
Medical Form
Medical Form
You might also like
- Crown Pallet PC 4500 Parts Catalog Maintenance Service Manual en FRDocument22 pagesCrown Pallet PC 4500 Parts Catalog Maintenance Service Manual en FRjohnathanfoster080802obr96% (27)
- Registration For ChildcareDocument2 pagesRegistration For Childcareapi-315547754No ratings yet
- Associate CalassDocument151 pagesAssociate CalassMuhammad Naveed AnjumNo ratings yet
- 12 Years A SlaveDocument2 pages12 Years A SlaveismanNo ratings yet
- Student MedicalDocument1 pageStudent MedicalbbruntNo ratings yet
- ChildenrollmentpapersDocument7 pagesChildenrollmentpapersapi-531837774No ratings yet
- Junior Tours Medical ReleaseDocument1 pageJunior Tours Medical Releaseapi-235166650No ratings yet
- Parent/Guardian Information: Continued On ReverseDocument2 pagesParent/Guardian Information: Continued On Reverseadhi eng lrtNo ratings yet
- Urgentcare FormDocument4 pagesUrgentcare Formapi-287654333No ratings yet
- GCCSACCEmergency Card InformationDocument1 pageGCCSACCEmergency Card InformationAl-juffrey Luis AmilhamjaNo ratings yet
- New Patient RegistrationDocument2 pagesNew Patient Registrationnaveenmi2100% (1)
- CDMedical AuthorizationDocument1 pageCDMedical Authorizationtrellon_devteamNo ratings yet
- Registration 2010 2011Document3 pagesRegistration 2010 2011cubanita11No ratings yet
- Teen MedicalDocument1 pageTeen MedicalJohn C StarkNo ratings yet
- Liability Release and Parental Consent FormDocument3 pagesLiability Release and Parental Consent Formapi-28674765No ratings yet
- Student Information Sheet 2Document2 pagesStudent Information Sheet 2jhon jhon millareNo ratings yet
- Enrollment PacketDocument3 pagesEnrollment Packetapi-741820810No ratings yet
- Patient Registration Form 13Document4 pagesPatient Registration Form 13windawaty humolaNo ratings yet
- General Release / Permission Form: ACTIVITIES: (Initial All That Apply)Document2 pagesGeneral Release / Permission Form: ACTIVITIES: (Initial All That Apply)Megan JonesNo ratings yet
- Clinical Health RequirementsDocument6 pagesClinical Health RequirementsbarneylovesbagelsNo ratings yet
- Pcs Emergency Permission Form - 21-22Document1 pagePcs Emergency Permission Form - 21-22api-671085061No ratings yet
- Asthma Inhaler FormDocument1 pageAsthma Inhaler Formheather579No ratings yet
- Student Enrollment FormDocument3 pagesStudent Enrollment Formapi-239237152No ratings yet
- Uprising Medical Release FormDocument1 pageUprising Medical Release Formone dollar youth ministryNo ratings yet
- Patient InformationDocument10 pagesPatient InformationFatimahNo ratings yet
- Official Medical Information and Release FormDocument2 pagesOfficial Medical Information and Release FormtheNOLAtreeNo ratings yet
- Health FormDocument2 pagesHealth Formamanda6254No ratings yet
- Brown Hearing Centers: Personal InformationDocument2 pagesBrown Hearing Centers: Personal InformationEddie TooheyNo ratings yet
- Next Gen Med ReleaseDocument2 pagesNext Gen Med ReleaserfbcgreenvilleNo ratings yet
- Af Cavemen Cheer Try-Out PacketDocument5 pagesAf Cavemen Cheer Try-Out PacketAf CheerNo ratings yet
- Student Assurance Services, Inc. P.O. Box 196 STILLWATER, MN 55082-0196Document1 pageStudent Assurance Services, Inc. P.O. Box 196 STILLWATER, MN 55082-0196Sharif M Mizanur RahmanNo ratings yet
- Dare To Dream 2011 Medical ReleaseDocument1 pageDare To Dream 2011 Medical Releaserls2orgNo ratings yet
- School Health Examination CardDocument3 pagesSchool Health Examination Cardjrose fay amatNo ratings yet
