Download as pdf or txt
You might also like
- MSI Health Card Renewal FormDocument1 pageMSI Health Card Renewal Formdohudohu2100% (1)
- Notes: Face AmountDocument4 pagesNotes: Face Amountqris24No ratings yet
- Appletree NP Forms FillableDocument2 pagesAppletree NP Forms FillableFabian SvrNo ratings yet
- New Patient Information Form PrintableDocument3 pagesNew Patient Information Form PrintableXyzNo ratings yet
- Go BIG For Parkinson Registration FormDocument2 pagesGo BIG For Parkinson Registration Formrickberry55No ratings yet
- Prenatal Req PDFDocument4 pagesPrenatal Req PDFVARDHINI N V RAMA JOGARAONo ratings yet
- Axa Mansard Health Corporate Form - Nathan Ayomide OriaifoDocument1 pageAxa Mansard Health Corporate Form - Nathan Ayomide OriaifoIsiNo ratings yet
- Appletree NP Fillable FormDocument2 pagesAppletree NP Fillable Form349154906No ratings yet
- 2023 PROJECT COOL BREEZE ApplicationDocument1 page2023 PROJECT COOL BREEZE ApplicationLive 5 News100% (3)
- Request Letter 2Document1 pageRequest Letter 2Rose Ann R. AbenidoNo ratings yet
- Request Letter 2 PDFDocument1 pageRequest Letter 2 PDFAnna Rose C. AlcazarenNo ratings yet
- HTCP Medical FormDocument2 pagesHTCP Medical Formapi-44699616No ratings yet
- Summercamp Regform 2015Document2 pagesSummercamp Regform 2015api-275753240No ratings yet
- History Form For AdultsDocument9 pagesHistory Form For AdultsFazal HaqueNo ratings yet
- HEALTH CARE QUESTIONNAIRE FAUSTINA NYARKO FINAL-mergedDocument8 pagesHEALTH CARE QUESTIONNAIRE FAUSTINA NYARKO FINAL-mergedEkow HaganNo ratings yet
- Rady Childrens HospitalDocument6 pagesRady Childrens HospitalTom HeavenNo ratings yet
- Urgentcare FormDocument4 pagesUrgentcare Formapi-287654333No ratings yet
- FF Knowles Membership ApplicationDocument2 pagesFF Knowles Membership Applicationtreedown3No ratings yet
- Employee Data (Application) FormDocument2 pagesEmployee Data (Application) FormGlaneisia MitchellNo ratings yet
- Chiropractic Application Form: Section A: Contact InformationDocument6 pagesChiropractic Application Form: Section A: Contact InformationAmanakeNo ratings yet
- Name of Health Care Provider / Plan / Other/ Myself Address: (Please Fill in Below)Document1 pageName of Health Care Provider / Plan / Other/ Myself Address: (Please Fill in Below)Jennifer walNo ratings yet
- Background Investigation Form: Please Fill All Information in PRINTED. If Item Is Not Applicable Put "N/A"Document5 pagesBackground Investigation Form: Please Fill All Information in PRINTED. If Item Is Not Applicable Put "N/A"Jason MendarosNo ratings yet
- Referral FormDocument2 pagesReferral FormRANDY BAOGBOG100% (1)
- Employment / Job Application: Page 1 of 4Document4 pagesEmployment / Job Application: Page 1 of 4api-545870588No ratings yet
- 4.2022 SCSC Membership FormDocument2 pages4.2022 SCSC Membership FormLerbet SisonNo ratings yet
- Teens Encounter Christ Medical Form: DD/ MM/ YyDocument3 pagesTeens Encounter Christ Medical Form: DD/ MM/ YyshawnbranchNo ratings yet
- NMTC Application Form FinalDocument5 pagesNMTC Application Form FinalicttumainiNo ratings yet
- COMPANY NAME: - Regular Salaried Employees - 18 To 65 Years OldDocument1 pageCOMPANY NAME: - Regular Salaried Employees - 18 To 65 Years OldCart Sunrise AguillonNo ratings yet
- Membership FormDocument2 pagesMembership FormpaglaummisNo ratings yet
- Teen MedicalDocument1 pageTeen MedicalJohn C StarkNo ratings yet
- Undergraduate Application Form EditedDocument2 pagesUndergraduate Application Form EditedDickson Samson AlexNo ratings yet
- Patient InformationDocument10 pagesPatient InformationFatimahNo ratings yet
- CamperDocument1 pageCamperapi-223112910No ratings yet
- Patient Registration Form 29Document8 pagesPatient Registration Form 29Cahayastore CahayastoreNo ratings yet
- Patient Registration Form 13Document4 pagesPatient Registration Form 13windawaty humolaNo ratings yet
