Download as pptx, pdf, or txt
You might also like
- Nursing Care Plan Impaired Gas ExchangeDocument1 pageNursing Care Plan Impaired Gas ExchangeKarylle PetilNo ratings yet
- RLEFand ECSDocument3 pagesRLEFand ECSPaul JacksonNo ratings yet
- CFED 1023 CM in Our TimesDocument15 pagesCFED 1023 CM in Our TimesJayson CasiliNo ratings yet
- A Case Presentation of Diabetes Mellitus Type 2 Uncontrolled Non-Healing WoundDocument67 pagesA Case Presentation of Diabetes Mellitus Type 2 Uncontrolled Non-Healing Woundashamy acolNo ratings yet
- Case Study On Fluid OverloadDocument37 pagesCase Study On Fluid OverloadradicalmpNo ratings yet
- Emphysema BrochureDocument2 pagesEmphysema Brochureapi-242394302No ratings yet
- Tetralogy of Fallot TofDocument37 pagesTetralogy of Fallot TofWiza ErlandaNo ratings yet
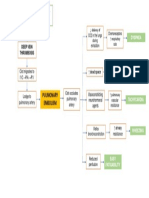
- Pulmonary Embolism PathophysiologyDocument1 pagePulmonary Embolism PathophysiologynikinoonaNo ratings yet
- Prof Ad Day 1Document136 pagesProf Ad Day 1Kareen ArnaizNo ratings yet
- Code Green Introduction Reviewer - RedDocument4 pagesCode Green Introduction Reviewer - RedJamieNo ratings yet
- GoutDocument12 pagesGoutEarle Jimenez Niervo RN100% (1)
- Pathophysiology of Tetralogy of FallotDocument2 pagesPathophysiology of Tetralogy of FallotWilliam GarnerNo ratings yet
- Topic 3 NCM 112Document4 pagesTopic 3 NCM 112Marielle ChuaNo ratings yet
- Gastritis FinalDocument6 pagesGastritis Finalapi-371817450% (2)
- Papillary Thyroid Ca: Group. 1 B Grand CaseDocument16 pagesPapillary Thyroid Ca: Group. 1 B Grand CaseAdora Dela CruzNo ratings yet
- Date and Time Focus Data Action Response 12/10/21Document2 pagesDate and Time Focus Data Action Response 12/10/21ANGEL AKIRA TORRESNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- Case Pres A1-RhdDocument11 pagesCase Pres A1-RhdCharm TanyaNo ratings yet
- CHFDocument35 pagesCHFNurayunie Abd HalimNo ratings yet
- Anatomy and Physiology PneumoniaDocument4 pagesAnatomy and Physiology PneumoniaJohnson MallibagoNo ratings yet
- Colon Cancer Introduction Case StudyDocument1 pageColon Cancer Introduction Case StudyHaru ZenkonsteinNo ratings yet
- PT EducationDocument4 pagesPT Educationapi-248017509No ratings yet
- Osteosarcoma-Ana and PhysiologyDocument4 pagesOsteosarcoma-Ana and PhysiologyNeirfla WassabiNo ratings yet
- Malnutrition in Older AdultsDocument44 pagesMalnutrition in Older Adultsjohnjoe subaynoNo ratings yet
- Liver CancerDocument28 pagesLiver CancerHealth Education Library for PeopleNo ratings yet
- Republic ActDocument36 pagesRepublic ActjanNo ratings yet
- HypopituitarismDocument2 pagesHypopituitarismAnne de VeraNo ratings yet
- Diverticular DiseaseDocument8 pagesDiverticular Diseasenurse_enzo100% (1)
- GlomerulonephritisDocument4 pagesGlomerulonephritisMary Cris BasayaNo ratings yet
- FluidDocument45 pagesFluidloglesb1No ratings yet
- Case Study PnuemoniaDocument10 pagesCase Study PnuemoniaKyle B. Nacionales Ü100% (1)
- Evidence-Based Nursing: I. Clinical QuestionDocument4 pagesEvidence-Based Nursing: I. Clinical QuestionRay Jorge MarmetoNo ratings yet
- Care PlanDocument4 pagesCare Planapi-217086261No ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) and Bronchial AsthmaDocument16 pagesChronic Obstructive Pulmonary Disease (COPD) and Bronchial AsthmaAngel Joy CatalanNo ratings yet
- NCP For PainDocument8 pagesNCP For PainClariz BascoNo ratings yet
- H MoleDocument2 pagesH MoleJoanna Marie Datahan EstomoNo ratings yet
- Case 052: Biliary ColicDocument4 pagesCase 052: Biliary ColicZauzaNo ratings yet
- NCPDocument10 pagesNCPCristina L. JaysonNo ratings yet
- Nutri WopsDocument4 pagesNutri WopsRizzy Ugay100% (1)
- Amoebiasis Case StudyDocument13 pagesAmoebiasis Case StudymelvinpasionaNo ratings yet
- Impaired Gas ExchangeDocument2 pagesImpaired Gas ExchangeLeah MillerNo ratings yet
- Pathophysiology of SeizuresDocument2 pagesPathophysiology of SeizuresireneNo ratings yet
- Case Study HyperkalemiaDocument10 pagesCase Study HyperkalemiaJamaica Cerrero100% (1)
