Download as docx, pdf, or txt
You might also like
- 10 CaritosDocument3 pages10 CaritosDARREN EDMARK100% (4)
- NCM 118L/ 119L (Related Learning Experience) Day 3-ActivityDocument4 pagesNCM 118L/ 119L (Related Learning Experience) Day 3-ActivityNicole Villanueva, BSN - Level 3ANo ratings yet
- STEMI Complications TreatmentDocument54 pagesSTEMI Complications TreatmentAnonymous CQmrhq1O7100% (1)
- Activity Intolerance Related To AmeniaDocument1 pageActivity Intolerance Related To AmeniaSiti Syazana Mohamad MogriNo ratings yet
- NCPDocument3 pagesNCPJerome Vergel RubianesNo ratings yet
- Nursing Diagnosis Rationale Interventions Rationale EvaluationDocument2 pagesNursing Diagnosis Rationale Interventions Rationale EvaluationJobie CasipongNo ratings yet
- Impaired Tissue PerfusionDocument2 pagesImpaired Tissue PerfusionLyka Mae Imbat - PacnisNo ratings yet
- Assessment Explanation of The Problem Objectives Nursing Interventions Rationale Evaluation Subjective: STO: Within 4 Hour of DX: DX: Sto: Goal MetDocument5 pagesAssessment Explanation of The Problem Objectives Nursing Interventions Rationale Evaluation Subjective: STO: Within 4 Hour of DX: DX: Sto: Goal MetRussel SantosNo ratings yet
- NCP CKDDocument3 pagesNCP CKDRiel TumandaNo ratings yet
- Nursing Care PlanDocument11 pagesNursing Care Planaycee0316100% (1)
- PathophysiologyDocument1 pagePathophysiologyHazel PalomaresNo ratings yet
- Ineffective ProtectionDocument7 pagesIneffective Protectionapi-283822730No ratings yet
- NCP Ineffective Cardiopulmonary PerfusionDocument3 pagesNCP Ineffective Cardiopulmonary PerfusionjamiemapanaoNo ratings yet
- NCP Decreased Cardiac Output 1Document2 pagesNCP Decreased Cardiac Output 1Arnel MacabalitaoNo ratings yet
- Hypertensive NephrosclerosisDocument14 pagesHypertensive Nephrosclerosisreysanne100% (2)
- NCP and DStudyDocument8 pagesNCP and DStudyJessica Rosan Hewald ManapatNo ratings yet
- NCP GRAND CASE PRE C Nursing ProblemsDocument9 pagesNCP GRAND CASE PRE C Nursing ProblemsAngie Mandeoya100% (1)
- Ineffective Peripheral Tissue Perfusion Related To Vasoconstriction Secondary To High Glucose Level.Document6 pagesIneffective Peripheral Tissue Perfusion Related To Vasoconstriction Secondary To High Glucose Level.SAROL, RYAN CHRISTIAN B.No ratings yet
- NCP 2 CabalunaDocument7 pagesNCP 2 CabalunaIrene Grace BalcuevaNo ratings yet
- Nursing Care Plan For Myocardial InfarctionDocument1 pageNursing Care Plan For Myocardial InfarctionIshaBrijeshSharmaNo ratings yet
- NCP Risk For InfectionDocument6 pagesNCP Risk For InfectionCazze SunioNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- Rufino, Leslie Kriztel S. BSN 3-2 Group 1Document6 pagesRufino, Leslie Kriztel S. BSN 3-2 Group 1Deinielle Magdangal RomeroNo ratings yet
- Pathophysiology Diagram of Congestive Heart FailureDocument3 pagesPathophysiology Diagram of Congestive Heart FailureLeng Royo BrionesNo ratings yet
- DuphalacDocument2 pagesDuphalacianecunarNo ratings yet
- NCP Gastric CancerDocument6 pagesNCP Gastric Cancerhayascent hilarioNo ratings yet
- NCPDocument3 pagesNCPJezza RequilmeNo ratings yet
- Levemir Product Insert PDFDocument11 pagesLevemir Product Insert PDFDegee O. GonzalesNo ratings yet
- Cues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationMiggy SikatNo ratings yet
- Risk For Decreased Cardiac Tissue PerfusionDocument3 pagesRisk For Decreased Cardiac Tissue PerfusionKarina MadriagaNo ratings yet
- Ineffective Tissue PerfusionDocument2 pagesIneffective Tissue PerfusionDiane ReyNo ratings yet
- Velez College of Nursing F. Ramos Street, Cebu CityDocument57 pagesVelez College of Nursing F. Ramos Street, Cebu Cityinah krizia lagueNo ratings yet
- Example of Drug StudyDocument2 pagesExample of Drug Studydonna mae junioNo ratings yet
- NCP PTBDocument2 pagesNCP PTBMack Jhed AnarconNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Short Term Short TermDocument2 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective Short Term Short TermFrancis Xavier S. MendezNo ratings yet
- NCP CvaDocument4 pagesNCP CvaMariquita BuenafeNo ratings yet
- HCVDDocument5 pagesHCVDkhrizaleehNo ratings yet
- Activity IntoleranceDocument1 pageActivity IntoleranceAndrea Francesca SantosNo ratings yet
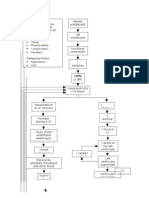
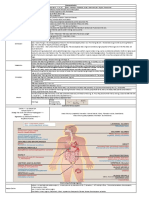
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyDocument3 pages"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyCarl Elexer Cuyugan Ano50% (2)
- NCP CHFDocument2 pagesNCP CHFaldrin1920No ratings yet
