Download as pdf or txt
You might also like
- Ethics Handbook For Energy Healers - Book ReviewDocument3 pagesEthics Handbook For Energy Healers - Book ReviewCambiador de MundoNo ratings yet
- AECOM 14942-C Construction Management Call in RFP Sample Port Authority-7Document226 pagesAECOM 14942-C Construction Management Call in RFP Sample Port Authority-7mish750012100% (1)
- 07 - Hit Readiness AssessmentDocument13 pages07 - Hit Readiness AssessmentAbidi HichemNo ratings yet
- MMDS (Medical Morrtality Data System)Document1,241 pagesMMDS (Medical Morrtality Data System)Bhella GuntoroNo ratings yet
- Paradigma Baru Pengelolaan Keuangan Rumah SakitDocument17 pagesParadigma Baru Pengelolaan Keuangan Rumah SakitQaisha ArbeyNo ratings yet
- Closed Medical Record ReviewDocument6 pagesClosed Medical Record ReviewMuzna Iqbal50% (2)
- Vibrational HealingDocument23 pagesVibrational Healingyasin11100% (1)
- EmrDocument8 pagesEmrAnnisa DarmawangsaNo ratings yet
- Dampak Penumpukan Berkas Rekam Medis Di RuangfilingDocument12 pagesDampak Penumpukan Berkas Rekam Medis Di RuangfilingKintan IntanNo ratings yet
- Asesmen Kesiapan Implementasi RME - Handout-1Document36 pagesAsesmen Kesiapan Implementasi RME - Handout-1Bening Ananing100% (1)
- LEMBAR JAWABAN KKPMT 1 - 10 (External Causes (01 November 2021) - (1) - 3Document4 pagesLEMBAR JAWABAN KKPMT 1 - 10 (External Causes (01 November 2021) - (1) - 3Dyah Citra100% (1)
- Analisis Desain Formulir Ringkasan Masuk & Keluar PDFDocument13 pagesAnalisis Desain Formulir Ringkasan Masuk & Keluar PDFNova Dwi Pawestri II0% (1)
- Soal Latihan Tindakan Icd9 CMDocument3 pagesSoal Latihan Tindakan Icd9 CMArmann100% (1)
- Form Registrasi Kanker RSDocument10 pagesForm Registrasi Kanker RSAnonymous 8UVWsANo ratings yet
- Aspek Keamanan BerkasDocument7 pagesAspek Keamanan BerkassivaNo ratings yet
- BS Rekam Medis Dan KerahasiaanDocument93 pagesBS Rekam Medis Dan KerahasiaanCeceNo ratings yet
- Kodifikasi Latihan Chapter XVDocument3 pagesKodifikasi Latihan Chapter XVZidaneNo ratings yet
- Kelmpok 3 Jawaban Soal 1 SD 10Document50 pagesKelmpok 3 Jawaban Soal 1 SD 10tri lestariNo ratings yet
- KKPMT EndokrinDocument6 pagesKKPMT EndokrinDyah CitraNo ratings yet
- Pedoman Retensi Rekam Medis (Dr. Rano Indradi, M.kes)Document20 pagesPedoman Retensi Rekam Medis (Dr. Rano Indradi, M.kes)febi novrizalNo ratings yet
- TM3 - P17410211020 - Nisa Amanda Diva P - 1A - TUGAS KODEFIKASI 3Document4 pagesTM3 - P17410211020 - Nisa Amanda Diva P - 1A - TUGAS KODEFIKASI 3NisaadivaNo ratings yet
- Kode Kombinasi & Kode GandaDocument15 pagesKode Kombinasi & Kode GandaJuwitahasugianNo ratings yet
- KKPMT Cidera Dan KeracunanDocument4 pagesKKPMT Cidera Dan KeracunanDyah CitraNo ratings yet
- Tugas Praktikum Kodefikasi PenyakitDocument6 pagesTugas Praktikum Kodefikasi Penyakitdewi candra agustinNo ratings yet
- Peranan Kompetensi PMIK Di PuskesmasDocument101 pagesPeranan Kompetensi PMIK Di Puskesmasahmad 85No ratings yet
- Soal External Cause 1-8Document7 pagesSoal External Cause 1-8Widiati AfNo ratings yet
- Latihan Soal Chapter XVDocument15 pagesLatihan Soal Chapter XVDEWI WULANDARI KONTJE100% (1)
- Analisis Kuantitatif Kelengkapan Dokumen Rekam Medis Pasien RawatDocument10 pagesAnalisis Kuantitatif Kelengkapan Dokumen Rekam Medis Pasien RawatLahasang JieNo ratings yet
- KKPMT UcodDocument3 pagesKKPMT UcodDyah CitraNo ratings yet
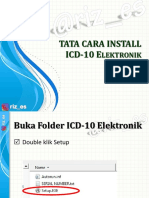
- TATA CARA INSTALL ICD-10 ElektronikDocument6 pagesTATA CARA INSTALL ICD-10 ElektronikPuskesmas Cijagra BaruNo ratings yet
- External CauseDocument49 pagesExternal Causemyrea projectNo ratings yet
