Download as docx, pdf, or txt
You might also like
- Photon Benefits 2022 (August)Document7 pagesPhoton Benefits 2022 (August)sojithesouljaNo ratings yet
- Corporate Classic PDFDocument4 pagesCorporate Classic PDFironhide404No ratings yet
- Vision Care Plan The Choice ProgramDocument2 pagesVision Care Plan The Choice Programapi-296522671No ratings yet
- US Apple Vision Plan Overview JAN152021 enDocument1 pageUS Apple Vision Plan Overview JAN152021 enCT NguonNo ratings yet
- 2016 FEP BlueVisionDocument2 pages2016 FEP BlueVisionGopal Gopinath100% (1)
- Vision Highlight Sheet For Bugatchi Group, IncDocument3 pagesVision Highlight Sheet For Bugatchi Group, Incdayron ruizNo ratings yet
- Bupa GoldExtras NSW ACT 0415Document3 pagesBupa GoldExtras NSW ACT 0415Laura Leander WildeNo ratings yet
- Bec Plan WordDocument11 pagesBec Plan Wordprint1156No ratings yet
- Stud-E PresentationDocument13 pagesStud-E Presentationapi-242374745No ratings yet
- Bupa ClassicExtras NSW ACT 0415Document3 pagesBupa ClassicExtras NSW ACT 0415Investor ProtegeNo ratings yet
- Flex Benefits July 2016Document4 pagesFlex Benefits July 2016Daniyal AzmatNo ratings yet
- VisionDocument5 pagesVisionCarl WiltNo ratings yet
- Price Compare 2010Document2 pagesPrice Compare 2010Marissa ClarkNo ratings yet
- PSU - Grad Students - VW Enh FF IX - 2022Document3 pagesPSU - Grad Students - VW Enh FF IX - 2022enzoNo ratings yet
- An Extras Cover For A Healthier LifestyleDocument6 pagesAn Extras Cover For A Healthier LifestylealterchicNo ratings yet
- EyeMed SummaryDocument2 pagesEyeMed Summaryyoungstarbuck3606No ratings yet
- 2022 Steven Charles BAG - CODocument4 pages2022 Steven Charles BAG - COAlejuanchis Kamacho GarciaNo ratings yet
- Brochure PDF MANHATTHAN LIFEDocument2 pagesBrochure PDF MANHATTHAN LIFEEmanuel ChirinosNo ratings yet
- 2021 - Life, Dental, Vision PacketDocument12 pages2021 - Life, Dental, Vision PacketEberNo ratings yet
- Weekly Sale October 1-8Document3 pagesWeekly Sale October 1-8katyucya7685No ratings yet
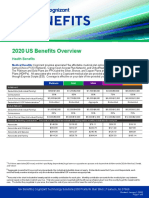
- 2020 US Benefits OverviewDocument5 pages2020 US Benefits OverviewrdmNo ratings yet
- Buy Stop and Grow Biting Deterant 7 ML Online at Chemist Warehouse®Document1 pageBuy Stop and Grow Biting Deterant 7 ML Online at Chemist Warehouse®Shiv BhattaraiNo ratings yet
- Your VSP Vision Benefits Summary: Frequency Copay Description BenefitDocument1 pageYour VSP Vision Benefits Summary: Frequency Copay Description BenefitVictor LepriNo ratings yet
- Benefit Overview 2019 For WebsiteDocument13 pagesBenefit Overview 2019 For Websiteapi-373197589No ratings yet
- 2020 Rate Sheet - DiversifiedDocument2 pages2020 Rate Sheet - Diversifiedrobin floydNo ratings yet
- OE Powerpoint PresentationDocument35 pagesOE Powerpoint PresentationAnonymous ibpKT07GNo ratings yet
- Weekly Sale February 10-14Document2 pagesWeekly Sale February 10-14Katrina NovikovaNo ratings yet
- Benefits Highlights 2018Document5 pagesBenefits Highlights 2018Marcus CosmeNo ratings yet
- Screenshot 2023-09-14 at 7.52.06 PMDocument1 pageScreenshot 2023-09-14 at 7.52.06 PMsophie.shlimonNo ratings yet
- SeKON Employee Benefits Summary 2016Document3 pagesSeKON Employee Benefits Summary 2016Ali HajassdolahNo ratings yet
- 2010 2011KaiserBenefitSummaryDocument1 page2010 2011KaiserBenefitSummaryJim LombardoNo ratings yet
