Download as docx, pdf, or txt
You might also like
- Rock Steady: Healing Vertigo or Tinnitus With NeuroplasticityFrom EverandRock Steady: Healing Vertigo or Tinnitus With NeuroplasticityRating: 5 out of 5 stars5/5 (4)
- Handbook of Self and Identity - Second Edition - Ch. 4 Pp. 69-104 38 Pages PDFDocument38 pagesHandbook of Self and Identity - Second Edition - Ch. 4 Pp. 69-104 38 Pages PDFBarthajuliaNo ratings yet
- Joyce Travelbee: Human-To-Human Relationship ModelDocument39 pagesJoyce Travelbee: Human-To-Human Relationship Modelxilina Bacasnot100% (3)
- Personal Nursing PhilosophyDocument5 pagesPersonal Nursing PhilosophyLaura Sotomayor100% (2)
- Drug Abuse - Causes and ResultsDocument4 pagesDrug Abuse - Causes and ResultsJohn OsborneNo ratings yet
- Stephen Wolinsky - Dark Side ODocument193 pagesStephen Wolinsky - Dark Side Oginigarden100% (2)
- Silence and Politeness in Intercultural Communication in Uni SeminarsDocument25 pagesSilence and Politeness in Intercultural Communication in Uni SeminarsCynthia LohNo ratings yet
- Compare and ContrastDocument4 pagesCompare and ContrastKathy LeNo ratings yet
- Mental Health Nursing-Hospice PaperDocument7 pagesMental Health Nursing-Hospice PaperKaylee BlankenshipNo ratings yet
- Formal Group Paper 1Document13 pagesFormal Group Paper 1api-340642770No ratings yet
- With References EachDocument5 pagesWith References EachYsabel Francesca AbadNo ratings yet
- Final End of Life Care-FinalDocument8 pagesFinal End of Life Care-FinalYounas BhattiNo ratings yet
- The Role of Spirituality in Health Care: C M. P, MD, MsDocument6 pagesThe Role of Spirituality in Health Care: C M. P, MD, MselvineNo ratings yet
- Health Promotion PaperDocument9 pagesHealth Promotion Paperapi-448502475No ratings yet
- Palliative Care PDFDocument14 pagesPalliative Care PDFNoshin MalekiNo ratings yet
- Hsci 301 PhilessayDocument11 pagesHsci 301 Philessayapi-241136824No ratings yet
- Into the Heart of Health: Reaching Your Health Threshold, an Unshakeable Balance in Mind, Body, and EmotionsFrom EverandInto the Heart of Health: Reaching Your Health Threshold, an Unshakeable Balance in Mind, Body, and EmotionsNo ratings yet
- Kaua'i Hospice & Palliative Care ExperienceDocument7 pagesKaua'i Hospice & Palliative Care ExperienceLlewelyn AgpaoaNo ratings yet
- Palliative Care NotesDocument29 pagesPalliative Care NotesCnette S. Lumbo100% (1)
- Hospice Care sc2Document5 pagesHospice Care sc2Aziil LiizaNo ratings yet
- Service Learning Reflection PaperDocument3 pagesService Learning Reflection Paperapi-297614673No ratings yet
- Living at the End of Life: A Hospice Nurse Addresses the Most Common QuestionsFrom EverandLiving at the End of Life: A Hospice Nurse Addresses the Most Common QuestionsRating: 4 out of 5 stars4/5 (4)
- Poc Enabling Compassionate Care Hospital Settings Apr09Document16 pagesPoc Enabling Compassionate Care Hospital Settings Apr09Cristian Meza ValladaresNo ratings yet
- 3 Death and DyingDocument34 pages3 Death and Dyingikram ullah khanNo ratings yet
- Drama and Movement TherapyDocument10 pagesDrama and Movement TherapyduramemoriaNo ratings yet
- Taranslate PaliatifDocument5 pagesTaranslate PaliatiffitriNo ratings yet
- Keperawatan Paliatif1 NewestDocument36 pagesKeperawatan Paliatif1 Newestmuhammad_abdullah_68No ratings yet
- Joyce TravelbeeDocument32 pagesJoyce TravelbeeJana ObligadoNo ratings yet
- TFN Week 13 14Document43 pagesTFN Week 13 14mccaberto1061cabNo ratings yet
- Promosi Kesehatan Dan Pencegahan PenyakiDocument27 pagesPromosi Kesehatan Dan Pencegahan PenyakiAngga PutraNo ratings yet
