Download as pdf or txt
You might also like
- OB-GYN - Shelf Review NotesDocument47 pagesOB-GYN - Shelf Review NotesJackJoseph95% (19)
- 2013 Sepsis GuidelinesDocument58 pages2013 Sepsis GuidelinesMuhd Azam100% (1)
- CNA772 - Respiratory Failure in ARDSDocument8 pagesCNA772 - Respiratory Failure in ARDSAby ZuñigaNo ratings yet
- Antimicrobial Resistance in Libya - 1970-2011Document8 pagesAntimicrobial Resistance in Libya - 1970-2011Khalifa Sifaw Ghenghesh100% (2)
- Juris Chapter 9Document4 pagesJuris Chapter 9IS99057No ratings yet
- Idiopathic Thrombocytopenic Purpura Henoch-Schönlein PurpuraDocument1 pageIdiopathic Thrombocytopenic Purpura Henoch-Schönlein PurpuraMadelyn MedlingNo ratings yet
- Patent Ductus ArteriosusDocument24 pagesPatent Ductus ArteriosusJustin Ahorro-DionisioNo ratings yet
- Bleeding in PregnancyDocument4 pagesBleeding in Pregnancyrame_badiNo ratings yet
- Amniotic Fluid Embolism - Diagnosis and Management 2016Document9 pagesAmniotic Fluid Embolism - Diagnosis and Management 2016drpumamanNo ratings yet
- Bronchiolitis Clinical Practice GuidelineDocument21 pagesBronchiolitis Clinical Practice GuidelineJuwita PratiwiNo ratings yet
- Biliary AtresiaDocument25 pagesBiliary Atresiajulius billiNo ratings yet
- Febrile SeizureDocument6 pagesFebrile SeizurepipimseptianaNo ratings yet
- Anaphylactic ReactionDocument9 pagesAnaphylactic ReactionZahir Jayvee Gayak IINo ratings yet
- Congenital Heart DiseaseDocument12 pagesCongenital Heart Diseaserakanootousan100% (1)
- What Are The Symptoms of Hydronephrosis?Document10 pagesWhat Are The Symptoms of Hydronephrosis?Rajendra Gautam100% (1)
- Vesicoureteral RefluxDocument4 pagesVesicoureteral RefluxPrasetya Ismail PermadiNo ratings yet
- Nur 111 Session 5 Sas 1Document7 pagesNur 111 Session 5 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Case Report of PneumoniaDocument3 pagesCase Report of PneumoniaCobzaru Mihai0% (1)
- Acute Glomerulonephritis: Group 8 PresentationDocument25 pagesAcute Glomerulonephritis: Group 8 PresentationcollinsmagNo ratings yet
- Diabetes InsipidusDocument7 pagesDiabetes Insipiduspaul_stefenson10No ratings yet
- Sample Medical Guidelines: Pediatric SeizureDocument2 pagesSample Medical Guidelines: Pediatric SeizureJohn PerezNo ratings yet
- Di Abetes Insipidus: Collaboration & Referral - PhysicianDocument1 pageDi Abetes Insipidus: Collaboration & Referral - PhysicianDaisy Jane KoNo ratings yet
- Ic-01-042 Infection Control in Emergency RoomDocument13 pagesIc-01-042 Infection Control in Emergency RoomDerick RanaNo ratings yet
- CAD - EBM September 2020 EditionDocument17 pagesCAD - EBM September 2020 EditionNaga Venkatamanoj Kumar PakalapatiNo ratings yet
- Nursing Care Plan (CASE STUDY DENGUE)Document10 pagesNursing Care Plan (CASE STUDY DENGUE)NiooleNo ratings yet
- Ventricular Septal DefectDocument12 pagesVentricular Septal DefectPutri LidyaCNo ratings yet
- PyelonephritisDocument9 pagesPyelonephritisAfif Al FatihNo ratings yet
- Post Operative Complications 2Document14 pagesPost Operative Complications 2drhiwaomer100% (5)
- Dermoid CystDocument29 pagesDermoid CystAlik ChuaNo ratings yet
- Ncma217-Day 4 - Ballard ScoringDocument4 pagesNcma217-Day 4 - Ballard ScoringAbegail Balloran0% (1)
- Research Proposal Atrial Septal DefectDocument28 pagesResearch Proposal Atrial Septal DefectIzharIsmailNo ratings yet
- Prevention and Treatment of Laryngospasm in The Pediatric Patient A Literature Review April 2019Document7 pagesPrevention and Treatment of Laryngospasm in The Pediatric Patient A Literature Review April 2019Elisa VargasNo ratings yet
- Treatment of Acute BronchitisDocument3 pagesTreatment of Acute BronchitisjokosudibyoNo ratings yet
- NCP PTBDocument9 pagesNCP PTBecbarticanNo ratings yet
- Acute Pyelonephritis in AdultsDocument12 pagesAcute Pyelonephritis in AdultsviinysantosNo ratings yet