- Medical Waiver 2014-2015Document4 pagesMedical Waiver 2014-2015api-73377093No ratings yet
- Parent Permission Formed ItDocument1 pageParent Permission Formed Itannoyed4lyfeNo ratings yet
- Field Trip Permission SlipDocument1 pageField Trip Permission Slipapi-272734430No ratings yet
- Adult Health HistoryDocument1 pageAdult Health HistorySally Hansen100% (1)
- Registration FormDocument3 pagesRegistration FormcampsunshinenycNo ratings yet
- Genesis Academy Pre-K Program Registration Form: Child's InformationDocument7 pagesGenesis Academy Pre-K Program Registration Form: Child's InformationPhillip M JonesNo ratings yet
- Writable PC FormDocument1 pageWritable PC FormJulie Vyne ModalesNo ratings yet
- Enrollment PacketDocument6 pagesEnrollment Packetapi-382256148No ratings yet
- MedicalformDocument1 pageMedicalformapi-257833418No ratings yet
- Medical Form 2022-2023Document1 pageMedical Form 2022-2023Devin HouseholderNo ratings yet
- Permission FormDocument2 pagesPermission Formapi-295968636No ratings yet
- Vermara Kids Daycare Registration Form 2Document5 pagesVermara Kids Daycare Registration Form 2api-29050616No ratings yet
- 2009 Enrollment FormsDocument2 pages2009 Enrollment FormsesromseanNo ratings yet
- Registration Form DoctorDocument4 pagesRegistration Form DoctorAaditya Shyam2No ratings yet
- St. George AppDocument9 pagesSt. George AppFutureDDSNo ratings yet
- Parental Consent Forms For Minors Travelling Without ParentsDocument4 pagesParental Consent Forms For Minors Travelling Without ParentsLuckyTTinioNo ratings yet
- Student InformationDocument1 pageStudent Informationchantel_allenNo ratings yet
- Typhoid Fever: Administrative DemographicsDocument6 pagesTyphoid Fever: Administrative DemographicsMohan ChikkalaNo ratings yet
- YouthactivitiesconsentDocument1 pageYouthactivitiesconsentLaurie ThomasNo ratings yet
- Pds Medical-Cert Waiver 2023-RspcDocument1 pagePds Medical-Cert Waiver 2023-RspcRon MenesNo ratings yet
- PDS Medical-Cert Waiver 2024-RSPCDocument1 pagePDS Medical-Cert Waiver 2024-RSPCRose Andrea BergonioNo ratings yet
- Mena Bands Medical Release FormDocument1 pageMena Bands Medical Release Formapi-358909433No ratings yet
- Application For Admission - Prek & Kindergarten Program: Morning Extended Care (7:30-8:30 Am)Document4 pagesApplication For Admission - Prek & Kindergarten Program: Morning Extended Care (7:30-8:30 Am)Pedro barriaNo ratings yet
- 5.13 Field Trip FormDocument3 pages5.13 Field Trip FormLisa RossNo ratings yet
- CamperDocument1 pageCamperapi-223112910No ratings yet
- Parental Consent Form: For Youth Ministry StudentsDocument2 pagesParental Consent Form: For Youth Ministry StudentsAnonymous LYJ5Aj83cNo ratings yet
- HTCP Medical FormDocument2 pagesHTCP Medical Formapi-44699616No ratings yet
- Sifa Student Enrollment Packet Sy19 20Document5 pagesSifa Student Enrollment Packet Sy19 20Anonymous 49o5YzlNo ratings yet
- I-C-E in Case of Emergency: Your Essential Medical JournalFrom EverandI-C-E in Case of Emergency: Your Essential Medical JournalNo ratings yet
- Information Pack For Schools 2011-WebDocument35 pagesInformation Pack For Schools 2011-Webapi-144496227No ratings yet
- Camp Permission FormDocument1 pageCamp Permission Formapi-144496227No ratings yet
- ST Francis CollegeDocument1 pageST Francis Collegeapi-144496227No ratings yet
- Sleepover 2015Document1 pageSleepover 2015api-144496227No ratings yet
- Pcka Term 1 Timetable 2013Document1 pagePcka Term 1 Timetable 2013api-144496227No ratings yet
