Download as doc, pdf, or txt
You might also like
- Concepts in Oral Medicine - Tractatio, Concipio, Documentatio Volume I, II, IIIDocument1 pageConcepts in Oral Medicine - Tractatio, Concipio, Documentatio Volume I, II, IIIGabriel Lazar100% (1)
- The Bicon Short ImplantDocument1 pageThe Bicon Short ImplantCarlosDiazNo ratings yet
- W. ProffitDocument118 pagesW. ProffitElena Oniga100% (1)
- Chapter 1 - Practical Notions Concerning Dental Occlusion: Personal InformationDocument61 pagesChapter 1 - Practical Notions Concerning Dental Occlusion: Personal InformationEmil Costruț100% (1)
- Ponts IndexDocument7 pagesPonts IndexTejinder SinghNo ratings yet
- Mandibular Overdenture PDFDocument103 pagesMandibular Overdenture PDFIbrahim Ahmed Dahab100% (1)
- Synthesis of A Diazo DyeDocument8 pagesSynthesis of A Diazo DyeLucas Man100% (1)
- Numerical Modelling of Stone Columns in Soft Clay Under An EmbankmentDocument7 pagesNumerical Modelling of Stone Columns in Soft Clay Under An EmbankmentebalicNo ratings yet
- CVM McnamaraDocument11 pagesCVM McnamaraXnb HajiNo ratings yet
- A Method of Cephalometric Evaluation Mcnamara 1984Document21 pagesA Method of Cephalometric Evaluation Mcnamara 1984Gaurav Pratap SinghNo ratings yet
- Biomechanical Relationship of The Cranial, Cervical, and Hyoid RegionsDocument7 pagesBiomechanical Relationship of The Cranial, Cervical, and Hyoid RegionsDenise MathreNo ratings yet
- Pi Is 0889540615010732Document17 pagesPi Is 0889540615010732Sri RengalakshmiNo ratings yet
- Moment To Force RatioDocument29 pagesMoment To Force RatioJp BaluyutNo ratings yet
- Cephalometrics Manual KrothDocument124 pagesCephalometrics Manual Krothimtiyazorthodontist100% (3)
- Skeletal Maturity IndicatorsDocument70 pagesSkeletal Maturity IndicatorsdrgreeshmahariniNo ratings yet
- Capitulo Jorge Ayala Libro Filosofia ROTHDocument44 pagesCapitulo Jorge Ayala Libro Filosofia ROTHAlan Ibarra MasterNo ratings yet
- Maintaining Clearly Defined Treatment Objectives:: Case StudyDocument5 pagesMaintaining Clearly Defined Treatment Objectives:: Case StudyAkylai IllanbekovaNo ratings yet
- TMJ Postgraduate ProgramDocument8 pagesTMJ Postgraduate ProgramsorcNo ratings yet
- Primary Role of Functional Matrices in Facial GrowthDocument12 pagesPrimary Role of Functional Matrices in Facial GrowthPranshu MathurNo ratings yet
- A Study of Parallelism of The Occlusal Plane and Ala Tragus LineDocument3 pagesA Study of Parallelism of The Occlusal Plane and Ala Tragus LineandrenicolasNo ratings yet
- The Bennett Angle: Clinical Comparison of Different Recording MethodsDocument6 pagesThe Bennett Angle: Clinical Comparison of Different Recording MethodsFrank Bermeo100% (1)
- Terapia MiofuncionalDocument10 pagesTerapia MiofuncionalvivianaNo ratings yet
- Andrews 6 Keys of Normal OcclusionDocument2 pagesAndrews 6 Keys of Normal OcclusionKaren AlfredNo ratings yet
- Impacts of Orthodontic Treatment On PeriDocument10 pagesImpacts of Orthodontic Treatment On PeriCatia Sofia A PNo ratings yet