- Bioterrorism: BY: - Bijay Kumar Mahato BPH 2 Semester Padmashree School of Public HealthDocument26 pagesBioterrorism: BY: - Bijay Kumar Mahato BPH 2 Semester Padmashree School of Public HealthBijay Kumar MahatoNo ratings yet
- Task 1 - Global Sample)Document6 pagesTask 1 - Global Sample)FATIN HAFIZAH MOHAMMAD SUKRINo ratings yet
- Neonatalhypoglycemia: Is There A Sweet Spot?Document14 pagesNeonatalhypoglycemia: Is There A Sweet Spot?karisman kadirNo ratings yet
- Atelectasis NFDocument57 pagesAtelectasis NFNurul FathiyaNo ratings yet
- Leptospirosis: Causes, Incidence, and Risk FactorsDocument6 pagesLeptospirosis: Causes, Incidence, and Risk FactorsJackii DoronilaNo ratings yet
- Garcia, Melegrito, Zamuco: Perforated Peptic Ulcer DiseaseDocument4 pagesGarcia, Melegrito, Zamuco: Perforated Peptic Ulcer DiseasePaulo GarciaNo ratings yet
- Natural History & Spectrum of DiseasesDocument26 pagesNatural History & Spectrum of DiseasesVincent Reyes100% (1)
- Essential Intrapartum Newborn Care: GOLEZ, Steffi Gabrielle RDocument9 pagesEssential Intrapartum Newborn Care: GOLEZ, Steffi Gabrielle RsteffiNo ratings yet
- Preoperative EvaluationDocument4 pagesPreoperative EvaluationFadly Setiawirawan100% (1)
- Cervical CancerDocument9 pagesCervical CancerRafaelJohannesNo ratings yet
- Concept Map DM FootDocument7 pagesConcept Map DM FootAlmira De JesusNo ratings yet
- Legal Medicine FinalsDocument13 pagesLegal Medicine FinalsBo DistNo ratings yet
- Ambulatory Care and Its Health RecordsDocument6 pagesAmbulatory Care and Its Health Recordsapi-302333945No ratings yet
- Murmur EvaluationDocument4 pagesMurmur EvaluationManjunath GeminiNo ratings yet
- The Perception of Pregnant Women Towards Antenatal Care at Madina Polyclinic-Ghana: A Descriptive Exploratory StudyDocument13 pagesThe Perception of Pregnant Women Towards Antenatal Care at Madina Polyclinic-Ghana: A Descriptive Exploratory StudyP'Babe Cece AdumoahNo ratings yet
- Tetralogy of FallotDocument8 pagesTetralogy of Fallotdecembergirl92No ratings yet
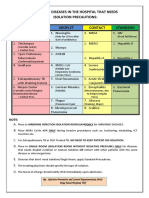
- Diseases That Needs Isolation PrecautionsDocument1 pageDiseases That Needs Isolation Precautionsjerimiah_manzonNo ratings yet
- Acute PharyngitisDocument51 pagesAcute PharyngitisrikafitriazaNo ratings yet
- Zoonotic Diseases: by Rita NkiroteDocument44 pagesZoonotic Diseases: by Rita NkiroteIsaac JumaNo ratings yet
- April Baylon2Document1 pageApril Baylon2April Love Baylon EndoNo ratings yet
- Aurelio - Afe PBLDocument26 pagesAurelio - Afe PBLLyca Mae AurelioNo ratings yet
- Amniotic Fluid Embolism.: ReferencesDocument7 pagesAmniotic Fluid Embolism.: ReferencesRSIA UMMINo ratings yet
- Amniotic Fluid EmbolismDocument13 pagesAmniotic Fluid Embolismelfa riniNo ratings yet
- Amniotic Fluid EmbolismDocument13 pagesAmniotic Fluid EmbolismDrNorNo ratings yet
- Pre EclampsiaDocument12 pagesPre EclampsiaJohn Mark PocsidioNo ratings yet
- Etiology, Clinical Manifestations, and Prediction of Placental AbruptionDocument9 pagesEtiology, Clinical Manifestations, and Prediction of Placental AbruptionKadije OanaNo ratings yet
- Amniotic Fluid Embolism: An Obstetric EmergencyDocument10 pagesAmniotic Fluid Embolism: An Obstetric EmergencyCaroline SidhartaNo ratings yet
- Barrett's OesophagusDocument20 pagesBarrett's OesophagusArri KurniawanNo ratings yet
- Ankle Ligaments On MRI Appearance of Normal and Injured LigamentsDocument9 pagesAnkle Ligaments On MRI Appearance of Normal and Injured LigamentsArri KurniawanNo ratings yet
- ACG Guideline GERD March 2013Document21 pagesACG Guideline GERD March 2013Arri KurniawanNo ratings yet
- Angina LudwigDocument4 pagesAngina LudwigArri KurniawanNo ratings yet
- AscariasisDocument11 pagesAscariasisArri Kurniawan100% (1)
- Inflamatory Brest CADocument9 pagesInflamatory Brest CAArri KurniawanNo ratings yet
- 9-Food and WaterTHE MICROBIOLOGICAL EXAMINATION OF FOODS & WATERDocument16 pages9-Food and WaterTHE MICROBIOLOGICAL EXAMINATION OF FOODS & WATERArri KurniawanNo ratings yet
