Download as ppt, pdf, or txt
You might also like
- Copy1 TOPANAT EXAM MCQ Nee RevisedDocument125 pagesCopy1 TOPANAT EXAM MCQ Nee Revisedkapil pancholiNo ratings yet
- Upper Limb - Pectoral Region, Scapular Region, Axilla & Brachial PlexusDocument12 pagesUpper Limb - Pectoral Region, Scapular Region, Axilla & Brachial Plexusewijayapala100% (1)
- Anatomy 090819Document30 pagesAnatomy 090819Vaishnavi GourabathiniNo ratings yet
- Anatomy and PhysiologyDocument7 pagesAnatomy and PhysiologyKelly Camero ÜNo ratings yet
- Anatomy of The NeckDocument34 pagesAnatomy of The NeckAsma AlamoudiNo ratings yet
- Anatomy of Respiratory SystemDocument61 pagesAnatomy of Respiratory SystemLalu Fatria ZulhadiNo ratings yet
- Osteology Lower Limb, by DR IramDocument76 pagesOsteology Lower Limb, by DR IramimmmiNo ratings yet
- Gross Anatomy of Posterior Compartment of The ThighDocument20 pagesGross Anatomy of Posterior Compartment of The ThighOnah ArinzeNo ratings yet
- Cat Muscles and O.I.A.: Body Region Muscle Origin Insertion ActionDocument5 pagesCat Muscles and O.I.A.: Body Region Muscle Origin Insertion ActioneumarasiganNo ratings yet
- Esophagus: - Development ofDocument14 pagesEsophagus: - Development ofJonathan00711No ratings yet
- Functional Anatomy of Respiratory SystemDocument36 pagesFunctional Anatomy of Respiratory SystemshikhaNo ratings yet
- Upper Respiratory Tract AnatomyDocument61 pagesUpper Respiratory Tract Anatomyيحيى اسماعيل الجميليNo ratings yet
- Anatomy of The Nose and Paranasal SinusDocument5 pagesAnatomy of The Nose and Paranasal Sinusbayoe_pra100% (1)
- Lungs - Gross AnatomyDocument8 pagesLungs - Gross AnatomySuresh KumarNo ratings yet
- Upper Limb, Pectoral RegionDocument24 pagesUpper Limb, Pectoral Regiongtaha80No ratings yet
- MnemonicsDocument11 pagesMnemonicsanon-626602No ratings yet
- Arteries of Upper Limb.Document16 pagesArteries of Upper Limb.Shimmering Moon100% (1)
- Lungs PDFDocument47 pagesLungs PDFAmna YousafNo ratings yet
- Bone Joint Cartilage PowerpointDocument81 pagesBone Joint Cartilage PowerpointChevie WisemanNo ratings yet
- Characteristics of Histology SlidesDocument4 pagesCharacteristics of Histology SlidesLaiq Khan100% (1)
- Anatomy of The Larynx: General DescriptionDocument38 pagesAnatomy of The Larynx: General DescriptionDr-Firas Nayf Al-ThawabiaNo ratings yet
- Hypo Thyroid Is MDocument4 pagesHypo Thyroid Is MAradhanaRamchandaniNo ratings yet
- Anatomy of The EarDocument41 pagesAnatomy of The EarDenny Briant100% (1)
- Anterior & Medial Compartment of ThighDocument25 pagesAnterior & Medial Compartment of ThighnasibdinNo ratings yet
- Surgical Anatomy of Fascial SpacesDocument61 pagesSurgical Anatomy of Fascial SpacesDR NASIM100% (1)
- Anato Head and Neck MnemonicsDocument10 pagesAnato Head and Neck MnemonicsLaura Lopez RocaNo ratings yet
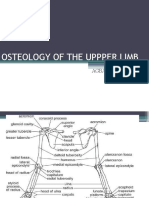
- Osteology of Upper LimbDocument63 pagesOsteology of Upper LimbAkomolede AbosedeNo ratings yet
- 3-Inguinal Canal PDFDocument58 pages3-Inguinal Canal PDFN A0% (1)
- ملزمه الانسجه الجهاز الهضمي الجزء الاولDocument42 pagesملزمه الانسجه الجهاز الهضمي الجزء الاولlaithjnbNo ratings yet
- Topographical Anatomy of The Lower Limb - Listed AlphabeticallyDocument3 pagesTopographical Anatomy of The Lower Limb - Listed AlphabeticallySaba Adde Duhera-HamidovicNo ratings yet
