Download as docx, pdf, or txt
You might also like
- Final Exam NRNP-6531 Advanced PracticeDocument21 pagesFinal Exam NRNP-6531 Advanced PracticeGeorge Ekai100% (4)
- Case Study Liver CirrhosisDocument64 pagesCase Study Liver CirrhosisJoseph Emmanuel Canda100% (1)
- GCAA Air Law ReviewDocument43 pagesGCAA Air Law ReviewAnonymous BiosaDDZVH100% (3)
- Ovarian Cyst - CSDocument42 pagesOvarian Cyst - CSMASII88% (26)
- BIOL 1700 - Test 1 - Important InformationDocument4 pagesBIOL 1700 - Test 1 - Important InformationSophie100% (1)
- A Case of PCAP-C (Individual INP)Document44 pagesA Case of PCAP-C (Individual INP)Preiane PayladoNo ratings yet
- Obstetrics and Gynaecology History Taking TemplateDocument4 pagesObstetrics and Gynaecology History Taking TemplateMaruti100% (3)
- GUILLAIN BARRE SYNDROME CASE STUDY (Group)Document28 pagesGUILLAIN BARRE SYNDROME CASE STUDY (Group)Kylie Golindang100% (7)
- DMD Walkthrough - V0.22Document8 pagesDMD Walkthrough - V0.22Gian GNo ratings yet
- Ectopic PregnancyDocument36 pagesEctopic PregnancyCham Ingalla Pascion100% (10)
- BSN Level III Clinical InstructorDocument33 pagesBSN Level III Clinical InstructorChristine Bell JapitanaNo ratings yet
- Central Luzon Doctors' Hospital Educational Institution: Department of NursingDocument86 pagesCentral Luzon Doctors' Hospital Educational Institution: Department of NursingDianneNo ratings yet
- DTS Live Birth, PROM Associated With Severe Pre-Eclampsia and Anemia 2 Degree To Acute Blood LossDocument30 pagesDTS Live Birth, PROM Associated With Severe Pre-Eclampsia and Anemia 2 Degree To Acute Blood LossChe LaiNo ratings yet
- 2M RevisedDocument109 pages2M RevisedRolland Ray MendozaNo ratings yet
- Acute PancreatitisDocument10 pagesAcute PancreatitisCuttie Anne GalangNo ratings yet
- 2M RevisedDocument109 pages2M RevisedRolland Ray MendozaNo ratings yet
- AppendicitisDocument32 pagesAppendicitisEarlKristofferdeGuia100% (3)
- Gcs Prolonged Labor 1Document58 pagesGcs Prolonged Labor 1Krishane JustaleroNo ratings yet
- Appendicitis SampleDocument15 pagesAppendicitis SampleChiqui Lao DumanhugNo ratings yet
- Acute Gastroenteritis With Moderate Dehydration, Congenital IchthyosisDocument36 pagesAcute Gastroenteritis With Moderate Dehydration, Congenital IchthyosisSunshine JaranillaNo ratings yet
- HCS 3rd YearDocument44 pagesHCS 3rd YearDafny CzarinaNo ratings yet
- Case Study Ucmed 6TH FloorDocument44 pagesCase Study Ucmed 6TH FloorPasay Trisha Faye Y.No ratings yet
- Liceo de Cagayan University College of NursingDocument44 pagesLiceo de Cagayan University College of NursingMary SengNo ratings yet
- Case!Document64 pagesCase!Abigael Rubio de LeonNo ratings yet
- Chapter 12 p.1 14Document15 pagesChapter 12 p.1 14angelasotocornetaNo ratings yet
- Gunshot Wound PeritonitisDocument66 pagesGunshot Wound PeritonitisMia Charisse FigueroaNo ratings yet
- Guillain Barre Syndrome Case Study GroupDocument28 pagesGuillain Barre Syndrome Case Study Groupyamie sulongNo ratings yet
- Case Study ObcsDocument41 pagesCase Study ObcsKrischelle Abella Sabordo100% (1)
- Table of Content: Chapte R Pages NODocument38 pagesTable of Content: Chapte R Pages NOAmirNo ratings yet
- Case Study - Group 3 Community Health NursingDocument31 pagesCase Study - Group 3 Community Health NursingApple MendozaNo ratings yet
- Case Pre For Normal OBDocument34 pagesCase Pre For Normal OBGrex TanNo ratings yet
- BSN 2 1 Group 3 Revised Grand Case Paper GDMDocument67 pagesBSN 2 1 Group 3 Revised Grand Case Paper GDMChristine Ann Gotan100% (1)
- IUFDDocument62 pagesIUFDMae Quito100% (1)