- Term 1 2013Document1 pageTerm 1 2013api-144496227No ratings yet
- Organization and Management LAS - Week 2Document4 pagesOrganization and Management LAS - Week 2Louie MunsayacNo ratings yet
- Exhibition Brochure-Embalsamada-Con-Picante (Embalmed With Spice)Document6 pagesExhibition Brochure-Embalsamada-Con-Picante (Embalmed With Spice)Isa SonNo ratings yet
- Our 16 Fundamental TruthsDocument10 pagesOur 16 Fundamental TruthsChristine Joy Verde SantiagoNo ratings yet
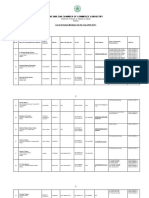
- OASGFO 2022 058 Requests For The Participation of Learners and Teachers in Extra CurricularDocument2 pagesOASGFO 2022 058 Requests For The Participation of Learners and Teachers in Extra CurricularRocky Nathaniel SalesNo ratings yet
- The Gender of The GiftDocument3 pagesThe Gender of The GiftMarcia Sandoval EsparzaNo ratings yet
- What Is Project Management Functions - These Big 8! - TompsDocument6 pagesWhat Is Project Management Functions - These Big 8! - TompsKavi MukilanNo ratings yet
- Foi Mtcu-100025 Bargaining Expenses Thu Aug 26 2010 08-26-27.142-1Document5 pagesFoi Mtcu-100025 Bargaining Expenses Thu Aug 26 2010 08-26-27.142-1Rob HorganNo ratings yet
- The Church House of God Fr. Tadros MalatyDocument354 pagesThe Church House of God Fr. Tadros MalatyIsa Almisry100% (3)
- Project Name: "New Arrivals": FNA Test PlanDocument6 pagesProject Name: "New Arrivals": FNA Test PlanNusrat HasanNo ratings yet
- Introduction and Preface To PFRS and Conceptual Framework: Theory of Accounts Preweek DiscussionDocument20 pagesIntroduction and Preface To PFRS and Conceptual Framework: Theory of Accounts Preweek DiscussionLeisleiRagoNo ratings yet
- Senoir Project-IrelandDocument12 pagesSenoir Project-Irelandapi-317313323No ratings yet
- Oracle Database 11 Product Family: An Oracle White Paper June 2012Document19 pagesOracle Database 11 Product Family: An Oracle White Paper June 2012Aliasger BharmalNo ratings yet
- MGT610 MIDTERM SOLVED MCQS by JUNAIDDocument33 pagesMGT610 MIDTERM SOLVED MCQS by JUNAIDtalha8389711100% (1)
- Vastu For House - Home Vastu Test - Vastu Shastra Score For House - Vastu House Facing - Vastu Shastra Home PDFDocument3 pagesVastu For House - Home Vastu Test - Vastu Shastra Score For House - Vastu House Facing - Vastu Shastra Home PDFSelvaraj VillyNo ratings yet
- Associated Gas Utilization Via MiniGTL Jan 2014 UpdateDocument37 pagesAssociated Gas Utilization Via MiniGTL Jan 2014 Updatekurtbk100% (1)
- Phed213 PrelimDocument1 pagePhed213 PrelimKaye OrtegaNo ratings yet
- GluttonyDocument2 pagesGluttonyFrezel BasiloniaNo ratings yet
- English Media (Mindmap) UnfDocument1 pageEnglish Media (Mindmap) Unfpanty sushiNo ratings yet
- 2 Studbooks in Denmark Licensed To Register Connemara PoniesDocument3 pages2 Studbooks in Denmark Licensed To Register Connemara PoniesFrankQuinnNo ratings yet
- Nathaniel HawthorneDocument41 pagesNathaniel HawthorneDương Thị Quỳnh Trang 5A-20No ratings yet
- Form 1Document2 pagesForm 1durgaprasad3004100% (1)
- Chapter 10 - Ethical Decision MakingDocument38 pagesChapter 10 - Ethical Decision MakingGraceNo ratings yet
- MythologyDocument6 pagesMythologysharlymarieNo ratings yet
- Oracle Order Backlog Management DsDocument4 pagesOracle Order Backlog Management DsSaurabh SharmaNo ratings yet
- Olukunle CVDocument2 pagesOlukunle CVSammy David Oluwafemi0% (1)
- Earth Science 5Document2 pagesEarth Science 5Sean CaloyloyNo ratings yet





























































































