
Ultrasound-Guided Block of The
Ultrasound-Guided Block of The
You might also like
- SJT Practice Paper 2 Large PrintDocument82 pagesSJT Practice Paper 2 Large PrintezzezzatNo ratings yet
- Apmc National Internship Program PrimerDocument10 pagesApmc National Internship Program PrimerSMR100% (1)
- 1.5T 3T Head Neck and Spine Array Coils - SM - Doc1821185 - 1Document92 pages1.5T 3T Head Neck and Spine Array Coils - SM - Doc1821185 - 1service iyadMedicalNo ratings yet
- Sports Medicine and Musculoskeletal Ultrasound: A Pocket Guide Mouhanad M. El-Othmani Henry T. Goitz J. Antonio BouffardDocument133 pagesSports Medicine and Musculoskeletal Ultrasound: A Pocket Guide Mouhanad M. El-Othmani Henry T. Goitz J. Antonio Bouffardnzkvw6s92hNo ratings yet
- EHR Module 6 PDFDocument4 pagesEHR Module 6 PDFJulie KiselevNo ratings yet
- (TS) HS70A - Booting Failed On System StartDocument6 pages(TS) HS70A - Booting Failed On System StartamirNo ratings yet
- The Preservation RhinoplastyDocument3 pagesThe Preservation RhinoplastyEvy Larousse33% (3)
- Highland Guidelines - LDK 2013-2-15Document3 pagesHighland Guidelines - LDK 2013-2-15andrew herringNo ratings yet
- Ultrasound and clinically guided Injection techniques on the musculoskeletal systemFrom EverandUltrasound and clinically guided Injection techniques on the musculoskeletal systemNo ratings yet
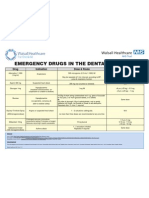
- Emergency Drugs Poster - Layout 1 in Dental PracticeDocument1 pageEmergency Drugs Poster - Layout 1 in Dental PracticeFady AtefNo ratings yet
- Thumb Congenital DisordersDocument16 pagesThumb Congenital Disordersqaz1122100% (1)
- K Opiods For Pain BupDocument2 pagesK Opiods For Pain Bupandrew herringNo ratings yet
- Basic Inpatient EM Coding TrainingDocument43 pagesBasic Inpatient EM Coding Trainingfahhad lashariNo ratings yet
- Anestesia Regional PerifericaDocument64 pagesAnestesia Regional PerifericaValeria GirónNo ratings yet
- Applications of Ultrasound in AnesthesiaDocument150 pagesApplications of Ultrasound in AnesthesiaLearnerNo ratings yet
- Peripheral Nerve Block The Upper ExtremityDocument43 pagesPeripheral Nerve Block The Upper ExtremityChristia Norielle MarambaNo ratings yet
- 3in1 Shoulder BlockDocument2 pages3in1 Shoulder BlockTejasvi ChandranNo ratings yet
- NYSORA Thoracic Paravertebral BlockDocument16 pagesNYSORA Thoracic Paravertebral BlockYee Yeow100% (1)
- Ultrasonography For The Upper Limb SurgeonDocument194 pagesUltrasonography For The Upper Limb Surgeonorthofitness2017100% (1)
- Annals of Plastic and Reconstructive SurgeryDocument10 pagesAnnals of Plastic and Reconstructive SurgeryLuiggi Fayad100% (2)
- Standards of Good Practice For Spinal Interventional ProceduresDocument20 pagesStandards of Good Practice For Spinal Interventional ProceduresMadyline VictoryaNo ratings yet
- Hemifacial SpasmDocument154 pagesHemifacial SpasmWalid YounesNo ratings yet
- CT Angiography of The Lower Extremities The Peripheral Vascular System Presents Unique Imaging ChallengesDocument7 pagesCT Angiography of The Lower Extremities The Peripheral Vascular System Presents Unique Imaging ChallengesDavid Puyó100% (1)
- Structural and Dynemic Base of Hand SurgeryDocument208 pagesStructural and Dynemic Base of Hand SurgeryTahaniNo ratings yet