- Uswatun Hasanah-195037-2a Rmik (KKPMT)Document4 pagesUswatun Hasanah-195037-2a Rmik (KKPMT)Uswatun HasanahNo ratings yet
- Tinjauan Penerapan Sistem Rekam Medis Elektronik Rawat Jalan Di Rumah Sakit Pelabuhan JakartaDocument5 pagesTinjauan Penerapan Sistem Rekam Medis Elektronik Rawat Jalan Di Rumah Sakit Pelabuhan JakartaAndi GumelarNo ratings yet
- Hris HospitalDocument14 pagesHris HospitalzebanawabNo ratings yet
- 3b-195055-Dyah Citra Resmi (KKPMT Kulit)Document3 pages3b-195055-Dyah Citra Resmi (KKPMT Kulit)Dyah CitraNo ratings yet
- 2B Dyah Citra Resmi 195055 (KKPMT Sistem Saraf)Document5 pages2B Dyah Citra Resmi 195055 (KKPMT Sistem Saraf)Dyah CitraNo ratings yet
- Kode Pintar ICD 9 CMDocument1 pageKode Pintar ICD 9 CMjack poetraNo ratings yet
- Rumus Hitung Pengembalian BRMDocument12 pagesRumus Hitung Pengembalian BRM'Laras' Vera GracilliaNo ratings yet
- 2B-195055-Dyah Citra Resmi-Gangguan Mental Dan PerilakuDocument4 pages2B-195055-Dyah Citra Resmi-Gangguan Mental Dan PerilakuDyah CitraNo ratings yet
- Nama: Dyah Citra Resmi Nim: 195055 Kelas: 3B RMIKDocument3 pagesNama: Dyah Citra Resmi Nim: 195055 Kelas: 3B RMIKDyah CitraNo ratings yet
- (KKPMT 2a) TM 5. Terminologi Medis SalcernaDocument16 pages(KKPMT 2a) TM 5. Terminologi Medis SalcernaFigaNo ratings yet
- Latihan Soal Koding PerinatalDocument9 pagesLatihan Soal Koding PerinatalikaNo ratings yet
- KODEDocument14 pagesKODEDeeLha RamadhanaNo ratings yet
- Terminologi Medis Terkait Congenital Malformations, Deformations and Chromosal AbnormalitiesDocument5 pagesTerminologi Medis Terkait Congenital Malformations, Deformations and Chromosal AbnormalitiesKartika Iva RiyantiNo ratings yet
- Discharge Summary ContohDocument2 pagesDischarge Summary ContohRemoBagasNo ratings yet
- Kel7 Unit3 BHS InggrisDocument8 pagesKel7 Unit3 BHS Inggrisrafiqa gustinaNo ratings yet
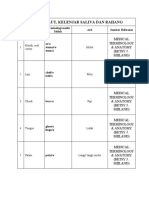
- Rongga Mulut, Kelenjar Saliva Dan Rahang: No Istilah Terminologi Medis Istilah Arti Sumber ReferensiDocument30 pagesRongga Mulut, Kelenjar Saliva Dan Rahang: No Istilah Terminologi Medis Istilah Arti Sumber ReferensiAlfi Melinda FNo ratings yet
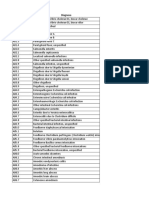
- Kode Icd 10Document536 pagesKode Icd 10AkbarisArisNo ratings yet
- Form Registrasi Kanker RSDocument10 pagesForm Registrasi Kanker RSRika WandiNo ratings yet
- Paper Consultation & ConsolidationDocument11 pagesPaper Consultation & ConsolidationSindy RosdianasNo ratings yet
- Bank Nomor Rekam MedisDocument310 pagesBank Nomor Rekam Medisnurcasan75% (4)
- CodingDocument110 pagesCodingBudi Yunanto100% (1)
- Faktor-Faktor Yang Mempengaruhi Kelengkapan Rekam Medis Rawat Inap Dengan Menggunakan Diagram Fishbone Di Rumah Sakit Pertamina Jaya Tahun 2017Document6 pagesFaktor-Faktor Yang Mempengaruhi Kelengkapan Rekam Medis Rawat Inap Dengan Menggunakan Diagram Fishbone Di Rumah Sakit Pertamina Jaya Tahun 2017WIdyaHumairaNo ratings yet
- 2.1.1.8 - Terminologi, Penamaan & Klasifikasi Neoplasma 2014Document28 pages2.1.1.8 - Terminologi, Penamaan & Klasifikasi Neoplasma 2014death_professorNo ratings yet
- 7-200 Sampe 7-209Document9 pages7-200 Sampe 7-209yulfiqiNo ratings yet
- Jurnal INFOKES Volume 7 Nomor 1 Juni 2023 ISSN. 2597-7776Document11 pagesJurnal INFOKES Volume 7 Nomor 1 Juni 2023 ISSN. 2597-7776raizap712100% (1)
- Evaluasi Kinerja Petugas Rekam Medis Berdasarkan MDocument5 pagesEvaluasi Kinerja Petugas Rekam Medis Berdasarkan MAmelia P. UsmanNo ratings yet
- Evaluasi Kelengkapan Rekam Medis Berdasa 1093e2ccDocument9 pagesEvaluasi Kelengkapan Rekam Medis Berdasa 1093e2ccOctavia MaltaNo ratings yet
- MATERI - PMK 21-2020 Menuju RME Terintegrasi - HandoutDocument22 pagesMATERI - PMK 21-2020 Menuju RME Terintegrasi - HandoutDony KristianNo ratings yet
