Download as docx, pdf, or txt
You might also like
- Physiological Ion ChlorideDocument15 pagesPhysiological Ion ChlorideMohammad Arafat Siddiqui100% (2)
- Metabolic Alkalosis (Base Bicarbonate Excess) I. Brief DescriptionDocument3 pagesMetabolic Alkalosis (Base Bicarbonate Excess) I. Brief DescriptionAllyssa MackinnonNo ratings yet
- Renal Tubular Acidosis: Moderator:Dr Nitin Joshi Presented By: Dr. Parth Nathwani MGM Medical College, MumbaiDocument71 pagesRenal Tubular Acidosis: Moderator:Dr Nitin Joshi Presented By: Dr. Parth Nathwani MGM Medical College, MumbaiariNo ratings yet
- Chemistry Pool ERTDocument15 pagesChemistry Pool ERTKatty TsaiNo ratings yet
- Serum Electrolytes-Part 1Document22 pagesSerum Electrolytes-Part 1Marwa 2002No ratings yet
- Chloride, Bicarbonate and LactateDocument32 pagesChloride, Bicarbonate and LactateElla OrtegaNo ratings yet
- POTASSIUM HOMEOSTASIS كيمياء سريريةDocument4 pagesPOTASSIUM HOMEOSTASIS كيمياء سريريةMustafa Salah MahdiNo ratings yet
- Chloride: By: Group 7Document13 pagesChloride: By: Group 7Juvial DavidNo ratings yet
- Anion Gap Metabolic Acidemia Case BasedDocument4 pagesAnion Gap Metabolic Acidemia Case Basedspiros.a.markouNo ratings yet
- Chloride Deficit LecDocument2 pagesChloride Deficit Leced123edNo ratings yet
- Metabolic Alkalosis: David S. Goldfarb and Jon-Emile S. KennyDocument8 pagesMetabolic Alkalosis: David S. Goldfarb and Jon-Emile S. Kennyandi siregarNo ratings yet
- Ms. Divyakrit AroraDocument15 pagesMs. Divyakrit ArorarkdivyaNo ratings yet
- Ion TransportersDocument2 pagesIon TransportersfilipemedicinavrNo ratings yet
- 2013 Renal Tubular AcidosisDocument13 pages2013 Renal Tubular AcidosisLUIS FRANCISCO GUERRERO MARTÍNEZNo ratings yet
- Renal Tubular AcidosisDocument59 pagesRenal Tubular Acidosiskash_buNo ratings yet
- Chlorine TerminologyDocument3 pagesChlorine Terminologyghost2humanNo ratings yet
- Approach To Metabolic AlkalosisDocument11 pagesApproach To Metabolic AlkalosisJou ÁlvarezNo ratings yet
- PUCAN, Julienne BSN III-D - SGD - HYPO&HYPERCHLOREMIADocument10 pagesPUCAN, Julienne BSN III-D - SGD - HYPO&HYPERCHLOREMIAJulienne PucanNo ratings yet
- Components of Renal SystemDocument5 pagesComponents of Renal SystemHuzaifa TahirNo ratings yet
- Chloride The Queen of ElectrolytesDocument9 pagesChloride The Queen of ElectrolytesYancy Erazo DoradoNo ratings yet
- DUIRETICSDocument41 pagesDUIRETICSJohnsonNo ratings yet
- Asidosis Metabolik PDFDocument6 pagesAsidosis Metabolik PDFafifurrahman_rizalNo ratings yet
- Chloride CompleteDocument8 pagesChloride CompleteGul Rehman GulNo ratings yet
- Jurnal DM 2Document7 pagesJurnal DM 2Elang SudewaNo ratings yet
- Acid-Base BalanceDocument28 pagesAcid-Base Balanceps4only100% (1)
- Acid Base Disorders MBBSDocument44 pagesAcid Base Disorders MBBSphuyalaryan666No ratings yet
- Cystic Fibrosis Cystic FibrosisDocument3 pagesCystic Fibrosis Cystic FibrosisleenNo ratings yet
- DiureticsDocument75 pagesDiureticsSilpa Jayakumar100% (5)
- Lec 14 - Kidney PDFDocument16 pagesLec 14 - Kidney PDFrajeshNo ratings yet
- Chloremia (Hypochloremia) & Acute and Chronic Respiratory Alkalosis (Carbonic Acid Deficit)Document4 pagesChloremia (Hypochloremia) & Acute and Chronic Respiratory Alkalosis (Carbonic Acid Deficit)KQarlo Luis Pestaño Maniaol100% (1)
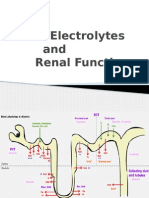