- Updates Clinical: International Association For The Study of PainDocument6 pagesUpdates Clinical: International Association For The Study of PainSuaeni Kurnia WirdaNo ratings yet
- Immediate Post Anesthetic RecoveryDocument12 pagesImmediate Post Anesthetic Recoverysubvig100% (2)
- Ultrasound Guided Interventional Procedures In.4Document13 pagesUltrasound Guided Interventional Procedures In.4andrew herringNo ratings yet
- Harvesting Rib Cartilage Grafts For Secondary Rhinoplasty: Background: MethodsDocument7 pagesHarvesting Rib Cartilage Grafts For Secondary Rhinoplasty: Background: MethodsLuiggi Fayad100% (1)
- Preservation Rhinoplasty ProgrammeDocument11 pagesPreservation Rhinoplasty ProgrammeSaad LahmitiNo ratings yet
- Radiology 2013 ProgramDocument19 pagesRadiology 2013 ProgramMohamed ElkhodaryNo ratings yet
- Anesthesia: A Comprehensive Review (5th Edition)Document1 pageAnesthesia: A Comprehensive Review (5th Edition)brakim23No ratings yet
- Usg 20088Document18 pagesUsg 20088iridaNo ratings yet
- Medical Imaging Signals and SystemsDocument31 pagesMedical Imaging Signals and SystemssaraNo ratings yet
- Rhinoplasty: Edited by Michael J. BrennerDocument158 pagesRhinoplasty: Edited by Michael J. BrennerSang TrầnNo ratings yet
- Fundamentals of Diagnostic RadiologyDocument52 pagesFundamentals of Diagnostic RadiologyYabets100% (1)
- Artefactos en Ultrasonido, Un TutorialDocument25 pagesArtefactos en Ultrasonido, Un Tutorialramon100% (2)
- Aesthetic Surgery of The Orbits and EyelidsDocument31 pagesAesthetic Surgery of The Orbits and EyelidsdoctorbanNo ratings yet
- Abdomen CTDocument26 pagesAbdomen CTAnto BijuNo ratings yet
- Interpleural Block - Part 1: ReviewarticleDocument11 pagesInterpleural Block - Part 1: ReviewarticleAlfredo Salinas CastilloNo ratings yet
- 2017 PHD PanDocument243 pages2017 PHD PanAnonymous TfIKuBcaNo ratings yet
- Mri Master RodillaDocument9 pagesMri Master RodillaAndrea BelénNo ratings yet
- Complication of Spina AnesthesiaDocument8 pagesComplication of Spina AnesthesiaSandroLaoNo ratings yet
- Bob Peripheral Nerve Blocks AspanDocument70 pagesBob Peripheral Nerve Blocks AspanPrunaru BogdanNo ratings yet
- Thyroid UltrasoundDocument62 pagesThyroid Ultrasounddrmoscalin8774No ratings yet
- Musculoskeletal Ultrasound How To Treat CalcificDocument1 pageMusculoskeletal Ultrasound How To Treat Calcificrdk7471No ratings yet
- ALT Flap PrintDocument11 pagesALT Flap PrintSitha Christine100% (2)
- Dezena Endoscopic Third Ventriculostomy 2020Document114 pagesDezena Endoscopic Third Ventriculostomy 2020Carlos Daniel Giménez MéndezNo ratings yet
- X-Ray-Positioning Spine Dr. FritschDocument62 pagesX-Ray-Positioning Spine Dr. Fritschbjpalmer100% (3)
- Hadzic's Peripheral Nerve Blocks and Anatomy For Ultrasound Guided Regional Anesthesia (New York School of Regional Anesthesia) PDF DownloadDocument3 pagesHadzic's Peripheral Nerve Blocks and Anatomy For Ultrasound Guided Regional Anesthesia (New York School of Regional Anesthesia) PDF Downloadhellena buks33% (3)
- Recommended Reading List For EDAIC 2019Document5 pagesRecommended Reading List For EDAIC 2019Bebo EsmatNo ratings yet
- Peroneal Nerve Palsy PDFDocument10 pagesPeroneal Nerve Palsy PDFChristian Reza WibowoNo ratings yet
- Microsurgery Manual For Medical Students and ResidentsDocument199 pagesMicrosurgery Manual For Medical Students and ResidentsMuhammad RifkiNo ratings yet
