
Materi OSC Damon
Materi OSC Damon
You might also like
- ALHS 1090 Final Exam WorksheetDocument18 pagesALHS 1090 Final Exam WorksheetCesilia Martinez Castro0% (1)
- Beggs' Technique (Stage I, Ii & Iii)Document25 pagesBeggs' Technique (Stage I, Ii & Iii)Dr. Suhasis Mondal96% (25)
- Special TestsDocument34 pagesSpecial TestsFitri Isnaini100% (1)
- Ortho BasicsDocument52 pagesOrtho Basicschellemi100% (1)
- The "Ballista Spring" System For Impacted Teeth: Genevu. SwitzerlandDocument9 pagesThe "Ballista Spring" System For Impacted Teeth: Genevu. Switzerlandapi-26468957100% (1)
- Appendix: Motor Control Training Intervention ManualDocument32 pagesAppendix: Motor Control Training Intervention Manualgonchodiaz1703No ratings yet
- James Ray Dixon - Amphibians and Reptiles of Texas - With Keys, Taxonomic Synopses, Bibliography, and Distribution Maps (W.L. Moody, JR., Natural History Series, No. 8.) (2000) PDFDocument430 pagesJames Ray Dixon - Amphibians and Reptiles of Texas - With Keys, Taxonomic Synopses, Bibliography, and Distribution Maps (W.L. Moody, JR., Natural History Series, No. 8.) (2000) PDFjohannesNo ratings yet
- Teach Me AnatomyDocument17 pagesTeach Me AnatomyMar Kristian Vero Lumen100% (1)
- Hanau's Quint Rudolph. L. Hanau ProposedDocument49 pagesHanau's Quint Rudolph. L. Hanau ProposedArunNo ratings yet
- Orthodontic BracketsDocument9 pagesOrthodontic Bracketsdevi kanthNo ratings yet
- Attachments Used For OrthodonticsDocument56 pagesAttachments Used For OrthodonticsScribdTranslationsNo ratings yet
- FridayDocument55 pagesFridayJim HungNo ratings yet
- Removable Orthodontic ApplianceDocument7 pagesRemovable Orthodontic ApplianceAhmed AymanNo ratings yet
- Attachments Used in Orthodontics First SemesterDocument13 pagesAttachments Used in Orthodontics First SemesterScribdTranslationsNo ratings yet
- RetainerDocument74 pagesRetainersonal agarwalNo ratings yet
- Fixed Functional AppliancesDocument82 pagesFixed Functional Appliancesdisha 146jandialNo ratings yet
- Role of Stress Breakers in Removable Partial DentureDocument66 pagesRole of Stress Breakers in Removable Partial DentureNimra WaniNo ratings yet
- Design Consideration in Reducing Stress in RPDDocument11 pagesDesign Consideration in Reducing Stress in RPDAnkit NarolaNo ratings yet
- Eyelets Vs Arch Bar 2017Document12 pagesEyelets Vs Arch Bar 20176hd6mnrzw2No ratings yet
- Maxillary Major ConnectorsDocument20 pagesMaxillary Major ConnectorsRohan GroverNo ratings yet
- Space Closure Using Frictionless MechanicsDocument11 pagesSpace Closure Using Frictionless MechanicsLisbethNo ratings yet
- Herbst ApplianceDocument36 pagesHerbst ApplianceSakthi Priya100% (5)
- Assignment: 1-What Is The Rationale Behind The Mesial Rest Concept in Distal Extension Removable Partial Denture Cases ?Document7 pagesAssignment: 1-What Is The Rationale Behind The Mesial Rest Concept in Distal Extension Removable Partial Denture Cases ?احمد القحطانيNo ratings yet
- Hybrid Functional Appliance / Orthodontic Courses by Indian Dental AcademyDocument127 pagesHybrid Functional Appliance / Orthodontic Courses by Indian Dental Academyindian dental academy100% (2)
- Cross Bit TXDocument47 pagesCross Bit TXYusra ShaukatNo ratings yet
