Download as pdf or txt
You might also like
- Market Research Survey Sample QuestionnaireDocument4 pagesMarket Research Survey Sample QuestionnaireKhenan James Narisma100% (1)
- Daily Observation ReportDocument1 pageDaily Observation ReportAnsar AliNo ratings yet
- July SMR RevDocument2 pagesJuly SMR RevShyam SadanandanNo ratings yet
- INV Action Plan TemplateDocument2 pagesINV Action Plan Templateloveson709No ratings yet
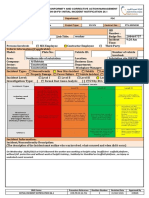
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocument2 pagesIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky BisNo ratings yet
- Templates Package 1 ContentDocument1 pageTemplates Package 1 ContentM IqbalNo ratings yet
- S/# Title This Week Figures Cumulative: Insert Epc/Sp/Mc Name and NumberDocument3 pagesS/# Title This Week Figures Cumulative: Insert Epc/Sp/Mc Name and NumberFarhat SetharNo ratings yet
- Weekly Progress Report 21 To 27 OCT2017Document2 pagesWeekly Progress Report 21 To 27 OCT2017Mehdi MessNo ratings yet
- Sample Template - Safety-DashboardDocument6 pagesSample Template - Safety-DashboardSivakumar ENo ratings yet
- Hazard ObservationDocument8 pagesHazard ObservationMarya HasniNo ratings yet
- 2021 Scorecard - Mark Christian Gullem Final For Supervisor SignatureDocument2 pages2021 Scorecard - Mark Christian Gullem Final For Supervisor SignatureAfroz SheikhNo ratings yet
- Entity EHSMS Quarterly Performance ReportDocument3 pagesEntity EHSMS Quarterly Performance ReportwritemeyouNo ratings yet
- HSE-003-HSE Plan - RV-02Document53 pagesHSE-003-HSE Plan - RV-02Jomy JohnyNo ratings yet
- EHS Observation Report FormatDocument1 pageEHS Observation Report FormatDore101No ratings yet
- Construction Site Safety Control Measures For Covid-19Document34 pagesConstruction Site Safety Control Measures For Covid-19Achik WahabNo ratings yet
- Pre Start Job MeetingDocument1 pagePre Start Job MeetingSardarFaisalHameedNo ratings yet
- Ra1 - General Risk Assessment Form 2015Document3 pagesRa1 - General Risk Assessment Form 2015api-349297013No ratings yet
- Daily Safety Compliance Report For InterviewDocument7 pagesDaily Safety Compliance Report For InterviewLemuel PetronioNo ratings yet
- Weekly Report As of September 12Document45 pagesWeekly Report As of September 12Cesar DuriasNo ratings yet
- Safety Report Weekly 6.12 Till 12.12.2021Document4 pagesSafety Report Weekly 6.12 Till 12.12.2021FARHANAH AFIQAH RAZMANNo ratings yet
- Waste Monitoring Flow Chart PicDocument1 pageWaste Monitoring Flow Chart PicDilip Kumar KNo ratings yet
- Close Out Report: Hse Department Period: JUNE 2013 - OCTOBER 2013 1 Article - Sub Sea Manifold ProjectDocument59 pagesClose Out Report: Hse Department Period: JUNE 2013 - OCTOBER 2013 1 Article - Sub Sea Manifold Projectadi100% (1)
- IGC3 - Exam TemplateDocument17 pagesIGC3 - Exam Templatevishal_sonari100% (1)
- Skweyiya Funeral ProgrammeDocument12 pagesSkweyiya Funeral ProgrammeeNCA.comNo ratings yet
- 9 Safety Inspection Report (Daily and Weekly) 01-12-14Document3 pages9 Safety Inspection Report (Daily and Weekly) 01-12-14Saboor KabierNo ratings yet
- HSE ALERT NO. 13-Near Miss ReportingDocument1 pageHSE ALERT NO. 13-Near Miss ReportingClark Angelo JuanNo ratings yet
- Emergency Reporting Plan - BeloniaDocument4 pagesEmergency Reporting Plan - BeloniaMd Nurul IslamNo ratings yet
- Safety Quiz - Answer PDFDocument1 pageSafety Quiz - Answer PDFRedzwan KadirNo ratings yet
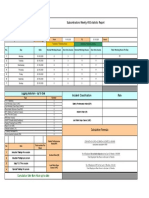
- Subcontractors Weekly HSE Statictic Report: Lagging Indicators - Up To DateDocument1 pageSubcontractors Weekly HSE Statictic Report: Lagging Indicators - Up To Dateindra setiawanNo ratings yet
- Training ReportDocument2 pagesTraining ReportisukuruNo ratings yet