- Tugas Coding Aulia Zajila Rmik 4aDocument2 pagesTugas Coding Aulia Zajila Rmik 4aAulia ZajilaNo ratings yet
- Handbook For Doctor On Cause of Death CertificationDocument32 pagesHandbook For Doctor On Cause of Death CertificationFarinaDwinandaFaisalNo ratings yet
- A The Health RecordDocument6 pagesA The Health Recordbusinge innocentNo ratings yet
- Hospital Information SystemDocument17 pagesHospital Information Systemdeepimalar28No ratings yet
- A Practical Guide To Caring For CaregiversDocument9 pagesA Practical Guide To Caring For CaregiversMarc Ernest BialaNo ratings yet
- Intuitive Medicine Summit 2022 Day 2Document8 pagesIntuitive Medicine Summit 2022 Day 2Paul Ioan PopescuNo ratings yet
- Samantha Stinsonresume 2Document2 pagesSamantha Stinsonresume 2samstinsonNo ratings yet
- CredentialingDocument35 pagesCredentialingAli AhmadNo ratings yet
- PSC Operations ManualDocument18 pagesPSC Operations ManualJohn TanhuecoNo ratings yet
- Violence Against Physicians in Jordan 2021Document14 pagesViolence Against Physicians in Jordan 2021magicuddinNo ratings yet
- LEGAL MEDICINE DigestDocument16 pagesLEGAL MEDICINE Digestesmeralda de guzmanNo ratings yet
- Kim 2015Document10 pagesKim 2015cekNo ratings yet
- Professional Ethics Roleand ImportanceDocument8 pagesProfessional Ethics Roleand ImportancePrecious KadiriNo ratings yet
- Registration Instructions For FreshmenDocument5 pagesRegistration Instructions For FreshmenQuicelyn OconNo ratings yet
- Perlindungan Hukum Bagi Profesi Perawat Terhadap Pelaksanaan Praktik KeperawatanDocument5 pagesPerlindungan Hukum Bagi Profesi Perawat Terhadap Pelaksanaan Praktik KeperawatanALWIN WinNo ratings yet
- Erin Kerbaugh's Career PlanDocument2 pagesErin Kerbaugh's Career Planca8erin15No ratings yet
- Ebook Handbook of Medicine in Psychiatry 3Rd Edition Manu Online PDF All ChapterDocument69 pagesEbook Handbook of Medicine in Psychiatry 3Rd Edition Manu Online PDF All Chaptershirley.richards902100% (5)
- 100 Years of Excellance For Saint Louis University School of Medicine Department of Internal MedicineDocument4 pages100 Years of Excellance For Saint Louis University School of Medicine Department of Internal MedicineSlusom WebNo ratings yet
- AAOHNS MembershipApplicationDocument4 pagesAAOHNS MembershipApplicationAnonymous AuJncFVWvNo ratings yet
- Health Care Laws P.S.D.A.: Submitted To: Mr. Kush Kalra Asst. Professor, Law Delhi Metropolitan EducationDocument10 pagesHealth Care Laws P.S.D.A.: Submitted To: Mr. Kush Kalra Asst. Professor, Law Delhi Metropolitan EducationAnuj Singh RaghuvanshiNo ratings yet
- The Cancer SolutionDocument227 pagesThe Cancer Solutionragod2100% (2)
- MaqasidDocument5 pagesMaqasidDidi FirdausNo ratings yet
- AdverDocument13 pagesAdverHelen Meriz SagunNo ratings yet
- 1st PT - MAPEH 10 SY 2022-2023Document5 pages1st PT - MAPEH 10 SY 2022-2023Norralyn NarioNo ratings yet
- Medical ATO Ukraine, April, 2015Document27 pagesMedical ATO Ukraine, April, 2015Patrick Chellew100% (1)
- GUIDELINES FOR REGULATION OF HERBS in UGANDA PDFDocument29 pagesGUIDELINES FOR REGULATION OF HERBS in UGANDA PDFShaima El Amrousy80% (5)
- SAQ123 NursesUserGuide V6Document30 pagesSAQ123 NursesUserGuide V6LisaBrook100% (1)
- HomeGymWod - 100+ Bodyweight Workouts Guide v1.7Document29 pagesHomeGymWod - 100+ Bodyweight Workouts Guide v1.7Hichem MustaphaNo ratings yet
- Guidelines On Aesthetic Medical Practice - 110613Document47 pagesGuidelines On Aesthetic Medical Practice - 110613windows3123No ratings yet
- IsbarDocument3 pagesIsbarapi-384653068No ratings yet
- Role of Psychiatric NursingDocument3 pagesRole of Psychiatric NursingOmega Shane LechonsitoNo ratings yet