- 08-The Heritability of Malocclusion-Part 2 The Influence of Genetics in Malocclusion PDFDocument9 pages08-The Heritability of Malocclusion-Part 2 The Influence of Genetics in Malocclusion PDFFadi Al Hajji100% (1)
- Elemento II AndrewsDocument8 pagesElemento II AndrewsdbarrioslambNo ratings yet
- Understanding The Basis of Space Closure in Orthodontics For A More Efficient Orthodontic TreatmentDocument12 pagesUnderstanding The Basis of Space Closure in Orthodontics For A More Efficient Orthodontic TreatmentGerardo QuinteroNo ratings yet
- Functional Examination: Textbook of OrthodonticsDocument3 pagesFunctional Examination: Textbook of OrthodonticsndranNo ratings yet
- Efecto Hyrax Vs HassDocument7 pagesEfecto Hyrax Vs HassJose Luis DominguezNo ratings yet
- The Herbst Appliance Research BasedDocument252 pagesThe Herbst Appliance Research BasedMu'taz ArmanNo ratings yet
- Anatomical Guidelines For Miniscrew InsertionDocument11 pagesAnatomical Guidelines For Miniscrew Insertionhector rincon100% (1)
- Acute Effects of Radiation InjuryDocument8 pagesAcute Effects of Radiation InjuryVikas VatsNo ratings yet
- Currie Et Al 2017 Angle Orthod PDFDocument14 pagesCurrie Et Al 2017 Angle Orthod PDFplayer osama100% (1)
- Wilmes. and Ludwig - Mini-Implants in The Anterior PalateDocument64 pagesWilmes. and Ludwig - Mini-Implants in The Anterior Palateromulodent100% (1)
- 2024 STAB J of Oral Rehabilitation - 2023 - Manfredini - Standardised Tool For The Assessment of BruxismDocument30 pages2024 STAB J of Oral Rehabilitation - 2023 - Manfredini - Standardised Tool For The Assessment of Bruxismteodude48100% (1)
- Topic - Maxillary Transverse DiscrepancyDocument42 pagesTopic - Maxillary Transverse Discrepancy王鈴鈞No ratings yet
- Broderick Occlusal Plane Analyzer (1DIEGO)Document5 pagesBroderick Occlusal Plane Analyzer (1DIEGO)diegoNo ratings yet
- Diagnosis & Treatment PlanningDocument46 pagesDiagnosis & Treatment PlanningNeha ChughNo ratings yet
- Positional Guidelines For Orthodontic Mini-Implant Placement in The Anterior Alveolar Region Systematic ReviewDocument10 pagesPositional Guidelines For Orthodontic Mini-Implant Placement in The Anterior Alveolar Region Systematic ReviewLarry MolinaNo ratings yet
- Holdaway SDocument64 pagesHoldaway SDryashpal Singh100% (1)
- Maxillary Transverse DeficiencyDocument4 pagesMaxillary Transverse DeficiencyCarlos Alberto CastañedaNo ratings yet
- Growth Studies of The Dentition. A Review. Moorrees, 1969Document17 pagesGrowth Studies of The Dentition. A Review. Moorrees, 1969Lorena ParraNo ratings yet
- Eur J Orthod-2007-Björk-i82-8Document7 pagesEur J Orthod-2007-Björk-i82-8Tammy MuñozNo ratings yet
- Class II Treatment Efficiency in U4 Extraction & Non Extraction Protocols 2007Document9 pagesClass II Treatment Efficiency in U4 Extraction & Non Extraction Protocols 2007Maha Ahmed SolimanNo ratings yet
- Chapter 1 Craniofacial Development - CompressedDocument30 pagesChapter 1 Craniofacial Development - CompressedAliya SyaikahNo ratings yet
- Growth and Development of FaceDocument12 pagesGrowth and Development of FaceARJUN SreenivasNo ratings yet
- CephalometricDocument42 pagesCephalometricAyad IbrahimNo ratings yet