- Emergency Chest ImagingDocument156 pagesEmergency Chest ImagingAshutosh KafleNo ratings yet
- Radiology Recent AdvancesDocument66 pagesRadiology Recent AdvancesDr.P.NatarajanNo ratings yet
- Complex Head and Neck Microvascular - SurgeryDocument327 pagesComplex Head and Neck Microvascular - Surgerydoctorsoha.shNo ratings yet
- Sonography of The Knee Joint PDFDocument8 pagesSonography of The Knee Joint PDFChavdarNo ratings yet
- The Scip Propeller Flap Versatility For R - 2019 - Journal of Plastic ReconstrDocument8 pagesThe Scip Propeller Flap Versatility For R - 2019 - Journal of Plastic Reconstrydk sinhNo ratings yet
- Structure Rhinoplasty Vol.3Document948 pagesStructure Rhinoplasty Vol.3drtechnoNo ratings yet
- Gluteal Artery Perforator FlapsDocument8 pagesGluteal Artery Perforator FlapsJose Mauricio Suarez BecerraNo ratings yet
- Atlas of 3D UltrasoundDocument71 pagesAtlas of 3D UltrasoundHalisson BastosNo ratings yet
- MR Requirements Musculoskeletal MRIDocument56 pagesMR Requirements Musculoskeletal MRIDifa ZafiraNo ratings yet
- Nerve Transfers. Hand Clin. Nov 2008Document175 pagesNerve Transfers. Hand Clin. Nov 2008k2rojo100% (1)
- EMG Trigerred StimulationDocument3 pagesEMG Trigerred StimulationralphholingsheadNo ratings yet
- Intro Head CTDocument34 pagesIntro Head CTbahar hoseiniNo ratings yet
- Advanced Endovascular Therapy of Aortic DiseaseFrom EverandAdvanced Endovascular Therapy of Aortic DiseaseAlan B. LumsdenNo ratings yet
- Local and Regional Flaps in Head and Neck Reconstruction: A Practical ApproachFrom EverandLocal and Regional Flaps in Head and Neck Reconstruction: A Practical ApproachRating: 2 out of 5 stars2/5 (1)
- Buprenorphine 2016-7-18Document1 pageBuprenorphine 2016-7-18andrew herringNo ratings yet
- Original Article: Serratus Plane Block: A Novel Ultrasound-Guided Thoracic Wall Nerve BlockDocument7 pagesOriginal Article: Serratus Plane Block: A Novel Ultrasound-Guided Thoracic Wall Nerve Blockandrew herringNo ratings yet
- Roux 2013Document7 pagesRoux 2013andrew herringNo ratings yet
- Rib Fracture SerratusDocument3 pagesRib Fracture Serratusandrew herring100% (1)
- Nej MR A 1511480Document9 pagesNej MR A 1511480Tohari Masidi AminNo ratings yet
- Intravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-OperatóriaDocument6 pagesIntravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-Operatóriaandrew herringNo ratings yet
- Rib Fracture W: PecsDocument8 pagesRib Fracture W: Pecsandrew herring100% (1)
- Herring ED Intractable Abdominal pain-N+VDocument1 pageHerring ED Intractable Abdominal pain-N+Vandrew herringNo ratings yet
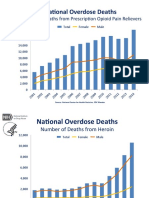
- OPR - Heroin DeathsDocument2 pagesOPR - Heroin Deathsandrew herringNo ratings yet
- 3.2.16.highland Emergency Medicine Journal Club Methods.2Document2 pages3.2.16.highland Emergency Medicine Journal Club Methods.2andrew herringNo ratings yet
- Dex For Dental Pain & SwellingDocument7 pagesDex For Dental Pain & Swellingandrew herring100% (1)
- Ketamine As Rescue Treatment FDocument8 pagesKetamine As Rescue Treatment Fandrew herringNo ratings yet
- CVS Action Plan v2Document1 pageCVS Action Plan v2andrew herringNo ratings yet
- Ultrasound Guided Interventional Procedures In.13Document14 pagesUltrasound Guided Interventional Procedures In.13andrew herring100% (1)