- Propranolol, Prophylactic Warfarin, Low Molecular Weight Heparin (LMWH), Furosemide, AntibioticsDocument8 pagesPropranolol, Prophylactic Warfarin, Low Molecular Weight Heparin (LMWH), Furosemide, AntibioticsArlyn MarcelinoNo ratings yet
- Activity IntoleranceDocument6 pagesActivity IntoleranceRaidis PangilinanNo ratings yet
- Case 1-Clinical Case StudyDocument4 pagesCase 1-Clinical Case StudyRachel VillanuevaNo ratings yet
- Acute TonsillopharyngitisDocument17 pagesAcute TonsillopharyngitisRachel Haide NaravalNo ratings yet
- Dr. Sunatrio - Management Hypovolemic ShockDocument59 pagesDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeNo ratings yet
- NCP ModsDocument5 pagesNCP ModsKirstin del CarmenNo ratings yet
- Schematic Diagram of CKD Sec. To DM Nephropathy, DM Type 2, DM FootDocument8 pagesSchematic Diagram of CKD Sec. To DM Nephropathy, DM Type 2, DM Footbeuwolfagate50% (2)
- Final Major Case StudyDocument17 pagesFinal Major Case Studyapi-546876878No ratings yet
- Hypothyroidism PathophysiologyDocument1 pageHypothyroidism PathophysiologyCleo Joyce C. CristalNo ratings yet
- Concept Map - Colon CancerDocument2 pagesConcept Map - Colon Cancerbea pegadNo ratings yet
- Occurs Most Often In:: Muscular DystrophyDocument4 pagesOccurs Most Often In:: Muscular DystrophyJiezl Abellano AfinidadNo ratings yet
- Medical TestsDocument41 pagesMedical TestsJared Tristan LewisNo ratings yet
- Hypokalemia Disease AmnaDocument5 pagesHypokalemia Disease AmnaIzhar AhmadNo ratings yet
- Potassium Imbalance: by Ezekiel Seth Umangay Mark Oliver GonzalesDocument8 pagesPotassium Imbalance: by Ezekiel Seth Umangay Mark Oliver GonzalesEzekiel Seth UmangayNo ratings yet
- HypokalemiaDocument40 pagesHypokalemiaNadila Putri100% (1)
- Paralitik HipokalemiaDocument45 pagesParalitik HipokalemiaSinde NijucimiNo ratings yet
- HypermagnesimiaDocument2 pagesHypermagnesimiaShermayne Mallapre HernandezNo ratings yet
- Flail Chest (Tayug)Document25 pagesFlail Chest (Tayug)Adrian MallarNo ratings yet
- Community Health Nursing p.31-55Document25 pagesCommunity Health Nursing p.31-55Adrian MallarNo ratings yet
- Casestudy FractureDocument22 pagesCasestudy FractureAdrian Mallar0% (1)
- Psychiatric NursingDocument15 pagesPsychiatric NursingAdrian MallarNo ratings yet
- Legg Calve PerthesDocument7 pagesLegg Calve PerthesAdrian Mallar100% (1)
- Acquired Immune Deficiency Syndrome or Acquired Immunodeficiency Syndrome (AIDS) Is A Disease of The Human Immune System Caused byDocument7 pagesAcquired Immune Deficiency Syndrome or Acquired Immunodeficiency Syndrome (AIDS) Is A Disease of The Human Immune System Caused byAdrian MallarNo ratings yet
- Potts Disease Case AnalysisDocument5 pagesPotts Disease Case AnalysisAdrian MallarNo ratings yet
- NCP Deficient KnowledgeDocument1 pageNCP Deficient KnowledgeAdrian Mallar67% (3)
- HyperkalemiaDocument10 pagesHyperkalemiaAdrian MallarNo ratings yet
- Activity IntoleranceDocument1 pageActivity IntoleranceAdrian MallarNo ratings yet
- Fluid Volume Loss NCP - PediaDocument2 pagesFluid Volume Loss NCP - PediaAdrian MallarNo ratings yet
- College of Nursing: Homer D. Elegado BSN 3ADocument16 pagesCollege of Nursing: Homer D. Elegado BSN 3AAdrian MallarNo ratings yet
- Case in Herniorraphy BESTCASEDocument23 pagesCase in Herniorraphy BESTCASEAdrian MallarNo ratings yet
- Orthopedic Case StudyDocument8 pagesOrthopedic Case StudyAdrian Mallar100% (1)
- Case Study On SchizophreniaDocument21 pagesCase Study On SchizophreniaAdrian Mallar100% (2)
- Activity IntoleranceDocument1 pageActivity IntoleranceAdrian MallarNo ratings yet
- Potts Disease Case AnalysisDocument5 pagesPotts Disease Case AnalysisAdrian MallarNo ratings yet
- Fluid Volume Loss NCP - PediaDocument2 pagesFluid Volume Loss NCP - PediaAdrian MallarNo ratings yet
- College of Nursing: Homer D. Elegado BSN 3ADocument12 pagesCollege of Nursing: Homer D. Elegado BSN 3AAdrian MallarNo ratings yet
- Stab Wound Case StudyDocument33 pagesStab Wound Case StudyAdrian MallarNo ratings yet