- 2016 Issue 3Document82 pages2016 Issue 3Fareesha KhanNo ratings yet
- Björk 1955 CRANIAL BASE DEVELOPMENTDocument28 pagesBjörk 1955 CRANIAL BASE DEVELOPMENTPauly JinezNo ratings yet
- Asymmetric Deep Bite With A Canted Occlusal Plane - A Case ReportDocument9 pagesAsymmetric Deep Bite With A Canted Occlusal Plane - A Case ReportIacominiGustavoNo ratings yet
- OP & Dento Skeletal Frames During Growth by Dr. Eliana Midori TanakaDocument11 pagesOP & Dento Skeletal Frames During Growth by Dr. Eliana Midori TanakaMarisol 'VelaNo ratings yet
- 6 Review Article OnychophagiaDocument8 pages6 Review Article OnychophagiaAmalia HusnaNo ratings yet
- Roth Versus MBTDocument23 pagesRoth Versus MBTJose Antonio Figuroa AbadoNo ratings yet
- Surgically-Assisted Rapid Palatal Expansion For Management of Transverse Maxillary DeficiencyDocument3 pagesSurgically-Assisted Rapid Palatal Expansion For Management of Transverse Maxillary DeficiencyDaniela CastilloNo ratings yet
- Growth Patterns in Subjects With Long and Short FacesDocument12 pagesGrowth Patterns in Subjects With Long and Short FacesMatt SanoudosNo ratings yet
- Mosby's Orthodontic Review (2nd Edition) Pages 92 - 96Document5 pagesMosby's Orthodontic Review (2nd Edition) Pages 92 - 96sillyazianNo ratings yet
- Orthodontics 2: Research Activity Part 3 of 3Document22 pagesOrthodontics 2: Research Activity Part 3 of 3Gem Hanna Callano ParaguaNo ratings yet
- Subiecte Patologie Orala ExamenDocument5 pagesSubiecte Patologie Orala ExamengmacaneataNo ratings yet
- Aspecte Clinico Terapeutice Ale Despicăturilor Labio Maxilo Palatine Date Din LiteraturăDocument6 pagesAspecte Clinico Terapeutice Ale Despicăturilor Labio Maxilo Palatine Date Din LiteraturăDaniela Lelic100% (1)
- TransPalatalArch SIO1995 J.robettaloDocument11 pagesTransPalatalArch SIO1995 J.robettaloutkmangal100% (1)
- Interactions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionFrom EverandInteractions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionNo ratings yet
- Postlaryngectomy voice rehabilitation with voice prosthesesFrom EverandPostlaryngectomy voice rehabilitation with voice prosthesesNo ratings yet
- Prevention of Dry Socket PDFDocument4 pagesPrevention of Dry Socket PDFeddy1012805361No ratings yet
- OCO Biomedical 2013 Product Catalog 10-2013Document28 pagesOCO Biomedical 2013 Product Catalog 10-2013eddy1012805361No ratings yet
- EzlaseDocument7 pagesEzlaseeddy1012805361No ratings yet
- Long Term FearDocument12 pagesLong Term FearAdi PraTamaNo ratings yet
- Dental Anxiety ScaleDocument2 pagesDental Anxiety Scaleeddy1012805361100% (2)
- MY 2nd Sem. Presttn Biosensor & Enzymes As ImmunosensorsDocument32 pagesMY 2nd Sem. Presttn Biosensor & Enzymes As ImmunosensorsSamhita KalitaNo ratings yet
- MasterFlow - 400 v1 - 2Document2 pagesMasterFlow - 400 v1 - 2Vivek GaurNo ratings yet
- School of Chemical Engineering and Chemistry: Mapua Institute of TechnologyDocument2 pagesSchool of Chemical Engineering and Chemistry: Mapua Institute of TechnologyKayla DollenteNo ratings yet
