Download as pdf or txt
You might also like
- The Saturn Time Cube SimulationDocument67 pagesThe Saturn Time Cube Simulationtriple7inc100% (3)
- MT 998Document2 pagesMT 998Santo Xing100% (1)
- Use Cases For Example ATM SystemDocument54 pagesUse Cases For Example ATM SystemGayatri SharmaNo ratings yet
- Pat 2 Medsurg1Document20 pagesPat 2 Medsurg1api-300849832No ratings yet
- CVADocument27 pagesCVAMafe Campo100% (3)
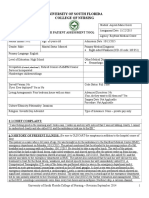
- University of South Florida College of Nursing: Fundamental Patient Assessment ToolDocument18 pagesUniversity of South Florida College of Nursing: Fundamental Patient Assessment Toolapi-315731045No ratings yet
- Nutrition Guide For Clinicians - STROKEDocument12 pagesNutrition Guide For Clinicians - STROKEPoiseBarbaraNo ratings yet
- Hemorrhagic Stroke Clinical PresentationDocument11 pagesHemorrhagic Stroke Clinical PresentationAndri wijayaNo ratings yet
- Case Analysis Presentation Group 1 Almost Done 2 1Document75 pagesCase Analysis Presentation Group 1 Almost Done 2 1Vhince Norben PiscoNo ratings yet
- Pat 2 Med Surg - Dean GradedDocument24 pagesPat 2 Med Surg - Dean Gradedapi-252790184No ratings yet
- Stroke 1. Disease/DisorderDocument11 pagesStroke 1. Disease/DisorderBiandaNo ratings yet
- Pat FinalDocument24 pagesPat Finalapi-252804976No ratings yet
- CNS Report-Stroke: Name: Koh Vic Ter Cohort: CH118 ID: 27542Document3 pagesCNS Report-Stroke: Name: Koh Vic Ter Cohort: CH118 ID: 27542ronwest1990No ratings yet
- Cerebrovascular DisordersDocument20 pagesCerebrovascular DisordersPrimas Shahibba RidhwanaNo ratings yet
- Pat Ms IIDocument18 pagesPat Ms IIapi-339980385No ratings yet
- Pat 2014Document20 pagesPat 2014api-324658071No ratings yet
- Ms 1 PatDocument19 pagesMs 1 Patapi-281676750No ratings yet
- Pat 2Document21 pagesPat 2api-270783686No ratings yet
- Heart Failure Thesis PDFDocument6 pagesHeart Failure Thesis PDFafknwride100% (2)
- Cerebrovascular AccidentDocument8 pagesCerebrovascular AccidentKarina CastilloNo ratings yet
- Patfall2015 Msii AnjouligerezDocument26 pagesPatfall2015 Msii Anjouligerezapi-325112936No ratings yet
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument20 pagesUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-300454618No ratings yet
- Hypertension: Pathophysiology and Diagnosis - CPD Article - Pharmaceutical JournalDocument8 pagesHypertension: Pathophysiology and Diagnosis - CPD Article - Pharmaceutical JournalOrion JohnNo ratings yet
- Pat 2 Sem 2Document25 pagesPat 2 Sem 2api-253093073No ratings yet
- Case Study QuestionsDocument35 pagesCase Study QuestionsazeemNo ratings yet
- Nur 111 Session 6 Sas 1Document12 pagesNur 111 Session 6 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Evaluation of Syncope in The Emergency Department: Differential DiagnosisDocument9 pagesEvaluation of Syncope in The Emergency Department: Differential DiagnosisaNo ratings yet
- Hemorrhagic Shock PDFDocument4 pagesHemorrhagic Shock PDFAdreiTheTripleANo ratings yet
- The Pathophysiology of Ischemic Strokes Is Widely Known. Ischemic Strokes Are TheDocument7 pagesThe Pathophysiology of Ischemic Strokes Is Widely Known. Ischemic Strokes Are Theprnczb13No ratings yet
- Coronary Artery Disease Cad2Document182 pagesCoronary Artery Disease Cad2Mamot Mot0% (1)
- Pat 3rd SemesterDocument19 pagesPat 3rd Semesterapi-324006383No ratings yet
- Case Study Cva Gr1Document72 pagesCase Study Cva Gr1Divina Gracia Fabicon Arana100% (1)