- Attachment5th ClassDocument10 pagesAttachment5th ClasswxmdkhbyvkNo ratings yet
- Sue OrtoDocument24 pagesSue OrtoInas MellanisaNo ratings yet
- 113 217 1 PB PDFDocument6 pages113 217 1 PB PDFdup11No ratings yet
- Principles and Planning of RPDDocument26 pagesPrinciples and Planning of RPDمحمد عبدالعالم البدويNo ratings yet
- The Swing Lock Denture: 1-Too Few Remaining Teeth For A Conventional DesignDocument9 pagesThe Swing Lock Denture: 1-Too Few Remaining Teeth For A Conventional DesignEsmail AhmedNo ratings yet
- Selection of Attachment PresentationDocument44 pagesSelection of Attachment PresentationIbrahim Ahmed Dahab100% (1)
- Fixed Appliance Design, Function and ConstructionDocument14 pagesFixed Appliance Design, Function and Constructionsp vumbunu100% (1)
- Iring Techniques: Sidra Tul MuntahaDocument36 pagesIring Techniques: Sidra Tul Muntahamiss0meNo ratings yet
- Reverse Facial Mask: Prepared by Shafa Fwad FaeeqDocument5 pagesReverse Facial Mask: Prepared by Shafa Fwad Faeeqمحمد العراقيNo ratings yet
- Carriere Motion Appliance Brochure InternationalDocument8 pagesCarriere Motion Appliance Brochure InternationalOrtho OrganizersNo ratings yet
- 11 Retention of Maxillofacial Prosthesis Fayad PDFDocument7 pages11 Retention of Maxillofacial Prosthesis Fayad PDFMostafa Fayad50% (2)
- Orthodontics Ii (Lecture Note)Document29 pagesOrthodontics Ii (Lecture Note)Rufai HarunaNo ratings yet
- Post Graduate Student: Dr. RahultiwariDocument158 pagesPost Graduate Student: Dr. RahultiwariVivek Sunil EdayathNo ratings yet
- Mathods of Gaining SpaceDocument22 pagesMathods of Gaining SpaceAamir FaizNo ratings yet
- Stage I and Stage Ii-Begg'S ApplianceDocument50 pagesStage I and Stage Ii-Begg'S ApplianceNaziya ShaikNo ratings yet
- Partial Denture 4Document11 pagesPartial Denture 4ShamsNo ratings yet
- MatricesDocument47 pagesMatricesAsmita VermaNo ratings yet
- Refernce 18Document11 pagesRefernce 18Ali ZubiediNo ratings yet
- Attachments in OverdentureDocument5 pagesAttachments in OverdentureQueen LiveNo ratings yet
- Stress BreakerDocument7 pagesStress BreakerEshan Verma33% (3)
- A Palatal Expansion Appliance For Non Compliance Therapy JCO ONLINE - Com Journal of Clinical OrthodonticsDocument6 pagesA Palatal Expansion Appliance For Non Compliance Therapy JCO ONLINE - Com Journal of Clinical OrthodonticsLeticia Sarzuri HonorioNo ratings yet
- Space Closure: K .Lavanya IiyrpgDocument162 pagesSpace Closure: K .Lavanya IiyrpgNeelima ChandranNo ratings yet
- Occlusal Considerations in Implant: Technology of Dental ImplantDocument16 pagesOcclusal Considerations in Implant: Technology of Dental ImplantDania TahboubNo ratings yet
- Molar DistalizationDocument27 pagesMolar DistalizationNeeraj AroraNo ratings yet
- OrthodonticsDocument123 pagesOrthodonticsAyesha Anwar90% (10)
- Removable Partial Prosthesis TrialDocument10 pagesRemovable Partial Prosthesis TrialScribdTranslationsNo ratings yet
- Retention and Relapse in Orthodontics: Submitted By: Ekta ChaudharyDocument60 pagesRetention and Relapse in Orthodontics: Submitted By: Ekta ChaudharyMuftihat IsrarNo ratings yet
- Retention of Removable Orthodontic AppliancesDocument18 pagesRetention of Removable Orthodontic AppliancesFahd Yusuf KariapperNo ratings yet