- Risk Assessment: Kitchen - HomeDocument5 pagesRisk Assessment: Kitchen - HomesonofoddinNo ratings yet
- Hse StaticsDocument1 pageHse StaticsBhagat DeepakNo ratings yet
- PD Ga CKP Juli 2023 NewDocument1 pagePD Ga CKP Juli 2023 NewEggi AdityaNo ratings yet
- Safety Meeting PHTDocument2 pagesSafety Meeting PHTMohamad Hidayat Zainul Masri100% (2)
- Post Applied For: HSE/Safety Engineer: Kamal AhmadDocument3 pagesPost Applied For: HSE/Safety Engineer: Kamal Ahmadsudeesh kumarNo ratings yet
- MOSH Health & Safety 14-01-2021Document31 pagesMOSH Health & Safety 14-01-2021Mahmood AliNo ratings yet
- SAM-HSE-F-003-03 Safety Induction Checklist (Project)Document2 pagesSAM-HSE-F-003-03 Safety Induction Checklist (Project)Azman.jpamNo ratings yet
- Accident Incident Report (Promat)Document2 pagesAccident Incident Report (Promat)jonesNo ratings yet
- Monthly HSE Report - January 2022Document13 pagesMonthly HSE Report - January 2022adeniyi abiolaNo ratings yet
- Hse Training Plan Template ExcelDocument2 pagesHse Training Plan Template ExcelNasri matar0% (1)
- GC3 Main FindingsDocument3 pagesGC3 Main Findingsadnanshaikh0988% (8)
- Risk Assessment FormDocument4 pagesRisk Assessment FormFrankie FryNo ratings yet
- GC3 ObservationDocument16 pagesGC3 ObservationjithinNo ratings yet
- 1.1 Buildings and FloorsDocument4 pages1.1 Buildings and FloorsMohamed Mouner100% (1)
- 01 04 AMM Daily HSE Statistics Report AprDocument1 page01 04 AMM Daily HSE Statistics Report AprPT. ANUGRAH MIRAN MANDIRINo ratings yet
- Daily OHSE ReportDocument1 pageDaily OHSE ReportNavnath Ambre100% (1)
- P Awjo Hse 003Document3 pagesP Awjo Hse 003fajarbamNo ratings yet
- 3.3.1 ANNUAL HSE STATISTICS REPORT 21aDocument1 page3.3.1 ANNUAL HSE STATISTICS REPORT 21aTunde SodeindeNo ratings yet
- Incident Reporting Form (Ir 01) : Fatality Lti I RWC Accident NEAR MissDocument1 pageIncident Reporting Form (Ir 01) : Fatality Lti I RWC Accident NEAR Missmuhammadumar412296No ratings yet
- OHS-PR-09-26-F01 INITIAL INCIDENT NOTIFICATION SS8358 Misk City ABC, January 26, 2022Document2 pagesOHS-PR-09-26-F01 INITIAL INCIDENT NOTIFICATION SS8358 Misk City ABC, January 26, 2022Shafie ZubierNo ratings yet
- Work Inspection Checklist: Project DetailsDocument1 pageWork Inspection Checklist: Project Detailsmark lester caluzaNo ratings yet
- Safety ObservationDocument327 pagesSafety ObservationSafetyNo ratings yet
- MS B4 - Monthly Report October 2023..Document23 pagesMS B4 - Monthly Report October 2023..safety.nagoor1992No ratings yet
- Qhse Monthly Report UpdateDocument8 pagesQhse Monthly Report Updatechristologo manzanoNo ratings yet
- Protecting Lone Workers: How To Manage The Risks of Working AloneDocument16 pagesProtecting Lone Workers: How To Manage The Risks of Working Alonesamer alrawashdehNo ratings yet
- Mock Drill Observer Feedback Form Rev-01Document1 pageMock Drill Observer Feedback Form Rev-01Mohammad ArifNo ratings yet
- Heat StressDocument2 pagesHeat StressVivian GonzalesNo ratings yet
- Incident ReportDocument3 pagesIncident ReportbmkallarackalNo ratings yet
- Near Miss Incident Accident Report and Investigation FormDocument3 pagesNear Miss Incident Accident Report and Investigation Formhutomo_90No ratings yet
- Lap 7 ArtDocument8 pagesLap 7 Artapi-299330082No ratings yet
- Maad 20brochure 20knDocument2 pagesMaad 20brochure 20knapi-299330082No ratings yet
- SitemaplessonDocument3 pagesSitemaplessonapi-299330082No ratings yet
- Finalassignment 1 S 269009 Etp 4252072017Document8 pagesFinalassignment 1 S 269009 Etp 4252072017api-299330082No ratings yet
- UxandlogotypelessonDocument3 pagesUxandlogotypelessonapi-299330082No ratings yet
- LayersDocument3 pagesLayersapi-299330082No ratings yet
- Photoshop LessonDocument3 pagesPhotoshop Lessonapi-299330082No ratings yet