- Ultrasound Guided Interventional Procedures In.4Document13 pagesUltrasound Guided Interventional Procedures In.4andrew herringNo ratings yet
- Spinal Cord CompressionDocument19 pagesSpinal Cord CompressionNikai PabayoNo ratings yet
- Gymnastics - Trampoline: Sport Technical ManualDocument26 pagesGymnastics - Trampoline: Sport Technical ManualCharles MercadoNo ratings yet
- VIVA - Adult Recon ExaminerDocument22 pagesVIVA - Adult Recon ExaminerAlbert KosasihNo ratings yet
- Role of Forensic Toxicologist in The Management of Poisoning Cases in Casuality Department of A HospitalDocument2 pagesRole of Forensic Toxicologist in The Management of Poisoning Cases in Casuality Department of A HospitalKrupa PrajapatiNo ratings yet
- Placenta PreviaDocument2 pagesPlacenta PreviaIrish Joy S. DecrepitoNo ratings yet
- PDFDocument58 pagesPDFMuralidaran Selvaraj75% (4)
- UNC ED Pediatric Asthma ProtocolDocument2 pagesUNC ED Pediatric Asthma ProtocolAhmed BekhetNo ratings yet
- Cataract Art ScienceDocument405 pagesCataract Art Sciencesafasayed100% (4)
- Sana Haq ResumeDocument3 pagesSana Haq Resumeapi-354943357No ratings yet
- Medical Services and ManagementDocument17 pagesMedical Services and ManagementjohnNo ratings yet
- Nepal PosterDocument1 pageNepal Posterapi-282838160No ratings yet
- PrincetonDocument7 pagesPrincetonangel nahdeeNo ratings yet
- Basic Statistics (3685) PPT - Lecture On 20-01-2019Document64 pagesBasic Statistics (3685) PPT - Lecture On 20-01-2019M Hammad ManzoorNo ratings yet
- MST Nursing HandoutDocument3 pagesMST Nursing Handoutapi-261265221No ratings yet
- Date: - Volunteer Assessment Survey: First NameDocument3 pagesDate: - Volunteer Assessment Survey: First NameGilbert CookNo ratings yet
- Planning and Designing An Isolation Facility in Hospitals Need of The Hour PDFDocument9 pagesPlanning and Designing An Isolation Facility in Hospitals Need of The Hour PDFdzakyzahidNo ratings yet
- Vicarious Liability of HospitalsDocument2 pagesVicarious Liability of HospitalsAlison D'souzaNo ratings yet
- The Association of Blood Pressure and Primary Open-Angle Glaucoma: A Meta-AnalysisDocument23 pagesThe Association of Blood Pressure and Primary Open-Angle Glaucoma: A Meta-AnalysisSarah Martinauli HarahapNo ratings yet
- Blankenship 2015Document8 pagesBlankenship 2015Maria Heredero HernándezNo ratings yet
- AO 2016-0042 Annex H-6a Checklist For Review of Floor Plans - Level 1 HospitalDocument5 pagesAO 2016-0042 Annex H-6a Checklist For Review of Floor Plans - Level 1 HospitalNiel Angelo HagapeNo ratings yet
- Hospital Follow Up Progress Note MedicalTemplateDocument1 pageHospital Follow Up Progress Note MedicalTemplatee-MedTools100% (18)
- First Twenty Years of Little Traverse HospitalDocument11 pagesFirst Twenty Years of Little Traverse HospitalHarbor Springs Area Historical SocietyNo ratings yet
- Goiter Patients Admitted To The Mugana HospitalDocument7 pagesGoiter Patients Admitted To The Mugana HospitalMuhidin Issa MichuziNo ratings yet
- Safe HandoverDocument38 pagesSafe HandoverMatt Turner100% (1)
- Ceramics-Based Sealers: As New Alternative To Currently Used Endodontic SealersDocument7 pagesCeramics-Based Sealers: As New Alternative To Currently Used Endodontic SealersfoysalNo ratings yet






































































