Download as docx, pdf, or txt
You might also like
- Crown Pallet PC 4500 Parts Catalog Maintenance Service Manual en FRDocument22 pagesCrown Pallet PC 4500 Parts Catalog Maintenance Service Manual en FRjohnathanfoster080802obr96% (27)
- Registration For ChildcareDocument2 pagesRegistration For Childcareapi-315547754No ratings yet
- Associate CalassDocument151 pagesAssociate CalassMuhammad Naveed AnjumNo ratings yet
- 12 Years A SlaveDocument2 pages12 Years A SlaveismanNo ratings yet
- Student MedicalDocument1 pageStudent MedicalbbruntNo ratings yet
- ChildenrollmentpapersDocument7 pagesChildenrollmentpapersapi-531837774No ratings yet
- Junior Tours Medical ReleaseDocument1 pageJunior Tours Medical Releaseapi-235166650No ratings yet
- Parent/Guardian Information: Continued On ReverseDocument2 pagesParent/Guardian Information: Continued On Reverseadhi eng lrtNo ratings yet
- Urgentcare FormDocument4 pagesUrgentcare Formapi-287654333No ratings yet
- GCCSACCEmergency Card InformationDocument1 pageGCCSACCEmergency Card InformationAl-juffrey Luis AmilhamjaNo ratings yet
- New Patient RegistrationDocument2 pagesNew Patient Registrationnaveenmi2100% (1)
- CDMedical AuthorizationDocument1 pageCDMedical Authorizationtrellon_devteamNo ratings yet
- Registration 2010 2011Document3 pagesRegistration 2010 2011cubanita11No ratings yet
- Teen MedicalDocument1 pageTeen MedicalJohn C StarkNo ratings yet
- Liability Release and Parental Consent FormDocument3 pagesLiability Release and Parental Consent Formapi-28674765No ratings yet
- Student Information Sheet 2Document2 pagesStudent Information Sheet 2jhon jhon millareNo ratings yet
- Enrollment PacketDocument3 pagesEnrollment Packetapi-741820810No ratings yet
- Patient Registration Form 13Document4 pagesPatient Registration Form 13windawaty humolaNo ratings yet
- General Release / Permission Form: ACTIVITIES: (Initial All That Apply)Document2 pagesGeneral Release / Permission Form: ACTIVITIES: (Initial All That Apply)Megan JonesNo ratings yet
- Clinical Health RequirementsDocument6 pagesClinical Health RequirementsbarneylovesbagelsNo ratings yet
- Pcs Emergency Permission Form - 21-22Document1 pagePcs Emergency Permission Form - 21-22api-671085061No ratings yet
- Asthma Inhaler FormDocument1 pageAsthma Inhaler Formheather579No ratings yet
- Student Enrollment FormDocument3 pagesStudent Enrollment Formapi-239237152No ratings yet
- Uprising Medical Release FormDocument1 pageUprising Medical Release Formone dollar youth ministryNo ratings yet
- Patient InformationDocument10 pagesPatient InformationFatimahNo ratings yet
- Official Medical Information and Release FormDocument2 pagesOfficial Medical Information and Release FormtheNOLAtreeNo ratings yet
- Health FormDocument2 pagesHealth Formamanda6254No ratings yet
- Brown Hearing Centers: Personal InformationDocument2 pagesBrown Hearing Centers: Personal InformationEddie TooheyNo ratings yet
- Next Gen Med ReleaseDocument2 pagesNext Gen Med ReleaserfbcgreenvilleNo ratings yet
- Af Cavemen Cheer Try-Out PacketDocument5 pagesAf Cavemen Cheer Try-Out PacketAf CheerNo ratings yet
- Student Assurance Services, Inc. P.O. Box 196 STILLWATER, MN 55082-0196Document1 pageStudent Assurance Services, Inc. P.O. Box 196 STILLWATER, MN 55082-0196Sharif M Mizanur RahmanNo ratings yet
- Dare To Dream 2011 Medical ReleaseDocument1 pageDare To Dream 2011 Medical Releaserls2orgNo ratings yet
