Download as ppt, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Put Your Heart in Your Mouth by Natasha Campbell-McBrideDocument2 pagesPut Your Heart in Your Mouth by Natasha Campbell-McBrideIoana Brăteanu50% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pharmacology UNIT 1 - Lesson 1Document29 pagesPharmacology UNIT 1 - Lesson 1Bea Bianca CruzNo ratings yet
- Species Common/Other Name Pathogenesis Mot/Infective Stage Diagnostic Stage I. NematodesDocument2 pagesSpecies Common/Other Name Pathogenesis Mot/Infective Stage Diagnostic Stage I. NematodesautumntreesNo ratings yet
- The American College of Radiology BI-RADS Atlas 5 Edition: Frequently Asked QuestionsDocument18 pagesThe American College of Radiology BI-RADS Atlas 5 Edition: Frequently Asked QuestionssatanioNo ratings yet
- Medscape RegistrationDocument8 pagesMedscape RegistrationhalayehiahNo ratings yet
- Work Psychology Understanding Human BehaDocument2 pagesWork Psychology Understanding Human BehahalayehiahNo ratings yet
- L 7 Informed Consent & L8 Nursing LawDocument47 pagesL 7 Informed Consent & L8 Nursing LawhalayehiahNo ratings yet
- Medical Literacy Case StudyDocument2 pagesMedical Literacy Case StudyhalayehiahNo ratings yet
- Individual Assignment PCT Moduel 3 Model AnswerDocument4 pagesIndividual Assignment PCT Moduel 3 Model AnswerhalayehiahNo ratings yet
- Long-Term Care SettingsDocument20 pagesLong-Term Care SettingshalayehiahNo ratings yet
- 2-Cardiac Electical ActivityDocument26 pages2-Cardiac Electical ActivityhalayehiahNo ratings yet
- Tooth Anatomy QuizDocument2 pagesTooth Anatomy QuizhalayehiahNo ratings yet
- Role Transition Among Baccalaureate Nursing Students at Umm Al Qura UniversityDocument1 pageRole Transition Among Baccalaureate Nursing Students at Umm Al Qura UniversityhalayehiahNo ratings yet
- Power, Politics and Delegation in Professional Nursing PracticeDocument28 pagesPower, Politics and Delegation in Professional Nursing PracticehalayehiahNo ratings yet
- Code of Ethics For Healthcare PractitionDocument60 pagesCode of Ethics For Healthcare PractitionhalayehiahNo ratings yet
- SpssDocument67 pagesSpsshalayehiahNo ratings yet
- Assessing With EliminationDocument79 pagesAssessing With EliminationhalayehiahNo ratings yet
- Patient Culture Safety3 Poster (2379)Document2 pagesPatient Culture Safety3 Poster (2379)halayehiahNo ratings yet
- Human Behavior in WorkplaceDocument58 pagesHuman Behavior in WorkplacehalayehiahNo ratings yet
- Introductin To ResearchDocument7 pagesIntroductin To ResearchhalayehiahNo ratings yet
- 2nd Lecture Normal Phsiological Changes of Aging Final1.Ppt40-41Document85 pages2nd Lecture Normal Phsiological Changes of Aging Final1.Ppt40-41halayehiahNo ratings yet
- Results: Manal M. Ibrahim, Manal H. Abou Al-Magd, & Hala Y. SayedDocument1 pageResults: Manal M. Ibrahim, Manal H. Abou Al-Magd, & Hala Y. SayedhalayehiahNo ratings yet
- Poster Reserch Hala YehiaDocument1 pagePoster Reserch Hala YehiahalayehiahNo ratings yet
- Human ResourcesDocument75 pagesHuman ResourceshalayehiahNo ratings yet
- CH 20Document23 pagesCH 20halayehiahNo ratings yet
- SchedulingDocument20 pagesSchedulinghalayehiahNo ratings yet
- AssigmentDocument51 pagesAssigmenthalayehiahNo ratings yet
- Patient Satisfaction: "We Are Listening-"Document17 pagesPatient Satisfaction: "We Are Listening-"DivyaDeepthi18No ratings yet