Download as pdf or txt
You might also like
- SJT Practice Paper 2 Large PrintDocument82 pagesSJT Practice Paper 2 Large PrintezzezzatNo ratings yet
- Apmc National Internship Program PrimerDocument10 pagesApmc National Internship Program PrimerSMR100% (1)
- 1.5T 3T Head Neck and Spine Array Coils - SM - Doc1821185 - 1Document92 pages1.5T 3T Head Neck and Spine Array Coils - SM - Doc1821185 - 1service iyadMedicalNo ratings yet
- Sports Medicine and Musculoskeletal Ultrasound: A Pocket Guide Mouhanad M. El-Othmani Henry T. Goitz J. Antonio BouffardDocument133 pagesSports Medicine and Musculoskeletal Ultrasound: A Pocket Guide Mouhanad M. El-Othmani Henry T. Goitz J. Antonio Bouffardnzkvw6s92hNo ratings yet
- EHR Module 6 PDFDocument4 pagesEHR Module 6 PDFJulie KiselevNo ratings yet
- (TS) HS70A - Booting Failed On System StartDocument6 pages(TS) HS70A - Booting Failed On System StartamirNo ratings yet
- The Preservation RhinoplastyDocument3 pagesThe Preservation RhinoplastyEvy Larousse33% (3)
- Highland Guidelines - LDK 2013-2-15Document3 pagesHighland Guidelines - LDK 2013-2-15andrew herringNo ratings yet
- Ultrasound and clinically guided Injection techniques on the musculoskeletal systemFrom EverandUltrasound and clinically guided Injection techniques on the musculoskeletal systemNo ratings yet
- Emergency Drugs Poster - Layout 1 in Dental PracticeDocument1 pageEmergency Drugs Poster - Layout 1 in Dental PracticeFady AtefNo ratings yet
- Thumb Congenital DisordersDocument16 pagesThumb Congenital Disordersqaz1122100% (1)
- K Opiods For Pain BupDocument2 pagesK Opiods For Pain Bupandrew herringNo ratings yet
- Basic Inpatient EM Coding TrainingDocument43 pagesBasic Inpatient EM Coding Trainingfahhad lashariNo ratings yet
- Anestesia Regional PerifericaDocument64 pagesAnestesia Regional PerifericaValeria GirónNo ratings yet
- Applications of Ultrasound in AnesthesiaDocument150 pagesApplications of Ultrasound in AnesthesiaLearnerNo ratings yet
- Peripheral Nerve Block The Upper ExtremityDocument43 pagesPeripheral Nerve Block The Upper ExtremityChristia Norielle MarambaNo ratings yet
- 3in1 Shoulder BlockDocument2 pages3in1 Shoulder BlockTejasvi ChandranNo ratings yet
- NYSORA Thoracic Paravertebral BlockDocument16 pagesNYSORA Thoracic Paravertebral BlockYee Yeow100% (1)
- Ultrasonography For The Upper Limb SurgeonDocument194 pagesUltrasonography For The Upper Limb Surgeonorthofitness2017100% (1)
- Annals of Plastic and Reconstructive SurgeryDocument10 pagesAnnals of Plastic and Reconstructive SurgeryLuiggi Fayad100% (2)
- Standards of Good Practice For Spinal Interventional ProceduresDocument20 pagesStandards of Good Practice For Spinal Interventional ProceduresMadyline VictoryaNo ratings yet
- Hemifacial SpasmDocument154 pagesHemifacial SpasmWalid YounesNo ratings yet
- CT Angiography of The Lower Extremities The Peripheral Vascular System Presents Unique Imaging ChallengesDocument7 pagesCT Angiography of The Lower Extremities The Peripheral Vascular System Presents Unique Imaging ChallengesDavid Puyó100% (1)
- Structural and Dynemic Base of Hand SurgeryDocument208 pagesStructural and Dynemic Base of Hand SurgeryTahaniNo ratings yet