- School Health Examination CardDocument3 pagesSchool Health Examination Cardjrose fay amatNo ratings yet
- Medical Waiver 2014-2015Document4 pagesMedical Waiver 2014-2015api-73377093No ratings yet
- Parent Permission Formed ItDocument1 pageParent Permission Formed Itannoyed4lyfeNo ratings yet
- Field Trip Permission SlipDocument1 pageField Trip Permission Slipapi-272734430No ratings yet
- Adult Health HistoryDocument1 pageAdult Health HistorySally Hansen100% (1)
- Registration FormDocument3 pagesRegistration FormcampsunshinenycNo ratings yet
- Genesis Academy Pre-K Program Registration Form: Child's InformationDocument7 pagesGenesis Academy Pre-K Program Registration Form: Child's InformationPhillip M JonesNo ratings yet
- Writable PC FormDocument1 pageWritable PC FormJulie Vyne ModalesNo ratings yet
- Enrollment PacketDocument6 pagesEnrollment Packetapi-382256148No ratings yet
- MedicalformDocument1 pageMedicalformapi-257833418No ratings yet
- Medical Form 2022-2023Document1 pageMedical Form 2022-2023Devin HouseholderNo ratings yet
- Permission FormDocument2 pagesPermission Formapi-295968636No ratings yet
- Vermara Kids Daycare Registration Form 2Document5 pagesVermara Kids Daycare Registration Form 2api-29050616No ratings yet
- 2009 Enrollment FormsDocument2 pages2009 Enrollment FormsesromseanNo ratings yet
- Registration Form DoctorDocument4 pagesRegistration Form DoctorAaditya Shyam2No ratings yet
- St. George AppDocument9 pagesSt. George AppFutureDDSNo ratings yet
- Parental Consent Forms For Minors Travelling Without ParentsDocument4 pagesParental Consent Forms For Minors Travelling Without ParentsLuckyTTinioNo ratings yet
- Student InformationDocument1 pageStudent Informationchantel_allenNo ratings yet
- Typhoid Fever: Administrative DemographicsDocument6 pagesTyphoid Fever: Administrative DemographicsMohan ChikkalaNo ratings yet
- YouthactivitiesconsentDocument1 pageYouthactivitiesconsentLaurie ThomasNo ratings yet
- Pds Medical-Cert Waiver 2023-RspcDocument1 pagePds Medical-Cert Waiver 2023-RspcRon MenesNo ratings yet
- PDS Medical-Cert Waiver 2024-RSPCDocument1 pagePDS Medical-Cert Waiver 2024-RSPCRose Andrea BergonioNo ratings yet
- Mena Bands Medical Release FormDocument1 pageMena Bands Medical Release Formapi-358909433No ratings yet
- Application For Admission - Prek & Kindergarten Program: Morning Extended Care (7:30-8:30 Am)Document4 pagesApplication For Admission - Prek & Kindergarten Program: Morning Extended Care (7:30-8:30 Am)Pedro barriaNo ratings yet
- 5.13 Field Trip FormDocument3 pages5.13 Field Trip FormLisa RossNo ratings yet
- CamperDocument1 pageCamperapi-223112910No ratings yet
- Parental Consent Form: For Youth Ministry StudentsDocument2 pagesParental Consent Form: For Youth Ministry StudentsAnonymous LYJ5Aj83cNo ratings yet
- HTCP Medical FormDocument2 pagesHTCP Medical Formapi-44699616No ratings yet
- Sifa Student Enrollment Packet Sy19 20Document5 pagesSifa Student Enrollment Packet Sy19 20Anonymous 49o5YzlNo ratings yet
- I-C-E in Case of Emergency: Your Essential Medical JournalFrom EverandI-C-E in Case of Emergency: Your Essential Medical JournalNo ratings yet
- Information Pack For Schools 2011-WebDocument35 pagesInformation Pack For Schools 2011-Webapi-144496227No ratings yet
- Camp Permission FormDocument1 pageCamp Permission Formapi-144496227No ratings yet
- ST Francis CollegeDocument1 pageST Francis Collegeapi-144496227No ratings yet
- Sleepover 2015Document1 pageSleepover 2015api-144496227No ratings yet
