special Issue: An Exchange of Technical Information About Carrier Transicold Container ProductsDocument4 pagesSpecial Issue: An Exchange of Technical Information About Carrier Transicold Container ProductsCarlosAlbertoMirandaAndradesNo ratings yet
- Physics A: Unit: G484: The Newtonian WorldDocument9 pagesPhysics A: Unit: G484: The Newtonian Worldptscribd941No ratings yet
- Lms Template - Tutorial Chap 5Document4 pagesLms Template - Tutorial Chap 5LeticiaNo ratings yet
- Calvary Premadhara Jul-Aug2013Document36 pagesCalvary Premadhara Jul-Aug2013princejonnala100% (1)
- Ijfmpvol 12no 3jul-Sep2019Document116 pagesIjfmpvol 12no 3jul-Sep2019Grnitrv 22No ratings yet
- ThermodynamicasDocument21 pagesThermodynamicasTom Psy100% (1)