- Updates Clinical: International Association For The Study of PainDocument6 pagesUpdates Clinical: International Association For The Study of PainSuaeni Kurnia WirdaNo ratings yet
- Immediate Post Anesthetic RecoveryDocument12 pagesImmediate Post Anesthetic Recoverysubvig100% (2)
- Ultrasound Guided Interventional Procedures In.4Document13 pagesUltrasound Guided Interventional Procedures In.4andrew herringNo ratings yet
- Harvesting Rib Cartilage Grafts For Secondary Rhinoplasty: Background: MethodsDocument7 pagesHarvesting Rib Cartilage Grafts For Secondary Rhinoplasty: Background: MethodsLuiggi Fayad100% (1)
- Preservation Rhinoplasty ProgrammeDocument11 pagesPreservation Rhinoplasty ProgrammeSaad LahmitiNo ratings yet
- Radiology 2013 ProgramDocument19 pagesRadiology 2013 ProgramMohamed ElkhodaryNo ratings yet
- Anesthesia: A Comprehensive Review (5th Edition)Document1 pageAnesthesia: A Comprehensive Review (5th Edition)brakim23No ratings yet
- Usg 20088Document18 pagesUsg 20088iridaNo ratings yet
- Medical Imaging Signals and SystemsDocument31 pagesMedical Imaging Signals and SystemssaraNo ratings yet
- Rhinoplasty: Edited by Michael J. BrennerDocument158 pagesRhinoplasty: Edited by Michael J. BrennerSang TrầnNo ratings yet
- Fundamentals of Diagnostic RadiologyDocument52 pagesFundamentals of Diagnostic RadiologyYabets100% (1)
- Artefactos en Ultrasonido, Un TutorialDocument25 pagesArtefactos en Ultrasonido, Un Tutorialramon100% (2)
- Aesthetic Surgery of The Orbits and EyelidsDocument31 pagesAesthetic Surgery of The Orbits and EyelidsdoctorbanNo ratings yet
- Abdomen CTDocument26 pagesAbdomen CTAnto BijuNo ratings yet
- Interpleural Block - Part 1: ReviewarticleDocument11 pagesInterpleural Block - Part 1: ReviewarticleAlfredo Salinas CastilloNo ratings yet
- 2017 PHD PanDocument243 pages2017 PHD PanAnonymous TfIKuBcaNo ratings yet
- Mri Master RodillaDocument9 pagesMri Master RodillaAndrea BelénNo ratings yet
- Complication of Spina AnesthesiaDocument8 pagesComplication of Spina AnesthesiaSandroLaoNo ratings yet
- Bob Peripheral Nerve Blocks AspanDocument70 pagesBob Peripheral Nerve Blocks AspanPrunaru BogdanNo ratings yet
- Thyroid UltrasoundDocument62 pagesThyroid Ultrasounddrmoscalin8774No ratings yet
- Musculoskeletal Ultrasound How To Treat CalcificDocument1 pageMusculoskeletal Ultrasound How To Treat Calcificrdk7471No ratings yet
- ALT Flap PrintDocument11 pagesALT Flap PrintSitha Christine100% (2)
- Dezena Endoscopic Third Ventriculostomy 2020Document114 pagesDezena Endoscopic Third Ventriculostomy 2020Carlos Daniel Giménez MéndezNo ratings yet
- X-Ray-Positioning Spine Dr. FritschDocument62 pagesX-Ray-Positioning Spine Dr. Fritschbjpalmer100% (3)
- Hadzic's Peripheral Nerve Blocks and Anatomy For Ultrasound Guided Regional Anesthesia (New York School of Regional Anesthesia) PDF DownloadDocument3 pagesHadzic's Peripheral Nerve Blocks and Anatomy For Ultrasound Guided Regional Anesthesia (New York School of Regional Anesthesia) PDF Downloadhellena buks33% (3)
- Recommended Reading List For EDAIC 2019Document5 pagesRecommended Reading List For EDAIC 2019Bebo EsmatNo ratings yet
- Peroneal Nerve Palsy PDFDocument10 pagesPeroneal Nerve Palsy PDFChristian Reza WibowoNo ratings yet