- Character Design AnimalDocument3 pagesCharacter Design Animalapi-299330082No ratings yet
- 2014 Parent Carers Complaints PolicyDocument2 pages2014 Parent Carers Complaints Policyapi-299330082No ratings yet
- Etp410 Form B-StudentDocument2 pagesEtp410 Form B-Studentapi-299330082No ratings yet
- Water Managment PlanDocument31 pagesWater Managment Planmehmal malikNo ratings yet
- Under Keel Clearnace (Filled-Up)Document1 pageUnder Keel Clearnace (Filled-Up)CHERRY ANN OLAJAYNo ratings yet
- Getachew AlemuDocument4 pagesGetachew AlemuGetachew AlemuNo ratings yet
- Cylinder Assy - Backhoe SwingDocument3 pagesCylinder Assy - Backhoe SwingivaldodanielNo ratings yet
- Listen To Perform Simon Says (With A Twist)Document5 pagesListen To Perform Simon Says (With A Twist)Hyacith Mae CanawayNo ratings yet
- Castle Clothing Co, E-ProfileDocument10 pagesCastle Clothing Co, E-ProfileraghuNo ratings yet
- Operator's Manual: Short-Reach Specification Machine (For Digging Operation) (S-SR120-B)Document88 pagesOperator's Manual: Short-Reach Specification Machine (For Digging Operation) (S-SR120-B)TommyNo ratings yet
- Chapter 3 WileyDocument20 pagesChapter 3 Wileyp876468No ratings yet
- Financial Management ImportantDocument6 pagesFinancial Management ImportantDippak ChabraNo ratings yet
- Fourier Series LessonDocument41 pagesFourier Series Lessonjackson246No ratings yet
- Ligia - Balbino Assignment 1 Version 2Document4 pagesLigia - Balbino Assignment 1 Version 2liesil100% (1)
- Sensors: Fluorescent Sensors For The Detection of Heavy Metal Ions in Aqueous MediaDocument34 pagesSensors: Fluorescent Sensors For The Detection of Heavy Metal Ions in Aqueous MediaTam Van TranNo ratings yet
- Aaaexamination PermitDocument1 pageAaaexamination PermitEmma KagutaNo ratings yet
- Ship Power PlantDocument141 pagesShip Power Plantnguyentrunghieu51dltt100% (2)
- Balmer Lawrie & Co HRDocument6 pagesBalmer Lawrie & Co HRPraneet TNo ratings yet
- Thermal Protection and Gate Protection of SCRDocument5 pagesThermal Protection and Gate Protection of SCRSnehasis BarikNo ratings yet
- Vibration Severity ChartsDocument4 pagesVibration Severity ChartsallmcbeallNo ratings yet
- ANA L. ANG, Petitioner, vs. TORIBIO TEODORO, Respondent. G.R. No. L-48226Document2 pagesANA L. ANG, Petitioner, vs. TORIBIO TEODORO, Respondent. G.R. No. L-48226Joven DelagenteNo ratings yet
- Phy Lab PDFDocument4 pagesPhy Lab PDFAlisha AgarwalNo ratings yet
- Transmission Gate Characteristics: DS DSDocument17 pagesTransmission Gate Characteristics: DS DSradeonleonNo ratings yet
- Azolla ZSDocument1 pageAzolla ZSSami KahtaniNo ratings yet
- Chapter 9 CapacitorsDocument11 pagesChapter 9 CapacitorsnNo ratings yet
- Ir - EFFRA INDUSTRIES LLP - MEW MS PO 02 2022 23 - 462023 - 472023ICS4199Document2 pagesIr - EFFRA INDUSTRIES LLP - MEW MS PO 02 2022 23 - 462023 - 472023ICS4199Voltonix InfratechNo ratings yet
- AssignmentDocument4 pagesAssignmentDenzel ChiuseniNo ratings yet
- Investigations of Some Properties of Oxysulphate of Magnesium by Admixing Zinc Oxide As An AdditiveDocument6 pagesInvestigations of Some Properties of Oxysulphate of Magnesium by Admixing Zinc Oxide As An AdditiveIJRASETPublicationsNo ratings yet
- Road Accidents in Malaysia - Causes & SolutionsDocument9 pagesRoad Accidents in Malaysia - Causes & Solutionssolidvanz100% (5)
- Leaf Description - PPT For Children..adverb RecapDocument6 pagesLeaf Description - PPT For Children..adverb RecapkokzdarlzNo ratings yet
- Military Exrcises of India Updated 15Document9 pagesMilitary Exrcises of India Updated 15Amit KayNo ratings yet
- Nursing Home Private Hospital / ICU Nursing Chart: 6 HR 18 HRDocument2 pagesNursing Home Private Hospital / ICU Nursing Chart: 6 HR 18 HRdavidNo ratings yet