- Semester 3 AssignmentDocument10 pagesSemester 3 Assignmentapi-283957252No ratings yet
- Dysfunctional Grief TheoryDocument4 pagesDysfunctional Grief TheoryScribdTranslationsNo ratings yet
- Report On The Theory of Dysfunctional GriefDocument11 pagesReport On The Theory of Dysfunctional GriefScribdTranslationsNo ratings yet
- The Body Deva: Working with the Spiritual Consciousness of the BodyFrom EverandThe Body Deva: Working with the Spiritual Consciousness of the BodyRating: 5 out of 5 stars5/5 (2)
- Journal of Surgical NurseDocument8 pagesJournal of Surgical NurseWahyu WeraNo ratings yet
- Palliative RehabilitationDocument43 pagesPalliative Rehabilitationrlinao100% (2)
- wk14PR 1.editedDocument8 pageswk14PR 1.editedOscarNo ratings yet
- Treating - Eating - Disorder 2019Document146 pagesTreating - Eating - Disorder 2019Cualit14100% (3)
- HOSPICE: A DIFFERENT TYPE OF HOPE: Criteria For Choosing Your Hospice Team SoonerFrom EverandHOSPICE: A DIFFERENT TYPE OF HOPE: Criteria For Choosing Your Hospice Team SoonerNo ratings yet
- Personal Philosphy PaperDocument9 pagesPersonal Philosphy Paperapi-353789245No ratings yet
- Final Draft Teen HospiceDocument10 pagesFinal Draft Teen Hospiceapi-311443082No ratings yet
- Intuitive Medicine Summit 2022 Day 3Document6 pagesIntuitive Medicine Summit 2022 Day 3Paul Ioan PopescuNo ratings yet
- Case Presentation: Presented By: BSN 141 / Group 161 - ADocument33 pagesCase Presentation: Presented By: BSN 141 / Group 161 - Akince0015No ratings yet
- The Role of the Spiritual Caregiver to the Terminally Ill PatientsFrom EverandThe Role of the Spiritual Caregiver to the Terminally Ill PatientsRating: 5 out of 5 stars5/5 (1)
- 2325 6134 1 SMDocument12 pages2325 6134 1 SMmuh. syahril ramadhanNo ratings yet
- Care of The Patient and His FamilyDocument2 pagesCare of The Patient and His FamilyNikey LimNo ratings yet
- Case StudyDocument62 pagesCase StudyIyalisaiVijay0% (1)
- Paley Philosophy PaperDocument5 pagesPaley Philosophy Paperapi-356236058No ratings yet
- Mourning Protocol Details and The Cognitive Behavior Therapy Applicability AuthorsDocument13 pagesMourning Protocol Details and The Cognitive Behavior Therapy Applicability AuthorsGraziele ZwielewskiNo ratings yet
- Hospice and PallativeDocument38 pagesHospice and PallativeVhe Pacatang100% (1)
- ElectiveDocument35 pagesElectivedeeNo ratings yet
- Elective NSG Palliative PrinciplesDocument17 pagesElective NSG Palliative PrinciplesdariosumandeNo ratings yet
- Eassy Humanities ContributeDocument9 pagesEassy Humanities Contributeoumou80No ratings yet
- Nurs 3021 Reflective JournalDocument6 pagesNurs 3021 Reflective Journalapi-487456788No ratings yet
- Vulnerable PopulationsDocument5 pagesVulnerable Populationsapi-250046004100% (1)
- Taranslate PaliatifDocument5 pagesTaranslate PaliatiffitriNo ratings yet
- Lesson 12Document39 pagesLesson 12Rizalyn Padua ReyNo ratings yet
- Nu518personal Philosophy E-PortDocument7 pagesNu518personal Philosophy E-Portapi-380371704No ratings yet
- Healing, Spirituality and Integrative Medicine: David M. Steinhorn, Jana Din, Angela JohnsonDocument11 pagesHealing, Spirituality and Integrative Medicine: David M. Steinhorn, Jana Din, Angela JohnsonTibor GalacziNo ratings yet
- Home Care and Family PhysicianDocument25 pagesHome Care and Family PhysiciandesypermitasariNo ratings yet
- Nikkithao ResumeDocument2 pagesNikkithao Resumeapi-285132682No ratings yet
- Filipino Cultural Interview PaperDocument13 pagesFilipino Cultural Interview Paperapi-285132682100% (2)
