Download as pdf or txt
You might also like
- AOTA Exam PrepDocument2 pagesAOTA Exam PrepKenny ClayNo ratings yet
- Performance Standards For Antifungal Susceptibility Testing of YeastsDocument30 pagesPerformance Standards For Antifungal Susceptibility Testing of YeastsAnne Abejuela Obial100% (2)
- CE Article November 2017Document8 pagesCE Article November 2017Marcelo Jorge EuredjianNo ratings yet
- Dementia AOTA Helpful Fact SheetDocument2 pagesDementia AOTA Helpful Fact SheetMysti Reeder100% (1)
- Opening A Private Practice in Occupational Therapy: Earn .1 Aota CeuDocument9 pagesOpening A Private Practice in Occupational Therapy: Earn .1 Aota CeuRey John MonjeNo ratings yet
- ANALYSIS OF LONGITUNIDAL CEPHALOMETRIC GROWTH DATA. Bhatia B.C. Leighton (1993) (01-17)Document17 pagesANALYSIS OF LONGITUNIDAL CEPHALOMETRIC GROWTH DATA. Bhatia B.C. Leighton (1993) (01-17)Nicolas StaffelbachNo ratings yet
- About The NBCOT OTR and Cota Exams: Exam BasicsDocument2 pagesAbout The NBCOT OTR and Cota Exams: Exam BasicsJennifer gomezNo ratings yet
- Soap NoteDocument2 pagesSoap Noteapi-285542134No ratings yet
- Vergara, J. - T.O. in The Neonatal Intensive Care UnitDocument11 pagesVergara, J. - T.O. in The Neonatal Intensive Care UnitFedora Margarita Santander CeronNo ratings yet
- Gilfoyle 1984 Slagle LectureDocument14 pagesGilfoyle 1984 Slagle LectureDebbieNo ratings yet
- MOHOST InformationDocument1 pageMOHOST InformationRichard FullertonNo ratings yet
- Ashley M Occt 651 Occupational ProfileDocument11 pagesAshley M Occt 651 Occupational Profileapi-25080062950% (2)
- Model of Human Occupation Parts 1-4Document36 pagesModel of Human Occupation Parts 1-4Alice GiffordNo ratings yet
- Occupational Therapy and Mental Health 1Document18 pagesOccupational Therapy and Mental Health 1Roman -No ratings yet
- Client-Centered AssessmentDocument4 pagesClient-Centered AssessmentHon “Issac” KinHoNo ratings yet
- AprJul2017 PublicReportDocument130 pagesAprJul2017 PublicReportAgnes Claudia100% (1)
- Bethany Case StudyDocument25 pagesBethany Case StudyMegan McCarthyNo ratings yet
- ADocument7 pagesARaphael AguiarNo ratings yet
- Occt630 Occupational Profile InterventionDocument19 pagesOcct630 Occupational Profile Interventionapi-290880850No ratings yet
- 2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)Document54 pages2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)engshi18No ratings yet
- Role of OT in End of Life CareDocument13 pagesRole of OT in End of Life Carekori holubNo ratings yet
- Occupational Therapy: SCI, TBI, & CVADocument35 pagesOccupational Therapy: SCI, TBI, & CVAAnAs Al ArjanNo ratings yet
- Aus Occup Therapy J - 2002 - Wilcock - Reflections On Doing Being and BecomingDocument11 pagesAus Occup Therapy J - 2002 - Wilcock - Reflections On Doing Being and BecomingMelissa CroukampNo ratings yet
- Placement HandbookDocument551 pagesPlacement HandbookAdonis GaleosNo ratings yet
- Occupational JusticeDocument4 pagesOccupational JusticeHardeep Singh BaliNo ratings yet
- Occupational Therapy in Oncology and Palliative CareDocument10 pagesOccupational Therapy in Oncology and Palliative CareSenthil KumarNo ratings yet
- Integration of Medication Management Into Occupational Therapy PracticeDocument7 pagesIntegration of Medication Management Into Occupational Therapy PracticeManuel PérezNo ratings yet
- Position Paper OT For People With LDDocument10 pagesPosition Paper OT For People With LDLytiana WilliamsNo ratings yet
- Aota Code of EthicsDocument13 pagesAota Code of Ethicsapi-311121263No ratings yet
- Occupational Therapy Activities For AdultsDocument3 pagesOccupational Therapy Activities For AdultsEllee HadesNo ratings yet
- Psychomotor Therapy and Psychiatry Whats in A NamDocument9 pagesPsychomotor Therapy and Psychiatry Whats in A NamBrigitte MauriNo ratings yet
- Occupational Therapy Rehabilitation Paraplegic PatientDocument7 pagesOccupational Therapy Rehabilitation Paraplegic PatientAlina PasăreNo ratings yet