- Maxillary Major ConnectorsDocument27 pagesMaxillary Major ConnectorsNikhil GuptaNo ratings yet
- Hybridhyrax 180211141507 PDFDocument42 pagesHybridhyrax 180211141507 PDFNgo Viet ThanhNo ratings yet
- Loops and RetractionDocument24 pagesLoops and RetractionYuvashreeNo ratings yet
- Design Considerations in RPD For Control of StressDocument7 pagesDesign Considerations in RPD For Control of StressSahana RangarajanNo ratings yet
- Complications and Maintenance of Dental ImplantDocument5 pagesComplications and Maintenance of Dental ImplantAkshay GajakoshNo ratings yet
- Lec 8 3rd Class PDFDocument4 pagesLec 8 3rd Class PDFBrandon AviciiNo ratings yet
- Removable Appliances 2Document136 pagesRemovable Appliances 2Mohsin Habib100% (1)
- Screenshot 2024-01-28 at 6.50.46 PMDocument14 pagesScreenshot 2024-01-28 at 6.50.46 PMmohamed samirNo ratings yet
- Stress Breakers: DR Mayur HegdeDocument35 pagesStress Breakers: DR Mayur HegdeSan0% (1)
- ImplantDocument9 pagesImplantKhaled Abo ZaidNo ratings yet
- Mplication of Cost Effectiveness in The Management of Patients at High CV-riskDocument43 pagesMplication of Cost Effectiveness in The Management of Patients at High CV-riskfika_khayanNo ratings yet
- Ek - Kes Pembiayaan RonnieDocument28 pagesEk - Kes Pembiayaan Ronniefika_khayanNo ratings yet
- He Economics of Exclusive Breastfeedin: Ronnie Rivany Pusat Kajian Ekonomi Kesehatan FkmuiDocument31 pagesHe Economics of Exclusive Breastfeedin: Ronnie Rivany Pusat Kajian Ekonomi Kesehatan Fkmuifika_khayanNo ratings yet
- Demand For Health CareDocument12 pagesDemand For Health Carefika_khayanNo ratings yet
- Periodontal Update 3: Klik DisiniDocument2 pagesPeriodontal Update 3: Klik Disinifika_khayanNo ratings yet
- Bagi Hari Sama Rata (FINAL)Document14 pagesBagi Hari Sama Rata (FINAL)fika_khayanNo ratings yet
- Chapman Points Table - Anatomical Terms of Location - Human Anatomy PDFDocument7 pagesChapman Points Table - Anatomical Terms of Location - Human Anatomy PDFSusan Rashid0% (1)
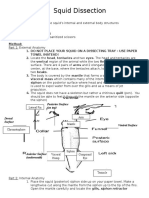
- Squid DissectionDocument3 pagesSquid Dissectionapi-297841438100% (1)
- HASPI Using Anatomical LanguageDocument6 pagesHASPI Using Anatomical LanguageAnirudh AnandNo ratings yet
- 11-C1 BrowliftDocument34 pages11-C1 BrowliftShaun Tan100% (1)
- The Masculoskeletal System & Tissue MechanicsDocument29 pagesThe Masculoskeletal System & Tissue MechanicsEdara Rajesh KumarNo ratings yet
- Health Science Tool Kit Text BookDocument278 pagesHealth Science Tool Kit Text BookAidan Glasby100% (1)
- European GuidelinesDocument88 pagesEuropean GuidelinesrochimNo ratings yet
- Contouring in Breast Cancer Current Practice and Future DirectionsDocument67 pagesContouring in Breast Cancer Current Practice and Future DirectionsRodrigo DíazNo ratings yet
- CPT PDFDocument43 pagesCPT PDFEbony Crawford100% (1)
- tmp6662 TMPDocument140 pagestmp6662 TMPFrontiersNo ratings yet
- The Normal Anterior Inferior Cerebellar ArteryDocument19 pagesThe Normal Anterior Inferior Cerebellar Artery16fernandoNo ratings yet
- WB CHPT 1 11 12 14 16 17Document2 pagesWB CHPT 1 11 12 14 16 17api-264668182No ratings yet
