Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Big Pharma's Worst NightmareDocument51 pagesBig Pharma's Worst NightmaredjoleNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Santrock Section 3 InfancyDocument21 pagesSantrock Section 3 InfancyAssumpta Minette Burgos100% (5)
- +english - Oral Matura Jachs - All TopicsDocument37 pages+english - Oral Matura Jachs - All Topicsapi-3754905100% (1)
- NewzoologynormalDocument12 pagesNewzoologynormalgupta_punNo ratings yet
- Historyof Genetics QuizDocument2 pagesHistoryof Genetics QuizGelli NancaNo ratings yet
- Case Study - Endocrine System PDFDocument3 pagesCase Study - Endocrine System PDFYusra Angel DelfinNo ratings yet
- Optimal Management of Collagenous Colitis A Review 021016Document9 pagesOptimal Management of Collagenous Colitis A Review 021016Eliza DNNo ratings yet
- History of The SADS Foundation and Long QT SyndromeDocument4 pagesHistory of The SADS Foundation and Long QT Syndromeapi-341217779No ratings yet
- Brianbee Sample Questions 1 PDFDocument2 pagesBrianbee Sample Questions 1 PDFLigeia100% (1)
- Notes On ImmunoserologyDocument7 pagesNotes On ImmunoserologyTiffany RemiendoNo ratings yet
- Howlett Paper 09182013Document6 pagesHowlett Paper 09182013FutantxxyzNo ratings yet
- Nanopharmaceutical Drugs MarketDocument15 pagesNanopharmaceutical Drugs Marketnox27No ratings yet
- DeFronzo Et Al-2012-Diabetes, Obesity and MetabolismDocument10 pagesDeFronzo Et Al-2012-Diabetes, Obesity and MetabolismlguerreroNo ratings yet
- Autoimmune Syndromes and Inflammatory Sy PDFDocument105 pagesAutoimmune Syndromes and Inflammatory Sy PDFdragosNo ratings yet
- E-Reader Beadle To Derrida in Word 2003Document145 pagesE-Reader Beadle To Derrida in Word 2003rosarevolNo ratings yet
- Musculoskeletal System L1Document28 pagesMusculoskeletal System L1BoazNo ratings yet
- Perdev ReviewerDocument11 pagesPerdev ReviewerSofiaNo ratings yet
- Oralpatho SEQDocument16 pagesOralpatho SEQKhushboo e ZehraNo ratings yet
- HydrocephalusDocument17 pagesHydrocephalusapi-265714286No ratings yet
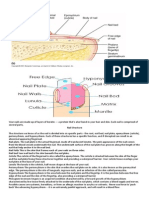
- Your Nails Are Made Up of Layers of KeratinDocument2 pagesYour Nails Are Made Up of Layers of KeratinRetchel LiwagonNo ratings yet
- Pt. Pathlab Indonesia: (Laboratorium Klinik)Document1 pagePt. Pathlab Indonesia: (Laboratorium Klinik)Aghiest Utungga Al BirruNo ratings yet
- Modified IntroductionDocument28 pagesModified IntroductionNormana ZureikatNo ratings yet
- Pathogenesis & Prognosis LeukoplakiaDocument4 pagesPathogenesis & Prognosis LeukoplakiaSundhias LarashatiNo ratings yet
- Chapter 13: Viruses: 13.1 General StructuresDocument3 pagesChapter 13: Viruses: 13.1 General StructuresASPEN FERNANDONo ratings yet
- Morens Doc FinalDocument6 pagesMorens Doc FinalGregory PriceNo ratings yet
- Coagulation StudyDocument57 pagesCoagulation Studytanweer_elevenNo ratings yet
- Articulo MalariaDocument19 pagesArticulo MalariaAndres Felipe DuqueNo ratings yet
- Part 1: Listen To The Recording Twice. Complete The Table Below. Write ONEDocument19 pagesPart 1: Listen To The Recording Twice. Complete The Table Below. Write ONEyamedagomenasaiNo ratings yet
- Chapter 27 - Anxiety-Related, Obsessive-Compulsive, Trauma and Stressor-Related, Somatic, and Dissociative DisordersDocument10 pagesChapter 27 - Anxiety-Related, Obsessive-Compulsive, Trauma and Stressor-Related, Somatic, and Dissociative DisordersKTNo ratings yet
- Stages of Prenatal Development Causes of Development DiseasesDocument2 pagesStages of Prenatal Development Causes of Development DiseasesAnnah Caponpon GalorNo ratings yet