- Evaluation of SyncopeDocument11 pagesEvaluation of Syncopebluecrush1No ratings yet
- Critical Care Flash CardsDocument107 pagesCritical Care Flash CardsJoanna Ephraim CruzNo ratings yet
- 1228 HFStroke Altered Neuro 2011Document74 pages1228 HFStroke Altered Neuro 2011Cyndy EnterlineNo ratings yet
- Dent Clin N Am 50 (2006) 625-633Document9 pagesDent Clin N Am 50 (2006) 625-633lalajanNo ratings yet
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument22 pagesUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-300454618No ratings yet
- IJRPR15417Document2 pagesIJRPR15417Gleeware LimitedNo ratings yet
- Acute Ischemic Stroke UpdateDocument38 pagesAcute Ischemic Stroke Updatenarendra wahyuNo ratings yet
- Cardiac Arrest - Critical Care Medicine - MSD Manual Professional EditionDocument3 pagesCardiac Arrest - Critical Care Medicine - MSD Manual Professional EditionAnnisa Hilmy NurarifahNo ratings yet
- Acutely Decompensated Heart FailureDocument28 pagesAcutely Decompensated Heart FailureSabyasachi MukhopadhyayNo ratings yet
- Pat Fall 2014Document17 pagesPat Fall 2014api-300849832No ratings yet
- SMJ 60 616Document5 pagesSMJ 60 616kpbugisNo ratings yet
- Pat FundamentalsDocument16 pagesPat Fundamentalsapi-339980385No ratings yet
- 8 StrokeDocument8 pages8 StrokeAhmed aljumailiNo ratings yet
- Drug Treatment For Hypertensive Emergencies: New Concepts and Emerging Technologies For Emergency PhysiciansDocument0 pagesDrug Treatment For Hypertensive Emergencies: New Concepts and Emerging Technologies For Emergency PhysiciansRajihah JihahNo ratings yet
- Congestive Heart Failure in The ElderlyDocument13 pagesCongestive Heart Failure in The ElderlyKezia MarsilinaNo ratings yet
- S TrokeDocument12 pagesS Trokenersimelda dutyNo ratings yet
- Alegrias Pat-FundsDocument14 pagesAlegrias Pat-Fundsapi-324006383No ratings yet
- Choque en Urgencias 2018Document14 pagesChoque en Urgencias 2018Aura María Salazar SolarteNo ratings yet
- Stroke PreventionDocument7 pagesStroke Preventionellla 38No ratings yet
- Cerebrovasculara Ccident: Holy Angel University Angeles City College of NursingDocument124 pagesCerebrovasculara Ccident: Holy Angel University Angeles City College of Nursingninafatima allamNo ratings yet
- Prepared & Presented by MB, CHB (Grodno Medical University. Belarus), MSC Neurology (Grodno-Belarus)Document43 pagesPrepared & Presented by MB, CHB (Grodno Medical University. Belarus), MSC Neurology (Grodno-Belarus)Mahad abuukarNo ratings yet
- Congestive Heart FailureDocument16 pagesCongestive Heart FailureRahmat Burhanudin RamdaniNo ratings yet
- Pat 2 Med SurgDocument18 pagesPat 2 Med Surgapi-316861395No ratings yet
- Cardiovascular Complications of Antipsychotic MedicationsDocument3 pagesCardiovascular Complications of Antipsychotic MedicationsAakash ShahNo ratings yet
- ETiologia y Manejo POTSDocument15 pagesETiologia y Manejo POTSAlfredoNo ratings yet
- Patient Assessment Tool ms2Document27 pagesPatient Assessment Tool ms2api-280998981No ratings yet
- Jurnal NCBI Gagal JantungDocument16 pagesJurnal NCBI Gagal JantungMAS MANTRINo ratings yet
- 2020 Heart Failure, Older People and FrailtyDocument21 pages2020 Heart Failure, Older People and Frailtyalejandromfunes1749No ratings yet
- Cvja 24 28 PDFDocument6 pagesCvja 24 28 PDFvitriaNo ratings yet
- Recovering from Stroke - Overcoming the Challenges of StrokeFrom EverandRecovering from Stroke - Overcoming the Challenges of StrokeNo ratings yet