- PharynxDocument39 pagesPharynxapi-324160601100% (1)
- General AnatomyDocument37 pagesGeneral AnatomyTaufik AhmadNo ratings yet
- Histology of The Digestive SystemDocument46 pagesHistology of The Digestive SystemM Reza Rizqi INo ratings yet
- BDS1040 The Orbit and Its Contents (Lecture)Document49 pagesBDS1040 The Orbit and Its Contents (Lecture)Aya OsamaNo ratings yet
- Shoulder SlidesDocument84 pagesShoulder SlidesSean Joseph100% (1)
- Temporal and Infratemporal FossaeDocument29 pagesTemporal and Infratemporal FossaeRobin Tolentino100% (1)
- 07.lymphatic Sysytem 18Document24 pages07.lymphatic Sysytem 18driraja9999No ratings yet
- Histology Practical Manual Part 1 2021Document124 pagesHistology Practical Manual Part 1 2021khushikumari1407No ratings yet
- Erb's PointDocument14 pagesErb's PointRohit SharmaNo ratings yet
- 6.24 Muscles Head & Neck - Blok 6Document12 pages6.24 Muscles Head & Neck - Blok 6magenthaNo ratings yet
- Femoral Region, Anterior and Medial Compartments of The ThighDocument49 pagesFemoral Region, Anterior and Medial Compartments of The ThighNolanNo ratings yet
- Upper Limb 1Document14 pagesUpper Limb 1faraNo ratings yet
- Circumflex Scapular: Dorsum of Thoracodorsal: Latissmus DorsiDocument4 pagesCircumflex Scapular: Dorsum of Thoracodorsal: Latissmus Dorsispeedy.catNo ratings yet
- Tissues 4Document65 pagesTissues 4marianisie448100% (3)
- Development of The FaceDocument76 pagesDevelopment of The Facedr parveen bathla100% (1)
- 2 MCQ - Autonomic - 2Document33 pages2 MCQ - Autonomic - 275qkdkj9mdNo ratings yet
- NeckDocument94 pagesNeckSathvika BNo ratings yet
- 4.thoracic WallDocument20 pages4.thoracic WallAmrith LordNo ratings yet
- Peritoneal Anatomy Lecture NotesDocument4 pagesPeritoneal Anatomy Lecture Noteschc300No ratings yet
- Anatomy - Abdomen and PelvisDocument46 pagesAnatomy - Abdomen and PelvisDr.G.Bhanu PrakashNo ratings yet
- Heart SoundsDocument23 pagesHeart SoundsK.R.RaguramNo ratings yet
- Upper Limb 0809 PDFDocument59 pagesUpper Limb 0809 PDFasdaNo ratings yet
- Upper LimbDocument54 pagesUpper LimbMar YNo ratings yet
- A Respiratory System Histology 16-12-14Document33 pagesA Respiratory System Histology 16-12-14Suhas KapseNo ratings yet
- Lesser Omentum Project: Penny Fleming Kimberly BurnhamDocument32 pagesLesser Omentum Project: Penny Fleming Kimberly BurnhamspiraldaoNo ratings yet
- Nerve and Blood Supply of Lower ExtremitiesDocument22 pagesNerve and Blood Supply of Lower ExtremitiesBenjamin Prabhu100% (3)
- Anatomy and Physiology Terms: Brief Definitions, Roots & Morphology; An Abecedary; Vol 10 - Digestive System TermsFrom EverandAnatomy and Physiology Terms: Brief Definitions, Roots & Morphology; An Abecedary; Vol 10 - Digestive System TermsNo ratings yet
- Physiology of The Respiratory System-1Document155 pagesPhysiology of The Respiratory System-1Adil MusaddiqNo ratings yet
- PM2 - Anatomy II - The Respiratory SystemDocument35 pagesPM2 - Anatomy II - The Respiratory SystemNsikan GabrielNo ratings yet
- Passenger Health Declaration Form-V9 - tcm27-72912Document2 pagesPassenger Health Declaration Form-V9 - tcm27-72912Mimi ChienNo ratings yet
- Meptin® Swinghaler®: Dry Powder InhalerDocument9 pagesMeptin® Swinghaler®: Dry Powder InhalerYusuf HadiNo ratings yet