- Microsurgery Manual For Medical Students and ResidentsDocument199 pagesMicrosurgery Manual For Medical Students and ResidentsMuhammad RifkiNo ratings yet
- Emergency Chest ImagingDocument156 pagesEmergency Chest ImagingAshutosh KafleNo ratings yet
- Radiology Recent AdvancesDocument66 pagesRadiology Recent AdvancesDr.P.NatarajanNo ratings yet
- Complex Head and Neck Microvascular - SurgeryDocument327 pagesComplex Head and Neck Microvascular - Surgerydoctorsoha.shNo ratings yet
- Sonography of The Knee Joint PDFDocument8 pagesSonography of The Knee Joint PDFChavdarNo ratings yet
- The Scip Propeller Flap Versatility For R - 2019 - Journal of Plastic ReconstrDocument8 pagesThe Scip Propeller Flap Versatility For R - 2019 - Journal of Plastic Reconstrydk sinhNo ratings yet
- Structure Rhinoplasty Vol.3Document948 pagesStructure Rhinoplasty Vol.3drtechnoNo ratings yet
- Gluteal Artery Perforator FlapsDocument8 pagesGluteal Artery Perforator FlapsJose Mauricio Suarez BecerraNo ratings yet
- Atlas of 3D UltrasoundDocument71 pagesAtlas of 3D UltrasoundHalisson BastosNo ratings yet
- MR Requirements Musculoskeletal MRIDocument56 pagesMR Requirements Musculoskeletal MRIDifa ZafiraNo ratings yet
- Nerve Transfers. Hand Clin. Nov 2008Document175 pagesNerve Transfers. Hand Clin. Nov 2008k2rojo100% (1)
- EMG Trigerred StimulationDocument3 pagesEMG Trigerred StimulationralphholingsheadNo ratings yet
- Intro Head CTDocument34 pagesIntro Head CTbahar hoseiniNo ratings yet
- Advanced Endovascular Therapy of Aortic DiseaseFrom EverandAdvanced Endovascular Therapy of Aortic DiseaseAlan B. LumsdenNo ratings yet
- Local and Regional Flaps in Head and Neck Reconstruction: A Practical ApproachFrom EverandLocal and Regional Flaps in Head and Neck Reconstruction: A Practical ApproachRating: 2 out of 5 stars2/5 (1)
- Buprenorphine 2016-7-18Document1 pageBuprenorphine 2016-7-18andrew herringNo ratings yet
- Original Article: Serratus Plane Block: A Novel Ultrasound-Guided Thoracic Wall Nerve BlockDocument7 pagesOriginal Article: Serratus Plane Block: A Novel Ultrasound-Guided Thoracic Wall Nerve Blockandrew herringNo ratings yet
- Roux 2013Document7 pagesRoux 2013andrew herringNo ratings yet
- Rib Fracture SerratusDocument3 pagesRib Fracture Serratusandrew herring100% (1)
- Nej MR A 1511480Document9 pagesNej MR A 1511480Tohari Masidi AminNo ratings yet
- Intravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-OperatóriaDocument6 pagesIntravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-Operatóriaandrew herringNo ratings yet
- Rib Fracture W: PecsDocument8 pagesRib Fracture W: Pecsandrew herring100% (1)
- Herring ED Intractable Abdominal pain-N+VDocument1 pageHerring ED Intractable Abdominal pain-N+Vandrew herringNo ratings yet
- OPR - Heroin DeathsDocument2 pagesOPR - Heroin Deathsandrew herringNo ratings yet
- 3.2.16.highland Emergency Medicine Journal Club Methods.2Document2 pages3.2.16.highland Emergency Medicine Journal Club Methods.2andrew herringNo ratings yet
- Dex For Dental Pain & SwellingDocument7 pagesDex For Dental Pain & Swellingandrew herring100% (1)
- Ketamine As Rescue Treatment FDocument8 pagesKetamine As Rescue Treatment Fandrew herringNo ratings yet
- CVS Action Plan v2Document1 pageCVS Action Plan v2andrew herringNo ratings yet
- Ultrasound Guided Interventional Procedures In.13Document14 pagesUltrasound Guided Interventional Procedures In.13andrew herring100% (1)