- Intro Ana-PhyDocument73 pagesIntro Ana-PhyKeith Lopez de VillaNo ratings yet
- GRP43 Manuscript-1Document69 pagesGRP43 Manuscript-1Marjune DimayugaNo ratings yet
- MCN Case Study-2pDocument76 pagesMCN Case Study-2pAngeline ShackletonNo ratings yet
- Case Study REVISEDDocument88 pagesCase Study REVISEDE.J. PelayoNo ratings yet
- Incomplete Abortion MINI CASE STUDY Group 3Document23 pagesIncomplete Abortion MINI CASE STUDY Group 3Katrina Tinapian100% (1)
- Grand Case Presentation SampleDocument23 pagesGrand Case Presentation SampleWillieNo ratings yet
- Multifetal Gestation Case StudyDocument67 pagesMultifetal Gestation Case StudyNikki Joy NavarroNo ratings yet
- A Delivery Room Write-UpDocument42 pagesA Delivery Room Write-UpDyanne BautistaNo ratings yet
- Assessment Tool BMS Year 2 Sem 2Document12 pagesAssessment Tool BMS Year 2 Sem 2Stephen KigoziNo ratings yet
- Appendectomy: (A Case Study)Document33 pagesAppendectomy: (A Case Study)Generose Laranang100% (1)
- MCU 2018 Workbook For Diagnostic Medical Sonography A Guide To ClinicalDocument496 pagesMCU 2018 Workbook For Diagnostic Medical Sonography A Guide To ClinicalHAVIZ YUADNo ratings yet
- Case Study - BronchopneumoniaDocument108 pagesCase Study - BronchopneumoniaAnthony WallNo ratings yet
- Nursing Care Management of A Client With Postpartum Iron Deficiency AnemiaDocument29 pagesNursing Care Management of A Client With Postpartum Iron Deficiency AnemiaLaurente, Patrizja Ysabel B. BSN-2DNo ratings yet
- Tagum Doctors CollegeDocument9 pagesTagum Doctors CollegeAya AringoyNo ratings yet
- A Student Manual of Clinical Skills 13 7 8Document194 pagesA Student Manual of Clinical Skills 13 7 8mofath100% (5)
- HMOLEDocument34 pagesHMOLEZuellen Mae Garapan BedañoNo ratings yet
- ACUTE-GASTROENTERITIS Case Study V6Document38 pagesACUTE-GASTROENTERITIS Case Study V6JOHN ALLEN GUISDANNo ratings yet
- JMDocument45 pagesJMDana Fajardo RezanoNo ratings yet
- Silvestri Chapter 46 Ed56ADocument31 pagesSilvestri Chapter 46 Ed56ABobet Reña100% (1)
- HyperbilirubinemiaDocument29 pagesHyperbilirubinemiaCham Ingalla Pascion88% (8)
- Case Protocol OB - H MOLEDocument3 pagesCase Protocol OB - H MOLEKim Adarem Joy ManimtimNo ratings yet
- Essential Medical Disorders of the Stomach and Small Intestine: A Clinical CasebookFrom EverandEssential Medical Disorders of the Stomach and Small Intestine: A Clinical CasebookNo ratings yet
- The Doctor's Guide to Gastrointestinal Health: Preventing and Treating Acid Reflux, Ulcers, Irritable Bowel Syndrome, Diverticulitis, Celiac Disease, Colon Cancer, Pancreatitis, Cirrhosis, Hernias and moreFrom EverandThe Doctor's Guide to Gastrointestinal Health: Preventing and Treating Acid Reflux, Ulcers, Irritable Bowel Syndrome, Diverticulitis, Celiac Disease, Colon Cancer, Pancreatitis, Cirrhosis, Hernias and moreRating: 3 out of 5 stars3/5 (2)
- Comprehensive Perspectives in Abdominal Compartment Syndrome: Understanding, Management, and Future DirectionsFrom EverandComprehensive Perspectives in Abdominal Compartment Syndrome: Understanding, Management, and Future DirectionsNo ratings yet
- Recurrent Pregnancy LossFrom EverandRecurrent Pregnancy LossOle Bjarne ChristiansenNo ratings yet
- Inflammatory Bowel Disease: Pathogenesis, Diagnosis and ManagementFrom EverandInflammatory Bowel Disease: Pathogenesis, Diagnosis and ManagementRamona RajapakseNo ratings yet
- Education for Pre- and Postoperative Procedures: A Special Urologic Nursing Focus SeriesFrom EverandEducation for Pre- and Postoperative Procedures: A Special Urologic Nursing Focus SeriesSusanne A. QuallichNo ratings yet