- Pcka Term 1 Timetable 2013Document1 pagePcka Term 1 Timetable 2013api-144496227No ratings yet
- Term 1 2013Document1 pageTerm 1 2013api-144496227No ratings yet
- Organization and Management LAS - Week 2Document4 pagesOrganization and Management LAS - Week 2Louie MunsayacNo ratings yet
- Exhibition Brochure-Embalsamada-Con-Picante (Embalmed With Spice)Document6 pagesExhibition Brochure-Embalsamada-Con-Picante (Embalmed With Spice)Isa SonNo ratings yet
- Our 16 Fundamental TruthsDocument10 pagesOur 16 Fundamental TruthsChristine Joy Verde SantiagoNo ratings yet
- OASGFO 2022 058 Requests For The Participation of Learners and Teachers in Extra CurricularDocument2 pagesOASGFO 2022 058 Requests For The Participation of Learners and Teachers in Extra CurricularRocky Nathaniel SalesNo ratings yet
- The Gender of The GiftDocument3 pagesThe Gender of The GiftMarcia Sandoval EsparzaNo ratings yet
- What Is Project Management Functions - These Big 8! - TompsDocument6 pagesWhat Is Project Management Functions - These Big 8! - TompsKavi MukilanNo ratings yet
- Foi Mtcu-100025 Bargaining Expenses Thu Aug 26 2010 08-26-27.142-1Document5 pagesFoi Mtcu-100025 Bargaining Expenses Thu Aug 26 2010 08-26-27.142-1Rob HorganNo ratings yet
- The Church House of God Fr. Tadros MalatyDocument354 pagesThe Church House of God Fr. Tadros MalatyIsa Almisry100% (3)
- Project Name: "New Arrivals": FNA Test PlanDocument6 pagesProject Name: "New Arrivals": FNA Test PlanNusrat HasanNo ratings yet
- Introduction and Preface To PFRS and Conceptual Framework: Theory of Accounts Preweek DiscussionDocument20 pagesIntroduction and Preface To PFRS and Conceptual Framework: Theory of Accounts Preweek DiscussionLeisleiRagoNo ratings yet
- Senoir Project-IrelandDocument12 pagesSenoir Project-Irelandapi-317313323No ratings yet
- Oracle Database 11 Product Family: An Oracle White Paper June 2012Document19 pagesOracle Database 11 Product Family: An Oracle White Paper June 2012Aliasger BharmalNo ratings yet
- MGT610 MIDTERM SOLVED MCQS by JUNAIDDocument33 pagesMGT610 MIDTERM SOLVED MCQS by JUNAIDtalha8389711100% (1)
- Vastu For House - Home Vastu Test - Vastu Shastra Score For House - Vastu House Facing - Vastu Shastra Home PDFDocument3 pagesVastu For House - Home Vastu Test - Vastu Shastra Score For House - Vastu House Facing - Vastu Shastra Home PDFSelvaraj VillyNo ratings yet
- Associated Gas Utilization Via MiniGTL Jan 2014 UpdateDocument37 pagesAssociated Gas Utilization Via MiniGTL Jan 2014 Updatekurtbk100% (1)
- Phed213 PrelimDocument1 pagePhed213 PrelimKaye OrtegaNo ratings yet
- GluttonyDocument2 pagesGluttonyFrezel BasiloniaNo ratings yet
- English Media (Mindmap) UnfDocument1 pageEnglish Media (Mindmap) Unfpanty sushiNo ratings yet
- 2 Studbooks in Denmark Licensed To Register Connemara PoniesDocument3 pages2 Studbooks in Denmark Licensed To Register Connemara PoniesFrankQuinnNo ratings yet
- Nathaniel HawthorneDocument41 pagesNathaniel HawthorneDương Thị Quỳnh Trang 5A-20No ratings yet
- Form 1Document2 pagesForm 1durgaprasad3004100% (1)
- Chapter 10 - Ethical Decision MakingDocument38 pagesChapter 10 - Ethical Decision MakingGraceNo ratings yet
- MythologyDocument6 pagesMythologysharlymarieNo ratings yet
- Oracle Order Backlog Management DsDocument4 pagesOracle Order Backlog Management DsSaurabh SharmaNo ratings yet
- Olukunle CVDocument2 pagesOlukunle CVSammy David Oluwafemi0% (1)
- Earth Science 5Document2 pagesEarth Science 5Sean CaloyloyNo ratings yet