- Electrolytes and Renal FunctionDocument7 pagesElectrolytes and Renal FunctionUhjafwnuijhnfa KmerkgoeNo ratings yet
- Deepak AssignmentDocument5 pagesDeepak AssignmentDEEPAK YadavNo ratings yet
- Wikipedia - Anion Gap (CHECKED)Document6 pagesWikipedia - Anion Gap (CHECKED)vitruvianxyzNo ratings yet
- Metabolic AlkalosisDocument8 pagesMetabolic AlkalosisPauline PerezNo ratings yet
- Acid BaseDocument21 pagesAcid BaseAngela Danielle TanNo ratings yet
- Hypokalemia: A Practical Approach To Diagnosis and TreatmentDocument17 pagesHypokalemia: A Practical Approach To Diagnosis and TreatmentIntan NoaNo ratings yet
- Metabolic AlkalosisDocument2 pagesMetabolic AlkalosisKath ComodaNo ratings yet
- ELECTROLYTESDocument7 pagesELECTROLYTESSleepy AssNo ratings yet
- Part 1 - US-Grade 4-BiochemistryDocument34 pagesPart 1 - US-Grade 4-BiochemistryFarah Bashar Al-RawachyNo ratings yet
- Anionic GapDocument8 pagesAnionic GapMaria-Larisa HohanNo ratings yet
- Diuretics: Pranjal Wagh Master of Pharmacy (2021-2023) Poona College of PharmacyDocument39 pagesDiuretics: Pranjal Wagh Master of Pharmacy (2021-2023) Poona College of PharmacyPranjalNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CKDocument15 pagesDr. Ali's Uworld Notes For Step 2 CKBoogy WoogyNo ratings yet
- Fluid and Electrolyte by Dr. MohsinDocument73 pagesFluid and Electrolyte by Dr. MohsinKrishna RajakumarNo ratings yet
- Dangerous Rhythms Tachycardia: Potassium Electrolyte HypokalemiaDocument7 pagesDangerous Rhythms Tachycardia: Potassium Electrolyte HypokalemiagorodoeNo ratings yet
- Acidification of UrineDocument14 pagesAcidification of UrineMohan BNo ratings yet
- Disorders of Potassium MetabolismDocument11 pagesDisorders of Potassium MetabolismKamal Kumar Kamal KumarNo ratings yet
- Renal System 2: Transport Properties of Nephron SegmentsDocument5 pagesRenal System 2: Transport Properties of Nephron SegmentsSherida GibbsNo ratings yet
- Medical Surgical Nursing TionkoDocument40 pagesMedical Surgical Nursing TionkojeshemaNo ratings yet
- DETERMINATION OF ALKALINITY BY A PH TITRATIONDocument3 pagesDETERMINATION OF ALKALINITY BY A PH TITRATIONThato NkhemeNo ratings yet
- Dagumbal Fluid and ElectrolyteDocument9 pagesDagumbal Fluid and ElectrolyteAlvin DagumbalNo ratings yet
- Secretion of Ions in SalivaDocument5 pagesSecretion of Ions in SalivabhumiparikhNo ratings yet
- Salty-Testing Skin, Chronic Respiratory Problems, Lung Infections, Poor Growth/weight Loss, Meconium IleusDocument8 pagesSalty-Testing Skin, Chronic Respiratory Problems, Lung Infections, Poor Growth/weight Loss, Meconium IleusOrhan AsdfghjklNo ratings yet
- 12 Bicarbonate, Calcium, Phosphate and MagnesiumDocument38 pages12 Bicarbonate, Calcium, Phosphate and MagnesiumFrances FranciscoNo ratings yet
- Chapter 3 CVS & RenalDocument116 pagesChapter 3 CVS & RenalKIDUS YAREDNo ratings yet
- Arterial Blood GasDocument14 pagesArterial Blood Gasannatw100% (1)
- Clinical Chemistry: Presented by Alyazeed Hussein, BSCDocument43 pagesClinical Chemistry: Presented by Alyazeed Hussein, BSCMONFOLANo ratings yet
- Pharmacology of Renal SystemDocument125 pagesPharmacology of Renal SystemBirhanu GetaNo ratings yet
- Nephron PhysiologyDocument8 pagesNephron PhysiologyHadeel A. AlkayedNo ratings yet
- Urinary Stones: Medical and Surgical ManagementFrom EverandUrinary Stones: Medical and Surgical ManagementMichael GrassoNo ratings yet