- Occupational Therapy Interventions To Improve PDFDocument9 pagesOccupational Therapy Interventions To Improve PDFPaula FariaNo ratings yet
- Occt 652a - ResumeDocument3 pagesOcct 652a - Resumeapi-279916752No ratings yet
- Stroke Rehab Fact SheetDocument2 pagesStroke Rehab Fact SheetHendra PrayogaNo ratings yet
- The Performance Quality Rating Scale (PQRS) : Reliability, Convergent Validity, and Internal Responsiveness For Two Scoring SystemsDocument8 pagesThe Performance Quality Rating Scale (PQRS) : Reliability, Convergent Validity, and Internal Responsiveness For Two Scoring SystemsCarol AlvaradoNo ratings yet
- 4th Sem 651 Occupational ProfileDocument19 pages4th Sem 651 Occupational Profileapi-291545292100% (1)
- Cognitive Rehabilitation For Occupational Outcomes After Traumatic Brain InjuryDocument9 pagesCognitive Rehabilitation For Occupational Outcomes After Traumatic Brain InjuryHardeep Singh BaliNo ratings yet
- CC StrokeDocument13 pagesCC Strokeapi-436090845100% (1)
- Pool Activity Level (PAL) Instrument For Occupational ProfilingDocument35 pagesPool Activity Level (PAL) Instrument For Occupational ProfilingAngela GohNo ratings yet
- Occupational Therapy For Spinal Cord Injury PatientsDocument8 pagesOccupational Therapy For Spinal Cord Injury Patientsvenkata ramakrishnaiahNo ratings yet
- Artifact 5 Soap NoteDocument3 pagesArtifact 5 Soap Noteapi-517998988No ratings yet
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument17 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherValeria Sousa de AndradeNo ratings yet
- Understanding Occupational Transitions in Forced Migration The Importance of Life Skills in Early Refugee ResettlementDocument11 pagesUnderstanding Occupational Transitions in Forced Migration The Importance of Life Skills in Early Refugee ResettlementAlejandroAndrésAlvarezContrerasNo ratings yet
- Implementing Occupation-Based PracticeDocument10 pagesImplementing Occupation-Based Practiceapi-392268685No ratings yet
- Home Environmental AssessmentDocument2 pagesHome Environmental AssessmentSelvi Puspa SariNo ratings yet
- Initial TemplateDocument8 pagesInitial TemplateZuj PayNo ratings yet
- Occupational Therapy Now Volume 14.5Document32 pagesOccupational Therapy Now Volume 14.5Sara Gomes CastroNo ratings yet
- Cognition, Cognitive Rehabilitation, and Occupational PerformanceDocument23 pagesCognition, Cognitive Rehabilitation, and Occupational PerformanceMaria AiramNo ratings yet
- Occupational Identity Disruption After Traumatic Brain Injury - An Approach To Occupational Therapy Evaluation and TreatmentDocument13 pagesOccupational Identity Disruption After Traumatic Brain Injury - An Approach To Occupational Therapy Evaluation and Treatmentapi-234120429No ratings yet
- Kristen Kincaid Occupational Analysis & Intervention PlanDocument23 pagesKristen Kincaid Occupational Analysis & Intervention Planapi-282525755100% (1)
- Ebp PaperDocument16 pagesEbp Paperapi-583545759No ratings yet
- Strategies Used by Occupational Therapy To Maximize ADL IndependenceDocument53 pagesStrategies Used by Occupational Therapy To Maximize ADL IndependenceNizam lotfi100% (1)
- Occupational Profile M Viveros FinalDocument19 pagesOccupational Profile M Viveros Finalapi-293258738No ratings yet
- Occupational AdaptationDocument5 pagesOccupational AdaptationVASH12345100% (1)
- Functional Capacity Evaluation: Occupational Therapy's Role inDocument2 pagesFunctional Capacity Evaluation: Occupational Therapy's Role inramesh babu100% (1)
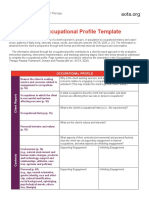
- AOTA Occupational Profile TemplateDocument2 pagesAOTA Occupational Profile TemplateYayan100% (1)
- Home Base Intervention OtDocument9 pagesHome Base Intervention OtPaulinaNo ratings yet
- Article 1Document7 pagesArticle 1dguginNo ratings yet
- Occupational Profile and Intervention PlanDocument18 pagesOccupational Profile and Intervention Planapi-282525755No ratings yet
- The Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionFrom EverandThe Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionNo ratings yet