- When Lightning Strikes: An Illustrated Guide To Stroke Prevention And Re coveryFrom EverandWhen Lightning Strikes: An Illustrated Guide To Stroke Prevention And Re coveryNo ratings yet
- Generator Manual 1Document392 pagesGenerator Manual 1Gopal Radhakrishnan100% (5)
- Uji Statistik T TEST: Mean N Std. Deviation Std. Error Mean Pair 1 Pre 4,15 27 1,064, 205 Post 2,30 27, 775, 149Document3 pagesUji Statistik T TEST: Mean N Std. Deviation Std. Error Mean Pair 1 Pre 4,15 27 1,064, 205 Post 2,30 27, 775, 149GUSNAN AFRIZALNo ratings yet
- Lean AccountingDocument42 pagesLean AccountingAmamore Lorenzana PlazaNo ratings yet
- TDS 202 Dura ProofDocument2 pagesTDS 202 Dura ProofGhulam WaheedNo ratings yet
- 66 - Series Singer 66 Sewing Machine ManualDocument16 pages66 - Series Singer 66 Sewing Machine ManualCynthia PorterNo ratings yet
- Ahu 01 (STD)Document5 pagesAhu 01 (STD)onspsnonsNo ratings yet
- Sop-10 Dose Rate MeasurementDocument3 pagesSop-10 Dose Rate MeasurementOSAMANo ratings yet
- Inmarsat C System Definition Manula - Google SearchDocument2 pagesInmarsat C System Definition Manula - Google SearchasdfaNo ratings yet
- MSP 430 G 2553Document75 pagesMSP 430 G 2553diosb3No ratings yet
- Lesson Plan: Unit 1: My Funny Friend Lesson 7&8: Listening, Speaking and WritingDocument4 pagesLesson Plan: Unit 1: My Funny Friend Lesson 7&8: Listening, Speaking and WritingThúy Võ ThịNo ratings yet
- Business Environment Ch.3Document13 pagesBusiness Environment Ch.3hahahaha wahahahhaNo ratings yet
- Msds Promois W-32u 120808Document3 pagesMsds Promois W-32u 120808tia_utami23No ratings yet
- Metal Joining (Fasteners)Document11 pagesMetal Joining (Fasteners)ganeshNo ratings yet
- 2010 Nissan Versa S Fluid CapacitiesDocument2 pages2010 Nissan Versa S Fluid CapacitiesRubenNo ratings yet
- Moduflex Power Core (12kW) Rev01Document2 pagesModuflex Power Core (12kW) Rev01Steven SeNo ratings yet
- Bed 2nd Sem ResultDocument1 pageBed 2nd Sem ResultAnusree PranavamNo ratings yet
- Astm A 121 PDFDocument4 pagesAstm A 121 PDFDeepakNo ratings yet
- Clinical and Diagnostic Imaging Findings in Police Working Dogs Referred For Hip OsteoarthritisDocument11 pagesClinical and Diagnostic Imaging Findings in Police Working Dogs Referred For Hip OsteoarthritisEquilibrium EduardoNo ratings yet
- Flow of Fluids QuizDocument2 pagesFlow of Fluids QuizJhon Oliver De JoseNo ratings yet
- Cash Flow TemplateDocument9 pagesCash Flow Templatealdi ruNo ratings yet
- List - Parts of Bahay Na Bato - Filipiniana 101Document7 pagesList - Parts of Bahay Na Bato - Filipiniana 101Eriellynn Liza100% (1)
- Barry Thompson Book CHAPTER 8 Cantron - Extraordinary Antioxidant and Ingenious Cancer KillerDocument32 pagesBarry Thompson Book CHAPTER 8 Cantron - Extraordinary Antioxidant and Ingenious Cancer Killermonluck100% (2)
- © The Institute of Chartered Accountants of IndiaDocument154 pages© The Institute of Chartered Accountants of IndiaJattu TatiNo ratings yet
- Service JarnothingDocument28 pagesService Jarnothingpkumarynr1No ratings yet
- Rightline 176529 Parts ManualDocument8 pagesRightline 176529 Parts ManualSean CarvalhoNo ratings yet
- rr320305 Design of Machine Members IIDocument8 pagesrr320305 Design of Machine Members IISRINIVASA RAO GANTANo ratings yet
- Executing / Implementing Agency: Financial Management Assessment Questionnaire Topic ResponseDocument6 pagesExecuting / Implementing Agency: Financial Management Assessment Questionnaire Topic ResponseBelle CartagenaNo ratings yet