- Ultrasound Guided Interventional Procedures In.4Document13 pagesUltrasound Guided Interventional Procedures In.4andrew herringNo ratings yet
- Spinal Cord CompressionDocument19 pagesSpinal Cord CompressionNikai PabayoNo ratings yet
- Gymnastics - Trampoline: Sport Technical ManualDocument26 pagesGymnastics - Trampoline: Sport Technical ManualCharles MercadoNo ratings yet
- VIVA - Adult Recon ExaminerDocument22 pagesVIVA - Adult Recon ExaminerAlbert KosasihNo ratings yet
- Role of Forensic Toxicologist in The Management of Poisoning Cases in Casuality Department of A HospitalDocument2 pagesRole of Forensic Toxicologist in The Management of Poisoning Cases in Casuality Department of A HospitalKrupa PrajapatiNo ratings yet
- Placenta PreviaDocument2 pagesPlacenta PreviaIrish Joy S. DecrepitoNo ratings yet
- PDFDocument58 pagesPDFMuralidaran Selvaraj75% (4)
- UNC ED Pediatric Asthma ProtocolDocument2 pagesUNC ED Pediatric Asthma ProtocolAhmed BekhetNo ratings yet
- Cataract Art ScienceDocument405 pagesCataract Art Sciencesafasayed100% (4)
- Sana Haq ResumeDocument3 pagesSana Haq Resumeapi-354943357No ratings yet
- Medical Services and ManagementDocument17 pagesMedical Services and ManagementjohnNo ratings yet
- Nepal PosterDocument1 pageNepal Posterapi-282838160No ratings yet
- PrincetonDocument7 pagesPrincetonangel nahdeeNo ratings yet
- Basic Statistics (3685) PPT - Lecture On 20-01-2019Document64 pagesBasic Statistics (3685) PPT - Lecture On 20-01-2019M Hammad ManzoorNo ratings yet
- MST Nursing HandoutDocument3 pagesMST Nursing Handoutapi-261265221No ratings yet
- Date: - Volunteer Assessment Survey: First NameDocument3 pagesDate: - Volunteer Assessment Survey: First NameGilbert CookNo ratings yet
- Planning and Designing An Isolation Facility in Hospitals Need of The Hour PDFDocument9 pagesPlanning and Designing An Isolation Facility in Hospitals Need of The Hour PDFdzakyzahidNo ratings yet
- Vicarious Liability of HospitalsDocument2 pagesVicarious Liability of HospitalsAlison D'souzaNo ratings yet
- The Association of Blood Pressure and Primary Open-Angle Glaucoma: A Meta-AnalysisDocument23 pagesThe Association of Blood Pressure and Primary Open-Angle Glaucoma: A Meta-AnalysisSarah Martinauli HarahapNo ratings yet
- Blankenship 2015Document8 pagesBlankenship 2015Maria Heredero HernándezNo ratings yet
- AO 2016-0042 Annex H-6a Checklist For Review of Floor Plans - Level 1 HospitalDocument5 pagesAO 2016-0042 Annex H-6a Checklist For Review of Floor Plans - Level 1 HospitalNiel Angelo HagapeNo ratings yet
- Hospital Follow Up Progress Note MedicalTemplateDocument1 pageHospital Follow Up Progress Note MedicalTemplatee-MedTools100% (18)
- First Twenty Years of Little Traverse HospitalDocument11 pagesFirst Twenty Years of Little Traverse HospitalHarbor Springs Area Historical SocietyNo ratings yet
- Goiter Patients Admitted To The Mugana HospitalDocument7 pagesGoiter Patients Admitted To The Mugana HospitalMuhidin Issa MichuziNo ratings yet
- Safe HandoverDocument38 pagesSafe HandoverMatt Turner100% (1)
- Ceramics-Based Sealers: As New Alternative To Currently Used Endodontic SealersDocument7 pagesCeramics-Based Sealers: As New Alternative To Currently Used Endodontic SealersfoysalNo ratings yet