- Occupational Therapy and Life Course Development: A Work Book for Professional PracticeFrom EverandOccupational Therapy and Life Course Development: A Work Book for Professional PracticeNo ratings yet
- PsmsformsDocument1 pagePsmsformsapi-261670650No ratings yet
- Final Cat Sylvia & ElizabethDocument11 pagesFinal Cat Sylvia & Elizabethapi-261670650No ratings yet
- FwevalDocument4 pagesFwevalapi-261670650No ratings yet
- Poster Systematic ReviewDocument1 pagePoster Systematic Reviewapi-261670650No ratings yet
- Niemyjski Sylvia Occupational Profile and Intervention FinalDocument17 pagesNiemyjski Sylvia Occupational Profile and Intervention Finalapi-261670650No ratings yet
- Casestudy520finalpaper 1Document19 pagesCasestudy520finalpaper 1api-261670650No ratings yet
- TracheostomyDocument29 pagesTracheostomyFemi AustinNo ratings yet
- Radio Immuno As SayDocument35 pagesRadio Immuno As SayDawlat SalamaNo ratings yet
- Gastrostomy and JejunostomyDocument43 pagesGastrostomy and JejunostomyLeslie Anne Alcibar TababaNo ratings yet
- Case Presentation: La Consolacion University Philippines Malolos City, BulacanDocument6 pagesCase Presentation: La Consolacion University Philippines Malolos City, BulacanElijah MancoNo ratings yet
- Cervicogenic HeadacheDocument7 pagesCervicogenic Headachemeta456No ratings yet
- Demografi Rawat Inap PDFDocument90 pagesDemografi Rawat Inap PDFNhaddz ERnNo ratings yet
- A Buccal Mucosa Ulcer As The First Sign Of.24Document5 pagesA Buccal Mucosa Ulcer As The First Sign Of.24liz chirinosNo ratings yet
- HHS Public Access: Chest Radiographic Findings and Outcomes of Pneumonia Among Children in BotswanaDocument14 pagesHHS Public Access: Chest Radiographic Findings and Outcomes of Pneumonia Among Children in BotswanagarexathNo ratings yet
- Corn MealDocument2 pagesCorn MealSantosh YeleNo ratings yet
- Patient Positioning in ORDocument28 pagesPatient Positioning in ORJoshua SmithNo ratings yet
- 2019 Developmentofthe PMGQand Prevalenceof Mobile Gaming Addiction Among Adolescentsin Taiwan Cyberpsychol Behav Soc NetwDocument8 pages2019 Developmentofthe PMGQand Prevalenceof Mobile Gaming Addiction Among Adolescentsin Taiwan Cyberpsychol Behav Soc NetwJr BagaporoNo ratings yet
- Antimicrobial StewardshipDocument7 pagesAntimicrobial StewardshipJohn TusselNo ratings yet
- Ingle's EndodonticsDocument50 pagesIngle's EndodonticsAndrei Antipin100% (1)
- Sample Charting (Fdar)Document3 pagesSample Charting (Fdar)Mary Beth AbelidoNo ratings yet
- FeverDocument29 pagesFeverYogesh KharcheNo ratings yet
- BERADocument19 pagesBERADr.shradhaNo ratings yet
- Nosocomial: Infections in The Neonatal Intensive Care UnitDocument9 pagesNosocomial: Infections in The Neonatal Intensive Care UnitCleoanne Gallegos100% (1)
- GROUP 3 - CASE STUDY - TraumaDocument5 pagesGROUP 3 - CASE STUDY - TraumaDinarkram Rabreca EculNo ratings yet
- Indonesia Hires OK PDFDocument94 pagesIndonesia Hires OK PDFikaNo ratings yet
- Combined Science b8Document6 pagesCombined Science b8Jose ArcosNo ratings yet
- Blood ConservationDocument7 pagesBlood ConservationbobbykrishNo ratings yet
- Moore Kiana - Family Planning BrochureDocument2 pagesMoore Kiana - Family Planning Brochureapi-518091160No ratings yet
- Prof. Eman Rushdy Sulphonylurea A Golden Therapy For DiabetesDocument51 pagesProf. Eman Rushdy Sulphonylurea A Golden Therapy For Diabetestorr123No ratings yet
- Capstone g7 Chapter 1Document7 pagesCapstone g7 Chapter 1Jabez Flores NatividadNo ratings yet
- Carti Libraria Victor Papilian Ian 2015Document8 pagesCarti Libraria Victor Papilian Ian 2015Petru AcozmeiNo ratings yet
- ACE Inhibitors Vs ARBs Is One Class Better For HeaDocument7 pagesACE Inhibitors Vs ARBs Is One Class Better For HeaZul Qodri GintingNo ratings yet
- Hazard and Risk For Nurse in HospitalDocument4 pagesHazard and Risk For Nurse in HospitalFaraahNo ratings yet
- Respiratory Distress Syndrome in A Premature BabyDocument29 pagesRespiratory Distress Syndrome in A Premature BabyVissalini JayabalanNo ratings yet