- PHYSIOTOXI Part1Document101 pagesPHYSIOTOXI Part1Angelyn RodulloNo ratings yet
- Rood S ApproachDocument33 pagesRood S Approachmedway physio teamNo ratings yet
- University of Rajshahi Syllabus BSC HonoursDocument21 pagesUniversity of Rajshahi Syllabus BSC HonoursProf. Dr. M. KhalequzzamanNo ratings yet
- 11rhinoplasty SurgicalAnatomyDocument49 pages11rhinoplasty SurgicalAnatomySanooj SeyedNo ratings yet
- Two New Genera & Three New Species of ThylacinidaeDocument18 pagesTwo New Genera & Three New Species of ThylacinidaeSeidskrattiNo ratings yet
- Primary Malignant Tumors of The Spine: Gregory S. Mcloughlin Daniel M. Sciubba Jean-Paul WolinskyDocument12 pagesPrimary Malignant Tumors of The Spine: Gregory S. Mcloughlin Daniel M. Sciubba Jean-Paul Wolinskymetasoniko81No ratings yet
- GROUP2 Surface Landmarks. Body Habitus. Anatomical Terms.Document27 pagesGROUP2 Surface Landmarks. Body Habitus. Anatomical Terms.Windelle RecolcolinNo ratings yet
- Full Ebook of Workbook For Diagnostic Medical Sonography The Vascular Systems 3Rd Edition Ann Marie Kupinski Online PDF All ChapterDocument69 pagesFull Ebook of Workbook For Diagnostic Medical Sonography The Vascular Systems 3Rd Edition Ann Marie Kupinski Online PDF All Chapterahmedhtrianz100% (10)
- Buccal Fat Pad Review PDFDocument4 pagesBuccal Fat Pad Review PDFNavatha MorthaNo ratings yet
- 1.1 Introduction To Human Anatomy - 2018-2019 PDFDocument11 pages1.1 Introduction To Human Anatomy - 2018-2019 PDFسيف محمود شاكر حسنNo ratings yet
- Ankle: FracturesDocument87 pagesAnkle: FracturesrifkialbanaNo ratings yet




























































































Download as doc, pdf, or txt
You might also like
- ALHS 1090 Final Exam WorksheetDocument18 pagesALHS 1090 Final Exam WorksheetCesilia Martinez Castro0% (1)
- Beggs' Technique (Stage I, Ii & Iii)Document25 pagesBeggs' Technique (Stage I, Ii & Iii)Dr. Suhasis Mondal96% (25)
- Special TestsDocument34 pagesSpecial TestsFitri Isnaini100% (1)
- Ortho BasicsDocument52 pagesOrtho Basicschellemi100% (1)
- The "Ballista Spring" System For Impacted Teeth: Genevu. SwitzerlandDocument9 pagesThe "Ballista Spring" System For Impacted Teeth: Genevu. Switzerlandapi-26468957100% (1)
- Appendix: Motor Control Training Intervention ManualDocument32 pagesAppendix: Motor Control Training Intervention Manualgonchodiaz1703No ratings yet
- James Ray Dixon - Amphibians and Reptiles of Texas - With Keys, Taxonomic Synopses, Bibliography, and Distribution Maps (W.L. Moody, JR., Natural History Series, No. 8.) (2000) PDFDocument430 pagesJames Ray Dixon - Amphibians and Reptiles of Texas - With Keys, Taxonomic Synopses, Bibliography, and Distribution Maps (W.L. Moody, JR., Natural History Series, No. 8.) (2000) PDFjohannesNo ratings yet
- Teach Me AnatomyDocument17 pagesTeach Me AnatomyMar Kristian Vero Lumen100% (1)
- Hanau's Quint Rudolph. L. Hanau ProposedDocument49 pagesHanau's Quint Rudolph. L. Hanau ProposedArunNo ratings yet
- Orthodontic BracketsDocument9 pagesOrthodontic Bracketsdevi kanthNo ratings yet
- Attachments Used For OrthodonticsDocument56 pagesAttachments Used For OrthodonticsScribdTranslationsNo ratings yet