- Gastrointestinal Diseases and Disorders Sourcebook, Fifth EditionFrom EverandGastrointestinal Diseases and Disorders Sourcebook, Fifth EditionNo ratings yet
- CP 2 Vibration Monitoring and Analysis GuideDocument5 pagesCP 2 Vibration Monitoring and Analysis GuideCristian GarciaNo ratings yet
- Across National Tax Jurisdictions. Hence, A Company's Transfer-Pricing PoliciesDocument2 pagesAcross National Tax Jurisdictions. Hence, A Company's Transfer-Pricing PoliciesLJBernardoNo ratings yet
- "Body Ritual Among The Nacirema": MinerDocument7 pages"Body Ritual Among The Nacirema": MinerALLIA LOPEZNo ratings yet
- Open2023 OpenDocument13 pagesOpen2023 Openipsita lahiriNo ratings yet
- Bx6wh, Bx8wh, Bx12wh Ops, Parts ManualDocument122 pagesBx6wh, Bx8wh, Bx12wh Ops, Parts ManualArthur SemillaNo ratings yet
- House of Five ElementsDocument4 pagesHouse of Five ElementsBhavani U KulkarniNo ratings yet
- Slicer A400 / A400FB: Instruction ManualDocument82 pagesSlicer A400 / A400FB: Instruction ManualganaaNo ratings yet
- Syllabus Family Law - IIDocument5 pagesSyllabus Family Law - IIRachelle ChandraNo ratings yet
- Medical MalpracticeDocument14 pagesMedical MalpracticeKBPLex50% (2)
- ASTM E 1444 11 MT Magnetic Particle TestingDocument21 pagesASTM E 1444 11 MT Magnetic Particle TestingeliuNo ratings yet
- Where Does The Glycolysis OccourDocument2 pagesWhere Does The Glycolysis OccourMaria Claudette Andres AggasidNo ratings yet
- Criminal Justice Reform ActDocument5 pagesCriminal Justice Reform ActDNAinfoNewYork100% (1)
- Institute of Technology Division of Civil Eng. Safety and Environment Protection Management BDC 323 2 CRHDocument81 pagesInstitute of Technology Division of Civil Eng. Safety and Environment Protection Management BDC 323 2 CRHKinfe Dufera Gonfa100% (1)
- Disaster Nursing NotesDocument4 pagesDisaster Nursing NotesChannelG100% (1)
- Techinques Coloredpencils Basics2Document7 pagesTechinques Coloredpencils Basics2Roland CepedaNo ratings yet
- Iep-Case 8Document9 pagesIep-Case 8api-238729229No ratings yet
- The Bhawanipur Education Society College Department of CommerceDocument3 pagesThe Bhawanipur Education Society College Department of CommerceAyush PathakNo ratings yet
- Multi-Split Type Air Conditioners: DC Inverter Control Cooling Only and Reverse Cycle 50 HZDocument31 pagesMulti-Split Type Air Conditioners: DC Inverter Control Cooling Only and Reverse Cycle 50 HZvphuc1984No ratings yet
- ME-52023 Internal Combustion Engines: Technological University (Hmawbi) Department of Mechanical EngineeringDocument25 pagesME-52023 Internal Combustion Engines: Technological University (Hmawbi) Department of Mechanical EngineeringSi Thu Aung100% (1)
- Woodcraft Construction Kit Product CatalogueDocument35 pagesWoodcraft Construction Kit Product CatalogueBoban Svemogući ĐokićNo ratings yet
- Msds en Shell Tellus s2 M 68Document15 pagesMsds en Shell Tellus s2 M 68Debora Septania PurbaNo ratings yet
- Lecture 7 & 8 Non-Mendelian GeneticsDocument49 pagesLecture 7 & 8 Non-Mendelian GeneticsSaakshi PalNo ratings yet
- Lista de Exercicios Reported Speech 786250Document3 pagesLista de Exercicios Reported Speech 786250Ricardo SazaNo ratings yet
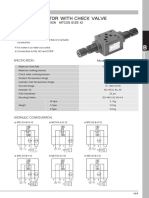
- MTC 03 W Throttle Check ValveDocument4 pagesMTC 03 W Throttle Check Valve박준용No ratings yet
- CIS Electrical Standard Rev 001Document46 pagesCIS Electrical Standard Rev 001Tarek AbulailNo ratings yet
- Status AnatomyDocument11 pagesStatus AnatomyLorng DeeNo ratings yet