- Hereditary Pituitary Dwarfism With Spontaneous PubertyDocument6 pagesHereditary Pituitary Dwarfism With Spontaneous PubertyArri KurniawanNo ratings yet
- Classification of Carious Lesions and Tooth PreparationDocument34 pagesClassification of Carious Lesions and Tooth PreparationArri KurniawanNo ratings yet
- Staphylococcus EnterotoxinDocument13 pagesStaphylococcus EnterotoxinArri KurniawanNo ratings yet
- Bahan Evo SeedDocument9 pagesBahan Evo SeedArri KurniawanNo ratings yet
- Obesteric Gynacology Short Notes For Usmle Step 2Document32 pagesObesteric Gynacology Short Notes For Usmle Step 2Rodaba Ahmadi Meherzad100% (1)
- Hematological Disorders and Pregnancy Associated Disease - 123200Document28 pagesHematological Disorders and Pregnancy Associated Disease - 123200Syed Yusuf SyedNo ratings yet
- Obstetrical EmergenciesDocument14 pagesObstetrical EmergenciesAswathy ChandranNo ratings yet
- Ayushman Bharat Arogya Karnataka Annexure 9 Package Rates Emergency Healthcare TreatmentsDocument36 pagesAyushman Bharat Arogya Karnataka Annexure 9 Package Rates Emergency Healthcare TreatmentsMidhilaNo ratings yet
- Cephalic Preterm Livebirth by Primary Lstcs Secondary To Hellp Syndrome Preeclampsia With Severe FeaturesDocument59 pagesCephalic Preterm Livebirth by Primary Lstcs Secondary To Hellp Syndrome Preeclampsia With Severe FeaturesAsterlyn ConiendoNo ratings yet
- SC DGN Metode Eracs 12 Des 2021Document31 pagesSC DGN Metode Eracs 12 Des 2021Rahmat AzimiNo ratings yet
- Revision Long Case Obs Gynae PDF FreeDocument10 pagesRevision Long Case Obs Gynae PDF Freesirajulislam6017No ratings yet
- HMS - Women's Health (MCQ & Notes)Document44 pagesHMS - Women's Health (MCQ & Notes)marouf elgoulNo ratings yet
- Case Study Group 2 Chapter 21Document4 pagesCase Study Group 2 Chapter 21Arnold ZamoroNo ratings yet
- Pre Eclampsia Case StudyDocument39 pagesPre Eclampsia Case StudyAnton RossiniNo ratings yet
- Obstetric Nursing Mentoring PDFDocument11 pagesObstetric Nursing Mentoring PDFDulle MulletNo ratings yet
- UwiseDocument26 pagesUwiseAyodeji SotimehinNo ratings yet
- Prelabor Rupture of MembranesDocument87 pagesPrelabor Rupture of MembranesJohn Paul DianNo ratings yet
- C1 Ob-Gyn-2020Document33 pagesC1 Ob-Gyn-2020yabsera mulatuNo ratings yet
- Questions and Answers in Maternal and Health NyrsingDocument10 pagesQuestions and Answers in Maternal and Health Nyrsingreden14No ratings yet
- NP2 Recalls1Document10 pagesNP2 Recalls1AhrisJeannine EscuadroNo ratings yet
- Copy EclampsiaDocument19 pagesCopy EclampsiaRobert ChilesheNo ratings yet
- Roisin Ryan Obstetrics Final Year RevisionDocument78 pagesRoisin Ryan Obstetrics Final Year RevisionDanny SchNo ratings yet
- Ob ReportDocument37 pagesOb ReportnicewanNo ratings yet
- Literature Review For Preterm Birth and Infant Mortality Online Copy pt1 Compressed PDFDocument216 pagesLiterature Review For Preterm Birth and Infant Mortality Online Copy pt1 Compressed PDFDgjj CompuiterNo ratings yet
- Midterm NotesDocument28 pagesMidterm NotesGen FranchesKyle Cortez ErigbuagasNo ratings yet
- Hematologic Changes in PregnancyDocument17 pagesHematologic Changes in PregnancyShofa NisaNo ratings yet
- Antepartum HaemorrhageDocument23 pagesAntepartum HaemorrhageSutanti Lara DewiNo ratings yet
- Obstetrics MCQsDocument12 pagesObstetrics MCQsDeeksha Bhardwaj100% (1)
- Maternal 8Document15 pagesMaternal 8shanikaNo ratings yet
- Code Blue: The Growing Threat of Non-Communicable Diseases On Maternal HealthDocument4 pagesCode Blue: The Growing Threat of Non-Communicable Diseases On Maternal HealthThe Wilson Center100% (1)
- Factors That May Affect The Unborn ChildDocument10 pagesFactors That May Affect The Unborn ChildDanica Mae de PedroNo ratings yet
- Assignments, Chapter 15, Nursing Care of A Family During Labor and BirthDocument8 pagesAssignments, Chapter 15, Nursing Care of A Family During Labor and BirthGLORY MI SHANLEY CARUMBANo ratings yet