- FridayDocument55 pagesFridayJim HungNo ratings yet
- Removable Orthodontic ApplianceDocument7 pagesRemovable Orthodontic ApplianceAhmed AymanNo ratings yet
- Attachments Used in Orthodontics First SemesterDocument13 pagesAttachments Used in Orthodontics First SemesterScribdTranslationsNo ratings yet
- RetainerDocument74 pagesRetainersonal agarwalNo ratings yet
- Fixed Functional AppliancesDocument82 pagesFixed Functional Appliancesdisha 146jandialNo ratings yet
- Role of Stress Breakers in Removable Partial DentureDocument66 pagesRole of Stress Breakers in Removable Partial DentureNimra WaniNo ratings yet
- Design Consideration in Reducing Stress in RPDDocument11 pagesDesign Consideration in Reducing Stress in RPDAnkit NarolaNo ratings yet
- Eyelets Vs Arch Bar 2017Document12 pagesEyelets Vs Arch Bar 20176hd6mnrzw2No ratings yet
- Maxillary Major ConnectorsDocument20 pagesMaxillary Major ConnectorsRohan GroverNo ratings yet
- Space Closure Using Frictionless MechanicsDocument11 pagesSpace Closure Using Frictionless MechanicsLisbethNo ratings yet
- Herbst ApplianceDocument36 pagesHerbst ApplianceSakthi Priya100% (5)
- Assignment: 1-What Is The Rationale Behind The Mesial Rest Concept in Distal Extension Removable Partial Denture Cases ?Document7 pagesAssignment: 1-What Is The Rationale Behind The Mesial Rest Concept in Distal Extension Removable Partial Denture Cases ?احمد القحطانيNo ratings yet
- Hybrid Functional Appliance / Orthodontic Courses by Indian Dental AcademyDocument127 pagesHybrid Functional Appliance / Orthodontic Courses by Indian Dental Academyindian dental academy100% (2)
- Cross Bit TXDocument47 pagesCross Bit TXYusra ShaukatNo ratings yet
- Attachment5th ClassDocument10 pagesAttachment5th ClasswxmdkhbyvkNo ratings yet
- Sue OrtoDocument24 pagesSue OrtoInas MellanisaNo ratings yet
- 113 217 1 PB PDFDocument6 pages113 217 1 PB PDFdup11No ratings yet
- Principles and Planning of RPDDocument26 pagesPrinciples and Planning of RPDمحمد عبدالعالم البدويNo ratings yet
- The Swing Lock Denture: 1-Too Few Remaining Teeth For A Conventional DesignDocument9 pagesThe Swing Lock Denture: 1-Too Few Remaining Teeth For A Conventional DesignEsmail AhmedNo ratings yet
- Selection of Attachment PresentationDocument44 pagesSelection of Attachment PresentationIbrahim Ahmed Dahab100% (1)
- Fixed Appliance Design, Function and ConstructionDocument14 pagesFixed Appliance Design, Function and Constructionsp vumbunu100% (1)
- Iring Techniques: Sidra Tul MuntahaDocument36 pagesIring Techniques: Sidra Tul Muntahamiss0meNo ratings yet
- Reverse Facial Mask: Prepared by Shafa Fwad FaeeqDocument5 pagesReverse Facial Mask: Prepared by Shafa Fwad Faeeqمحمد العراقيNo ratings yet
- Carriere Motion Appliance Brochure InternationalDocument8 pagesCarriere Motion Appliance Brochure InternationalOrtho OrganizersNo ratings yet
- 11 Retention of Maxillofacial Prosthesis Fayad PDFDocument7 pages11 Retention of Maxillofacial Prosthesis Fayad PDFMostafa Fayad50% (2)
- Orthodontics Ii (Lecture Note)Document29 pagesOrthodontics Ii (Lecture Note)Rufai HarunaNo ratings yet
- Post Graduate Student: Dr. RahultiwariDocument158 pagesPost Graduate Student: Dr. RahultiwariVivek Sunil EdayathNo ratings yet