- Comparative Analysis Essay ExampleDocument5 pagesComparative Analysis Essay Examplefz75yesw100% (2)
- Heat Stress PlanDocument11 pagesHeat Stress Planzahid khanNo ratings yet
- National Mental Health ProgrammeDocument58 pagesNational Mental Health ProgrammeShilu Mathai PappachanNo ratings yet
- Human Values and Professional Ethics: Submitted To Dr. Khushbu Batra, Assistant Professor, Ash DeptDocument7 pagesHuman Values and Professional Ethics: Submitted To Dr. Khushbu Batra, Assistant Professor, Ash DeptAparna TyagiNo ratings yet
- January 2024 (Part-I)Document12 pagesJanuary 2024 (Part-I)Drishti KarmaNo ratings yet
- Presentation Electri in TrichologyDocument69 pagesPresentation Electri in TrichologycarmenNo ratings yet
- Contact Dermatitis: Dr. Hanna Jinky AbraganDocument11 pagesContact Dermatitis: Dr. Hanna Jinky AbraganAying De Barras AbraganNo ratings yet
- In Focus 15Document4 pagesIn Focus 15drrselvarajNo ratings yet
- Fnhum 16 950434Document8 pagesFnhum 16 950434syarifaNo ratings yet
- FB 230219174334Document73 pagesFB 230219174334tiyNo ratings yet
- FAQs - Population-Based Health Care PackagesDocument2 pagesFAQs - Population-Based Health Care PackagesPhilippe Ceasar C. BascoNo ratings yet
- Osh 6301Document4 pagesOsh 6301Hassan ShahzadNo ratings yet
- Inclusion and Equity PolicyDocument10 pagesInclusion and Equity Policyapi-281870616No ratings yet
- Ijomi 15 415Document4 pagesIjomi 15 415Bagis Emre GulNo ratings yet
- Central Nervous System Drug StudyDocument11 pagesCentral Nervous System Drug StudySanny L Asim Jr.No ratings yet
- Faktor Risiko Yang Mempengaruhi Terjadinya Stroke Non Hemoragik Pada Pasien Di RS RK Charitas Dan RS Myria PalembangDocument7 pagesFaktor Risiko Yang Mempengaruhi Terjadinya Stroke Non Hemoragik Pada Pasien Di RS RK Charitas Dan RS Myria PalembangmasyitahNo ratings yet
- AudiogramDocument38 pagesAudiogramaarya12No ratings yet
- Indian Women and Health Related IssuesDocument29 pagesIndian Women and Health Related Issuesuma_mandeNo ratings yet
- Grade 11biology: Science of YourselfDocument60 pagesGrade 11biology: Science of YourselfDanielNo ratings yet
- Nanda 2021 2023Document6 pagesNanda 2021 2023Khimberly UmbaoNo ratings yet
- Society: America's "Young" Weight ProblemDocument9 pagesSociety: America's "Young" Weight ProblemFabiano HenriqueNo ratings yet
- 500 Most Important English Questions For CDS Exam Part 2Document259 pages500 Most Important English Questions For CDS Exam Part 2Jatin BhagatNo ratings yet
- Pathophysiology of Myocardial Infarction and Acute Management StrategiesDocument11 pagesPathophysiology of Myocardial Infarction and Acute Management StrategiesnwabukingzNo ratings yet
- Assigment MicrobiologyDocument7 pagesAssigment MicrobiologyFu'e AbdumalikNo ratings yet
- Diabetes Mellitus Indian PerspectiveDocument8 pagesDiabetes Mellitus Indian PerspectiveEditor IJTSRDNo ratings yet
- FEP MendozaDocument5 pagesFEP MendozaSamantha ClaireNo ratings yet
- Parameters of Fluid Responsiveness Curr Op Crit Care Shi2020Document8 pagesParameters of Fluid Responsiveness Curr Op Crit Care Shi2020Tadeo PradoNo ratings yet
- Astrocyte: Structure & FunctionDocument7 pagesAstrocyte: Structure & Functionمحمود الموسويNo ratings yet