- 14) ELIB-Female CI-Claim FormDocument7 pages14) ELIB-Female CI-Claim Formbibianna93No ratings yet
- In Kind Donation FormDocument1 pageIn Kind Donation Formgenesisworldmission100% (4)
- Austin Divorce Attorney - Client Info - Law Office of Jay D. SmithDocument7 pagesAustin Divorce Attorney - Client Info - Law Office of Jay D. Smithas_jaydsmithNo ratings yet
- RegularvolunteerDocument2 pagesRegularvolunteerapi-242884241No ratings yet
- PETS Nail Trim FormDocument1 pagePETS Nail Trim Formamy welchNo ratings yet
- Applicationform Mortgage LoanDocument7 pagesApplicationform Mortgage LoanBijendra Singh BishtNo ratings yet
- ACE Medical Center - Shareholders Personal Data Sheet-IRO HEIDIE OMBAODocument1 pageACE Medical Center - Shareholders Personal Data Sheet-IRO HEIDIE OMBAOSam AlianzaNo ratings yet
- Auction Item Donation FormDocument1 pageAuction Item Donation FormgenesisworldmissionNo ratings yet
- Confidential Patient Information: Authorization and AssignmentDocument10 pagesConfidential Patient Information: Authorization and AssignmenteryxspNo ratings yet
- Self Pay Information FormDocument1 pageSelf Pay Information FormPerformax Physical TherapyNo ratings yet
- 2016 Associate Membership ApplicationDocument2 pages2016 Associate Membership ApplicationNJ Food CouncilNo ratings yet
- Taska Mami Adik ReportDocument3 pagesTaska Mami Adik ReportDhiya' QawiemNo ratings yet
- Know Your Customer (KYC) Application FormDocument3 pagesKnow Your Customer (KYC) Application Formbioduny2kNo ratings yet
- Adult NP Ppwrork KCPGDocument16 pagesAdult NP Ppwrork KCPGMary GreerNo ratings yet
- VAW Intake Form 2023Document4 pagesVAW Intake Form 2023Arnold GuintoNo ratings yet
- Skin Tbmantouxapp05 PDFDocument1 pageSkin Tbmantouxapp05 PDFprateek chaudharyNo ratings yet
- Mantoux Tuberculin Skin Test Record Form: Patient InformationDocument1 pageMantoux Tuberculin Skin Test Record Form: Patient InformationreactanttNo ratings yet
- Symmetry Data Sheet 12 12Document1 pageSymmetry Data Sheet 12 12Argel Hanzon NietesNo ratings yet
- GAL Application - Become A GAL in SCDocument5 pagesGAL Application - Become A GAL in SCWylde FaerieNo ratings yet
- NITC Membership 2010Document1 pageNITC Membership 2010North Iowa SpinNo ratings yet
- Membership Renewal FormDocument3 pagesMembership Renewal Formdalitsanibanda4No ratings yet
- CUMC Medical Consent 2010-2011Document1 pageCUMC Medical Consent 2010-2011Matthew Dunn-RankinNo ratings yet
- Appllication Form For Ccreditation-FormDocument1 pageAppllication Form For Ccreditation-FormChrome JerichoNo ratings yet
- CTBHI 2014 Belkin Golf TournamentDocument4 pagesCTBHI 2014 Belkin Golf TournamentCTBHINo ratings yet
- CTBHI - Application For FundraiserDocument1 pageCTBHI - Application For FundraiserCTBHINo ratings yet
- Shop For A CauseDocument1 pageShop For A CauseCTBHINo ratings yet
- Belkin GolfTournament2011wDocument2 pagesBelkin GolfTournament2011wCTBHINo ratings yet
- Liu ActaF 2012Document6 pagesLiu ActaF 2012CTBHINo ratings yet
- 2012 Golf SaveTheDateDocument1 page2012 Golf SaveTheDateCTBHINo ratings yet
- FINAL 2012 Golf Application (4 Pages Stacked) - r1Document4 pagesFINAL 2012 Golf Application (4 Pages Stacked) - r1CTBHINo ratings yet
- Monday, September 12, 2011: Howard H. Belkin Memorial Golf TournamentDocument4 pagesMonday, September 12, 2011: Howard H. Belkin Memorial Golf TournamentCTBHINo ratings yet
- STYD Flyer 2011 - 11-6Document1 pageSTYD Flyer 2011 - 11-6CTBHINo ratings yet
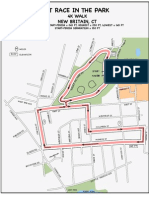
- Race in Park 4K MapDocument1 pageRace in Park 4K MapCTBHINo ratings yet
- Race in Park 5K MapDocument1 pageRace in Park 5K MapCTBHINo ratings yet
- CT BHI JazzerciseFundraiser.1Document1 pageCT BHI JazzerciseFundraiser.1CTBHINo ratings yet
- BTag DirectionsDocument1 pageBTag DirectionsCTBHINo ratings yet
- Nondiscrimination PolicyDocument1 pageNondiscrimination PolicyCTBHINo ratings yet
- 2012 CTBHISponsorformDocument2 pages2012 CTBHISponsorformCTBHINo ratings yet