- Prof BoundariesDocument36 pagesProf BoundarieshalayehiahNo ratings yet
- Research in NursingDocument37 pagesResearch in NursinghalayehiahNo ratings yet
- Checklist For Research ProposalsDocument2 pagesChecklist For Research ProposalshalayehiahNo ratings yet
- MBEB - Mindfulness-Based Emotional Balance Teacher Training IntensiveDocument10 pagesMBEB - Mindfulness-Based Emotional Balance Teacher Training IntensiveLina SantosNo ratings yet
- Capítulo 10 SerdevDocument19 pagesCapítulo 10 SerdevErik BrooksNo ratings yet
- List of Private Testing Labs in Kerala For Covid 19 As On October 22Document19 pagesList of Private Testing Labs in Kerala For Covid 19 As On October 22pushpanarayananNo ratings yet
- Journal of Scoupus IndexedDocument458 pagesJournal of Scoupus IndexedEndang TriyantoNo ratings yet
- TorchDocument10 pagesTorchAyen Fajardo-HernalNo ratings yet
- Resource Guide - Model Nbs PolicyDocument7 pagesResource Guide - Model Nbs PolicyagelesswapNo ratings yet
- Agostino Et Al-2014-Cochrane Database of Systematic Reviews PDFDocument61 pagesAgostino Et Al-2014-Cochrane Database of Systematic Reviews PDFdruzair007No ratings yet
- Anaesthetic Management of Patients With Cardiac Pacemakers and Defibrillators For Noncardiac SurgeryDocument12 pagesAnaesthetic Management of Patients With Cardiac Pacemakers and Defibrillators For Noncardiac SurgeryzaheerNo ratings yet
- SAI's vs. STD'S: - Syphilis - Chlamydia - Vaginitis - Herpes - GonnorheaDocument25 pagesSAI's vs. STD'S: - Syphilis - Chlamydia - Vaginitis - Herpes - GonnorheaMark CheneyNo ratings yet
- Digestion & Absorption of CarbohydratesDocument14 pagesDigestion & Absorption of CarbohydratesKuzhandai VeluNo ratings yet
- Glenn Gould and Finger TappingDocument3 pagesGlenn Gould and Finger Tappingnuunumcl100% (1)
- TN Medical CoursesDocument112 pagesTN Medical CoursesdansanxNo ratings yet
- Msds Guano DiscsDocument5 pagesMsds Guano Discsapi-289433849No ratings yet
- Cervical Vertigo PDFDocument5 pagesCervical Vertigo PDFPaijo SusenoNo ratings yet
- Mouse PartsDocument1 pageMouse PartsBea JulongbayanNo ratings yet
- Aspartame Side EffectsDocument3 pagesAspartame Side Effectsnettie95No ratings yet
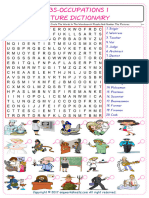
- Jobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Document2 pagesJobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Raquel NoeliaNo ratings yet
- Thyroid Iodine Special ReportDocument6 pagesThyroid Iodine Special ReportRxOuzoNo ratings yet
- OPD Schedule Jan-Feb 23Document22 pagesOPD Schedule Jan-Feb 23Ajay DherwaniNo ratings yet
- Case 13 - People v. Ulep, G.R. No. L-36858Document5 pagesCase 13 - People v. Ulep, G.R. No. L-36858Jo-Al GealonNo ratings yet
- Tuberculosis (TB) Blood Test (IGRA) : Minnesota Department of HealthDocument1 pageTuberculosis (TB) Blood Test (IGRA) : Minnesota Department of HealthYeon Ae NaritaNo ratings yet
- Staining Intracellular Antigens For Flow CytometryDocument5 pagesStaining Intracellular Antigens For Flow CytometryAditya Satriya NugrahaNo ratings yet
- Uwise ReviewDocument14 pagesUwise ReviewAnonymous T1G9BQQNo ratings yet
- Stephen's Story: A 19 Year Old'S Life Lessons OnDocument16 pagesStephen's Story: A 19 Year Old'S Life Lessons OnSylvia DobsonNo ratings yet
- Iceman TattoosDocument3 pagesIceman TattoosfuturearunaNo ratings yet
- 2018 SEAOHUN Scholarship DetailDocument1 page2018 SEAOHUN Scholarship DetailQurratu A'yuninNo ratings yet