- Mental Health - PT Case StudyDocument10 pagesMental Health - PT Case Studyapi-285132682No ratings yet
- Nikki - Sentinel Event PaperDocument18 pagesNikki - Sentinel Event Paperapi-285132682100% (1)
- Field Observation Paper - American Indian Pow WowDocument7 pagesField Observation Paper - American Indian Pow Wowapi-285132682No ratings yet
- Global Health Paper Final DraftDocument22 pagesGlobal Health Paper Final Draftapi-285132682No ratings yet
- Updated Basic Competencies As of Sept 9, 2019 PDFDocument318 pagesUpdated Basic Competencies As of Sept 9, 2019 PDFraquel100% (4)
- Week 3-Leadership and Management StylesDocument29 pagesWeek 3-Leadership and Management Stylesfionatex35No ratings yet
- Syllabus: Introduction To Principle of CreativityDocument1 pageSyllabus: Introduction To Principle of CreativityShahla AliNo ratings yet
- Etextbook 978 0205985807 CognitionDocument61 pagesEtextbook 978 0205985807 Cognitionbenjamin.vega423100% (53)
- Jalowiec Coping Scale OverviewDocument3 pagesJalowiec Coping Scale OverviewShandy100% (3)
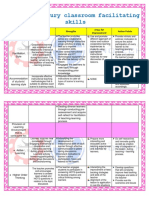
- Assignment No. 2 - My 21st Century Classroom Facilitating SkillsDocument4 pagesAssignment No. 2 - My 21st Century Classroom Facilitating SkillsKaren Delos Santos Toledo100% (2)
- WK01. S2 - WMC201Document30 pagesWK01. S2 - WMC201tr.hjieu0708No ratings yet
- Exploring Leadership - Autor BoldenDocument27 pagesExploring Leadership - Autor BoldenZoila Castro UriolNo ratings yet
- Mastering The Art of QuestioningDocument2 pagesMastering The Art of QuestioningYeshua YeshaNo ratings yet
- Influence of Student's STEM Self-Efficacy On STEM and Physics Career ChoiceDocument3 pagesInfluence of Student's STEM Self-Efficacy On STEM and Physics Career ChoiceEazel Donn VillamaterNo ratings yet
- Com325 Week1 AssignDocument5 pagesCom325 Week1 Assignjoseph mainaNo ratings yet
- Presentation1 MC ELT 1Document61 pagesPresentation1 MC ELT 1Ana Kassandra Lazaro HernandezNo ratings yet
- Notes in ACC148 P1docxDocument4 pagesNotes in ACC148 P1docxShaina Laila OlpindoNo ratings yet
- Sculpture Lesson PlanDocument4 pagesSculpture Lesson PlanPaulina WilkersonNo ratings yet
- National Curriculum Framework NCF (2005) OnDocument33 pagesNational Curriculum Framework NCF (2005) OnLeo SaimNo ratings yet
- UNIT 4 Human Growth and Development PowerpointDocument19 pagesUNIT 4 Human Growth and Development PowerpointMaria Judith Peña JulianesNo ratings yet
- Conaghan P Et Al - Feedback To Feedforward - Notfall Rettungsmed 2009Document4 pagesConaghan P Et Al - Feedback To Feedforward - Notfall Rettungsmed 2009Orlando EsparzaNo ratings yet
- FIELD STUDY 4 (Interview)Document8 pagesFIELD STUDY 4 (Interview)Julius BaldivinoNo ratings yet
- Consumer Behavior of Gym GoersDocument4 pagesConsumer Behavior of Gym GoersBadel Singh100% (1)
- Background and ContextDocument2 pagesBackground and ContextNatasa TucevNo ratings yet
- Brazil Business CultureDocument17 pagesBrazil Business CultureIrma Aprilia SalehNo ratings yet
- Schizophrenia UndifferentiatedDocument64 pagesSchizophrenia UndifferentiatedJen GarzoNo ratings yet
- BBS Do's and Don'tsDocument9 pagesBBS Do's and Don'tsparag14No ratings yet
- AttitudeDocument12 pagesAttitudeAlex PavelNo ratings yet
- ANECDOTAL RECORD & Observation Rport 2015-16Document3 pagesANECDOTAL RECORD & Observation Rport 2015-16maria luzNo ratings yet
- When It's Time To Go A Look at ContractDocument2 pagesWhen It's Time To Go A Look at ContractRaghu NayakNo ratings yet