Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Eye Care We Care Photo ReportsDocument11 pagesEye Care We Care Photo ReportsNOMER NAVARRO VARUANo ratings yet
- Galeazzi Fracture and Monteggia FractureDocument31 pagesGaleazzi Fracture and Monteggia FracturenihthaNo ratings yet
- Ventricular Septal Defect VSD FactsheetDocument3 pagesVentricular Septal Defect VSD FactsheetArgolekso RatriNo ratings yet
- Fundamental of Nursing: Unit OneDocument13 pagesFundamental of Nursing: Unit OneSumaira NoreenNo ratings yet
- LIMFANGIOLEIOMATOZADocument11 pagesLIMFANGIOLEIOMATOZAAbuzdea AlexNo ratings yet
- Fundamentals of Nursing NCLEX Practice Quiz 1 (25 Items)Document16 pagesFundamentals of Nursing NCLEX Practice Quiz 1 (25 Items)Akia Cayasan BayaNo ratings yet
- Presentation On Renal CalculiDocument16 pagesPresentation On Renal CalculiSangay CheshireNo ratings yet
- Brain InjuryDocument50 pagesBrain InjuryMuhammad Abdul RahmanNo ratings yet
- Ledge Pada PsaDocument9 pagesLedge Pada Psacrush crushNo ratings yet
- Pipa Guidance Document: Responding To Patient EnquiriesDocument6 pagesPipa Guidance Document: Responding To Patient EnquiriesSabina PetrarNo ratings yet
- Effects of Massage On Delayed-Onset Muscle Soreness, Swelling, and Recovery of Muscle FunctionDocument7 pagesEffects of Massage On Delayed-Onset Muscle Soreness, Swelling, and Recovery of Muscle FunctionjaviNo ratings yet
- Risk For Injury DengueDocument3 pagesRisk For Injury DengueLouise BandalaNo ratings yet
- Slide Lokakarya Insulin Makassar Sept 2004Document45 pagesSlide Lokakarya Insulin Makassar Sept 2004Dian SobaNo ratings yet
- Adult Bacterial Conjunctivitis: Resistance Patterns Over 12 Years in Patients Attending A Large Primary Eye Care Centre in The UKDocument4 pagesAdult Bacterial Conjunctivitis: Resistance Patterns Over 12 Years in Patients Attending A Large Primary Eye Care Centre in The UKegyzellahsNo ratings yet
- TB Flipchart RSDocument30 pagesTB Flipchart RSMuhammad Hasbul100% (1)
- Paul S. Appelbaum M.DDocument54 pagesPaul S. Appelbaum M.DMarkingsonCaseNo ratings yet
- Rak Single DentureDocument48 pagesRak Single Denturerakes0No ratings yet
- 2005 - EMCNA - Disorders of PotassiumDocument25 pages2005 - EMCNA - Disorders of PotassiummagnavlerNo ratings yet
- Sa Mental HealthDocument9 pagesSa Mental HealthKimberly Camacho CatubigNo ratings yet
- Chapter 14 Personality Outline AP PsychologyDocument4 pagesChapter 14 Personality Outline AP Psychologyccarroll2722100% (2)
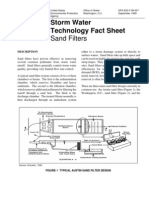
- Storm Water Technology - Sand FiltersDocument7 pagesStorm Water Technology - Sand FiltersGreen Action Sustainable Technology GroupNo ratings yet
- Medical Leave of Absence (Mloa) Treatment Provider Report: SECTION I: To Be Completed by The StudentDocument4 pagesMedical Leave of Absence (Mloa) Treatment Provider Report: SECTION I: To Be Completed by The StudentShubho DasNo ratings yet
- Cytochrome P450 PharmacogeneticsDocument3 pagesCytochrome P450 PharmacogeneticsSiegfriedCristoforNo ratings yet
- Spinal Neurosurgery 1St Edition James Harrop Editor All ChapterDocument67 pagesSpinal Neurosurgery 1St Edition James Harrop Editor All Chapterronald.kotson988No ratings yet
- Nursing Care Plan: Cues Nursing Diagnosis Analysis Goal and Objectives Interventions Rationale EvaluationDocument3 pagesNursing Care Plan: Cues Nursing Diagnosis Analysis Goal and Objectives Interventions Rationale EvaluationCalimlim KimNo ratings yet
- A Network Meta-Analysis On The Effects of Information Technology Application On Preoperative Anxiety of PatientsDocument7 pagesA Network Meta-Analysis On The Effects of Information Technology Application On Preoperative Anxiety of PatientsInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Current Opinion Hematol RR AML 2019Document8 pagesCurrent Opinion Hematol RR AML 2019Ernesto PiconNo ratings yet
- Positioning Techniques in Long-Term Care: Self-Directed Learning Package For Health Care ProvidersDocument41 pagesPositioning Techniques in Long-Term Care: Self-Directed Learning Package For Health Care ProvidersHbk RajneeshNo ratings yet
- Different Types of Bath PresentationDocument55 pagesDifferent Types of Bath PresentationThomas Mathew100% (2)
- Complications in Dentoalveolar Surgery PDFDocument37 pagesComplications in Dentoalveolar Surgery PDFmirfanulhaqNo ratings yet