- Determination of The Viscosity of Different Liquids Using A Falling Ball ViscometerDocument9 pagesDetermination of The Viscosity of Different Liquids Using A Falling Ball ViscometerJarell BalajadiaNo ratings yet
- 2005 Pearson Education South Asia Pte LTDDocument68 pages2005 Pearson Education South Asia Pte LTDDickson LeongNo ratings yet
- CT Selection - SIEMENSDocument1 pageCT Selection - SIEMENSveemandalNo ratings yet
- 1991 Alfred Maul - A Pioneer of Camera RocketDocument13 pages1991 Alfred Maul - A Pioneer of Camera RocketAlysson DiógenesNo ratings yet
- Plastic Analysis of Unbraced Portal Frames of Steel Structures in PDFDocument99 pagesPlastic Analysis of Unbraced Portal Frames of Steel Structures in PDFbiniamNo ratings yet
- Alis: An E Fficient Method To Compute High Spectral Resolution Polarized Solar Radiances Using The Monte Carlo ApproachDocument12 pagesAlis: An E Fficient Method To Compute High Spectral Resolution Polarized Solar Radiances Using The Monte Carlo ApproachShohihatun BariyahNo ratings yet
- Electrodynamics and RelativityDocument12 pagesElectrodynamics and RelativityWaqar Ahmed100% (1)
- User Manual OCTOPUS-OFFICE SHIP MOTION ANALYSIS SOFTWAREDocument69 pagesUser Manual OCTOPUS-OFFICE SHIP MOTION ANALYSIS SOFTWAREMiruna ClinciuNo ratings yet
- Cobalt Synthesis 0Document28 pagesCobalt Synthesis 0Rahul GogiaNo ratings yet
- Charles' Law Lab: BackgroundDocument3 pagesCharles' Law Lab: BackgroundKemani CampbellNo ratings yet
- Contributors: K LIMDocument6 pagesContributors: K LIMThiago Bruno CarneiroNo ratings yet
- Techteach - No Simview Temp Control IndexDocument4 pagesTechteach - No Simview Temp Control IndexDiabloNo ratings yet
- Waves Unit Catch A Wave!Document35 pagesWaves Unit Catch A Wave!aal_shurafaNo ratings yet
- Enve 208 Experiment-1Document3 pagesEnve 208 Experiment-1mihrican302No ratings yet
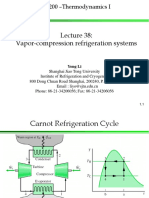
- Vapor-Compression Refrigeration SystemsDocument28 pagesVapor-Compression Refrigeration Systemsm_alodat6144No ratings yet
- Pathria Solution1Document4 pagesPathria Solution1Mario Mede RiteNo ratings yet
- Activated Sludge Flocculation: On-Line Determination of Floc Size and The Effect of ShearDocument9 pagesActivated Sludge Flocculation: On-Line Determination of Floc Size and The Effect of ShearCamila ContrerasNo ratings yet
- Jntua B.tech 2-1 Eee r15Document20 pagesJntua B.tech 2-1 Eee r15Vinodhkumar ReddyNo ratings yet
- Noether's TheoremDocument12 pagesNoether's TheoremFernando Vidal OlmosNo ratings yet
- MasterEmaco - S 348 v1Document2 pagesMasterEmaco - S 348 v1vahab_shaik0% (1)
- Friction Is The Force Resisting The Relative Motion of Solid SurfacesDocument2 pagesFriction Is The Force Resisting The Relative Motion of Solid SurfacesGunda LadkaNo ratings yet
- Calculos YogurtDocument2 pagesCalculos YogurtJohann RamirezNo ratings yet
- EuclidDocument12 pagesEuclidCaimar DoruanNo ratings yet
- Pogil Saturated and Unsaturated SolutionsDocument6 pagesPogil Saturated and Unsaturated Solutionsapi-213793181No ratings yet
- Experiment 2 & 3 FR Chem 28.1Document5 pagesExperiment 2 & 3 FR Chem 28.1Mara Krista CooNo ratings yet