- Options Plus VSPDocument1 pageOptions Plus VSPGowell SupportNo ratings yet
- Program Planning PilatesDocument3 pagesProgram Planning Pilatesapi-3550687960% (1)
- Budget ProjectDocument12 pagesBudget Projectapi-353143592No ratings yet
- Guardian - VSP Choice PPO Plan Summary 2022Document3 pagesGuardian - VSP Choice PPO Plan Summary 2022Jessi ChallagullaNo ratings yet
- Spirit 2023 Benefits - FT - Pilots - Day - One - BenefitsDocument4 pagesSpirit 2023 Benefits - FT - Pilots - Day - One - BenefitsFelipe MontanoNo ratings yet
- Critical Issues: Spring One of A Kind ShowDocument6 pagesCritical Issues: Spring One of A Kind ShowAmie NguyenNo ratings yet
- Your Customized Benefits Plan at HCL America IncDocument2 pagesYour Customized Benefits Plan at HCL America IncShiv RanjanNo ratings yet
- New Hire Benefits Summary: Medical Plan OptionsDocument3 pagesNew Hire Benefits Summary: Medical Plan OptionsRavi Prakash MayreddyNo ratings yet
- 2022 1027 Ahs SD 1058-1 BroDocument8 pages2022 1027 Ahs SD 1058-1 BroFernanda VargasNo ratings yet
- Glamador Teeth Whitening Kit, Reusable Teeth Whitening Set, 12 Teeth Whitening Gel, 3 Soothing Gel, 1 LED Blue Light Bleaching LDocument1 pageGlamador Teeth Whitening Kit, Reusable Teeth Whitening Set, 12 Teeth Whitening Gel, 3 Soothing Gel, 1 LED Blue Light Bleaching LMarah BakelehNo ratings yet
- COBRA Monthly Premium Rate Chart: Effective January 1 - December 31, 2014Document1 pageCOBRA Monthly Premium Rate Chart: Effective January 1 - December 31, 2014stevenzliNo ratings yet
- ABS TRA CT: To UndeDocument18 pagesABS TRA CT: To UndeJoshua FlowersNo ratings yet
- Life Is Better in Focus.: Consumers'Document2 pagesLife Is Better in Focus.: Consumers'Sakuryu TsukinoNo ratings yet
- Chamber Rate SheetDocument1 pageChamber Rate SheetBshale1No ratings yet
- Program Planning Worksheet: Masen SpeirDocument3 pagesProgram Planning Worksheet: Masen Speirapi-355068796No ratings yet
- A Hat For Pollution ControlDocument2 pagesA Hat For Pollution ControlDevesh Kumar SinghalNo ratings yet
- Sunscreen QuestionsDocument7 pagesSunscreen QuestionsUmme Laila JatoiNo ratings yet
- Aetna Vision CoreDocument2 pagesAetna Vision CoreBeau PeskaNo ratings yet
- JACAM Benefit OverviewDocument7 pagesJACAM Benefit OverviewStephenDohertyNo ratings yet
- 2024 Health Plan Costs English NonHawaiiDocument6 pages2024 Health Plan Costs English NonHawaiinouskarmaxyNo ratings yet
- 2017 DgldmetDocument5 pages2017 DgldmetLucas FrançaNo ratings yet
- Dental Benefit DetailsDocument3 pagesDental Benefit DetailsFernanda VargasNo ratings yet
- Rite Aid, Wags, CVS 2-19Document4 pagesRite Aid, Wags, CVS 2-19SistersShoppingNo ratings yet
- Benefit at A GlanceDocument2 pagesBenefit at A GlanceShiv ChauhanNo ratings yet
- Opsm OfferDocument1 pageOpsm Offerhetalgajjar41No ratings yet
- GROUP 4 - MM 3-3 - PRODUCT MANAGEMENT - With CommentDocument15 pagesGROUP 4 - MM 3-3 - PRODUCT MANAGEMENT - With CommentJoe ArmentaNo ratings yet
- Greenology: Giving Back and Growing TogetherDocument7 pagesGreenology: Giving Back and Growing TogethergreeNology MagazineNo ratings yet
- The Natural Acne Remedy Handbook: 50 Ways to treat acne using natural remediesFrom EverandThe Natural Acne Remedy Handbook: 50 Ways to treat acne using natural remediesNo ratings yet