- Mathods of Gaining SpaceDocument22 pagesMathods of Gaining SpaceAamir FaizNo ratings yet
- Stage I and Stage Ii-Begg'S ApplianceDocument50 pagesStage I and Stage Ii-Begg'S ApplianceNaziya ShaikNo ratings yet
- Partial Denture 4Document11 pagesPartial Denture 4ShamsNo ratings yet
- MatricesDocument47 pagesMatricesAsmita VermaNo ratings yet
- Refernce 18Document11 pagesRefernce 18Ali ZubiediNo ratings yet
- Attachments in OverdentureDocument5 pagesAttachments in OverdentureQueen LiveNo ratings yet
- Stress BreakerDocument7 pagesStress BreakerEshan Verma33% (3)
- A Palatal Expansion Appliance For Non Compliance Therapy JCO ONLINE - Com Journal of Clinical OrthodonticsDocument6 pagesA Palatal Expansion Appliance For Non Compliance Therapy JCO ONLINE - Com Journal of Clinical OrthodonticsLeticia Sarzuri HonorioNo ratings yet
- Space Closure: K .Lavanya IiyrpgDocument162 pagesSpace Closure: K .Lavanya IiyrpgNeelima ChandranNo ratings yet
- Occlusal Considerations in Implant: Technology of Dental ImplantDocument16 pagesOcclusal Considerations in Implant: Technology of Dental ImplantDania TahboubNo ratings yet
- Molar DistalizationDocument27 pagesMolar DistalizationNeeraj AroraNo ratings yet
- OrthodonticsDocument123 pagesOrthodonticsAyesha Anwar90% (10)
- Removable Partial Prosthesis TrialDocument10 pagesRemovable Partial Prosthesis TrialScribdTranslationsNo ratings yet
- Retention and Relapse in Orthodontics: Submitted By: Ekta ChaudharyDocument60 pagesRetention and Relapse in Orthodontics: Submitted By: Ekta ChaudharyMuftihat IsrarNo ratings yet
- Retention of Removable Orthodontic AppliancesDocument18 pagesRetention of Removable Orthodontic AppliancesFahd Yusuf KariapperNo ratings yet
- Maxillary Major ConnectorsDocument27 pagesMaxillary Major ConnectorsNikhil GuptaNo ratings yet
- Hybridhyrax 180211141507 PDFDocument42 pagesHybridhyrax 180211141507 PDFNgo Viet ThanhNo ratings yet
- Loops and RetractionDocument24 pagesLoops and RetractionYuvashreeNo ratings yet
- Design Considerations in RPD For Control of StressDocument7 pagesDesign Considerations in RPD For Control of StressSahana RangarajanNo ratings yet
- Complications and Maintenance of Dental ImplantDocument5 pagesComplications and Maintenance of Dental ImplantAkshay GajakoshNo ratings yet
- Lec 8 3rd Class PDFDocument4 pagesLec 8 3rd Class PDFBrandon AviciiNo ratings yet
- Removable Appliances 2Document136 pagesRemovable Appliances 2Mohsin Habib100% (1)
- Screenshot 2024-01-28 at 6.50.46 PMDocument14 pagesScreenshot 2024-01-28 at 6.50.46 PMmohamed samirNo ratings yet
- Stress Breakers: DR Mayur HegdeDocument35 pagesStress Breakers: DR Mayur HegdeSan0% (1)
- ImplantDocument9 pagesImplantKhaled Abo ZaidNo ratings yet
- Mplication of Cost Effectiveness in The Management of Patients at High CV-riskDocument43 pagesMplication of Cost Effectiveness in The Management of Patients at High CV-riskfika_khayanNo ratings yet
- Ek - Kes Pembiayaan RonnieDocument28 pagesEk - Kes Pembiayaan Ronniefika_khayanNo ratings yet
- He Economics of Exclusive Breastfeedin: Ronnie Rivany Pusat Kajian Ekonomi Kesehatan FkmuiDocument31 pagesHe Economics of Exclusive Breastfeedin: Ronnie Rivany Pusat Kajian Ekonomi Kesehatan Fkmuifika_khayanNo ratings yet
- Demand For Health CareDocument12 pagesDemand For Health Carefika_khayanNo ratings yet
- Periodontal Update 3: Klik DisiniDocument2 pagesPeriodontal Update 3: Klik Disinifika_khayanNo ratings yet
- Bagi Hari Sama Rata (FINAL)Document14 pagesBagi Hari Sama Rata (FINAL)fika_khayanNo ratings yet
- Chapman Points Table - Anatomical Terms of Location - Human Anatomy PDFDocument7 pagesChapman Points Table - Anatomical Terms of Location - Human Anatomy PDFSusan Rashid0% (1)
- Squid DissectionDocument3 pagesSquid Dissectionapi-297841438100% (1)
- HASPI Using Anatomical LanguageDocument6 pagesHASPI Using Anatomical LanguageAnirudh AnandNo ratings yet
- 11-C1 BrowliftDocument34 pages11-C1 BrowliftShaun Tan100% (1)
- The Masculoskeletal System & Tissue MechanicsDocument29 pagesThe Masculoskeletal System & Tissue MechanicsEdara Rajesh KumarNo ratings yet
- Health Science Tool Kit Text BookDocument278 pagesHealth Science Tool Kit Text BookAidan Glasby100% (1)
- European GuidelinesDocument88 pagesEuropean GuidelinesrochimNo ratings yet
- Contouring in Breast Cancer Current Practice and Future DirectionsDocument67 pagesContouring in Breast Cancer Current Practice and Future DirectionsRodrigo DíazNo ratings yet
- CPT PDFDocument43 pagesCPT PDFEbony Crawford100% (1)
- tmp6662 TMPDocument140 pagestmp6662 TMPFrontiersNo ratings yet
- The Normal Anterior Inferior Cerebellar ArteryDocument19 pagesThe Normal Anterior Inferior Cerebellar Artery16fernandoNo ratings yet
- WB CHPT 1 11 12 14 16 17Document2 pagesWB CHPT 1 11 12 14 16 17api-264668182No ratings yet
- PHYSIOTOXI Part1Document101 pagesPHYSIOTOXI Part1Angelyn RodulloNo ratings yet
- Rood S ApproachDocument33 pagesRood S Approachmedway physio teamNo ratings yet
- University of Rajshahi Syllabus BSC HonoursDocument21 pagesUniversity of Rajshahi Syllabus BSC HonoursProf. Dr. M. KhalequzzamanNo ratings yet
- 11rhinoplasty SurgicalAnatomyDocument49 pages11rhinoplasty SurgicalAnatomySanooj SeyedNo ratings yet
- Two New Genera & Three New Species of ThylacinidaeDocument18 pagesTwo New Genera & Three New Species of ThylacinidaeSeidskrattiNo ratings yet
- Primary Malignant Tumors of The Spine: Gregory S. Mcloughlin Daniel M. Sciubba Jean-Paul WolinskyDocument12 pagesPrimary Malignant Tumors of The Spine: Gregory S. Mcloughlin Daniel M. Sciubba Jean-Paul Wolinskymetasoniko81No ratings yet
- GROUP2 Surface Landmarks. Body Habitus. Anatomical Terms.Document27 pagesGROUP2 Surface Landmarks. Body Habitus. Anatomical Terms.Windelle RecolcolinNo ratings yet
- Full Ebook of Workbook For Diagnostic Medical Sonography The Vascular Systems 3Rd Edition Ann Marie Kupinski Online PDF All ChapterDocument69 pagesFull Ebook of Workbook For Diagnostic Medical Sonography The Vascular Systems 3Rd Edition Ann Marie Kupinski Online PDF All Chapterahmedhtrianz100% (10)
- Buccal Fat Pad Review PDFDocument4 pagesBuccal Fat Pad Review PDFNavatha MorthaNo ratings yet
- 1.1 Introduction To Human Anatomy - 2018-2019 PDFDocument11 pages1.1 Introduction To Human Anatomy - 2018-2019 PDFسيف محمود شاكر حسنNo ratings yet
- Ankle: FracturesDocument87 pagesAnkle: FracturesrifkialbanaNo ratings yet