- MGH 8 - Ihd - NCPDocument12 pagesMGH 8 - Ihd - NCPSesinando Niez Quilao Jr.100% (1)
- Collaboration:: The Possibility of Acidosis Accompanied byDocument2 pagesCollaboration:: The Possibility of Acidosis Accompanied bymashupNo ratings yet
- Ineffective Cerebral Tissue Perfusion Related ToDocument7 pagesIneffective Cerebral Tissue Perfusion Related TohannahNo ratings yet
- Ncp'sDocument8 pagesNcp'sDuchess Kleine RafananNo ratings yet
- NCP Acitivity IntoleranceDocument3 pagesNCP Acitivity IntolerancegizelleNo ratings yet
- Anxiety R:T Death ThreatDocument8 pagesAnxiety R:T Death ThreatAlfredo BaulaNo ratings yet
- Decreased Cardiac OutputDocument4 pagesDecreased Cardiac OutputRenie SerranoNo ratings yet
- NCP PROPER Pain and Decreased Cardiac OutputDocument3 pagesNCP PROPER Pain and Decreased Cardiac OutputErienne Lae Manangan - CadalsoNo ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle AcenaNo ratings yet
- Hyperkalemia Discharge PlanDocument2 pagesHyperkalemia Discharge PlanDe Sesto Rhys CarloNo ratings yet
- Nursing Care Plan CVADocument6 pagesNursing Care Plan CVAessevyNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care Planjnx_anonymousNo ratings yet
- Tissue PerfusionDocument2 pagesTissue PerfusionMichael John LeandichoNo ratings yet
- Scribd 020922 Case Study-Oncology A&kDocument2 pagesScribd 020922 Case Study-Oncology A&kKellie DNo ratings yet
- Cu 5Document2 pagesCu 5Clareze AbadNo ratings yet
- NCP 1Document1 pageNCP 1hsiriaNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Angina PectorisDocument8 pagesAngina PectorisPrince DuNo ratings yet
- Case Analysis: Medical Surgical NursingDocument7 pagesCase Analysis: Medical Surgical NursingMaria ThereseNo ratings yet
- Req ERDocument9 pagesReq ERmayxzineNo ratings yet
- RNPIDEA-Coronary Artery Disease Nursing Care PlanDocument8 pagesRNPIDEA-Coronary Artery Disease Nursing Care PlanAngie MandeoyaNo ratings yet
- Laws On The Couple, The Child, & The FamilyDocument12 pagesLaws On The Couple, The Child, & The FamilyGerardeanne ReposarNo ratings yet
- Impaired Skin IntegrityDocument3 pagesImpaired Skin IntegrityGerardeanne Reposar100% (2)
- Pathophysiology of Rheumatoid ArthritisDocument1 pagePathophysiology of Rheumatoid ArthritisGerardeanne ReposarNo ratings yet
- Acute PainDocument3 pagesAcute PainGerardeanne ReposarNo ratings yet
- Family Nursing Care PlanDocument3 pagesFamily Nursing Care PlanGerardeanne ReposarNo ratings yet
- Home Visit PlanningDocument3 pagesHome Visit PlanningGerardeanne Reposar0% (1)
- Family Coping IndexDocument2 pagesFamily Coping IndexGerardeanne Reposar60% (5)
- Pansit PansitanDocument3 pagesPansit PansitanGerardeanne ReposarNo ratings yet
- Newborn Hearing Screening TestDocument11 pagesNewborn Hearing Screening TestGerardeanne Reposar100% (2)
- NCP Acute Pain NCSDocument3 pagesNCP Acute Pain NCSPaolo Vittorio Perdigueros GonzalesNo ratings yet
- Emergency Drugs Drug StudyDocument15 pagesEmergency Drugs Drug StudyCathrine Sandile Tangwara100% (1)
- Acute Coronary SyndromeDocument46 pagesAcute Coronary Syndromewiwidhipw18No ratings yet
- Chapter 23: Alterations of Cardiovascular FunctionDocument5 pagesChapter 23: Alterations of Cardiovascular Functionw1111am0% (1)
- Nursing Comps Study GuideDocument15 pagesNursing Comps Study GuideforminskoNo ratings yet
- ArtherosclerosisDocument23 pagesArtherosclerosistanyagargNo ratings yet
- Aging Changes in The Heart and Blood VesselsDocument4 pagesAging Changes in The Heart and Blood VesselsTotalenesya Reforrent SutiknoNo ratings yet
- Kelantan Guidelines For Nsteacs 2nd Edition 2012 PDFDocument48 pagesKelantan Guidelines For Nsteacs 2nd Edition 2012 PDFAhmad Nafais RahimiNo ratings yet
- Chest Pain. Surgical Treatment of Acute Coronary Syndrome (ACS)Document21 pagesChest Pain. Surgical Treatment of Acute Coronary Syndrome (ACS)Hanif ZamriNo ratings yet
- Case StudyDocument6 pagesCase StudyApoorv Jain100% (1)
- MSN Questions 100Document16 pagesMSN Questions 100Efreignz Mangay-at KinomesNo ratings yet
- Reffered PainDocument26 pagesReffered PainHappy Septianto SNo ratings yet
- Geria - CardioDocument4 pagesGeria - CardioLeah GordoncilloNo ratings yet
- Heart Attacks and There Effects On LifeDocument11 pagesHeart Attacks and There Effects On Lifeapi-291565665No ratings yet
- Angina PectorisDocument38 pagesAngina Pectorisekhafagy100% (1)
- Aberrant Ventricular Conduction Types and Concealed ConductionDocument25 pagesAberrant Ventricular Conduction Types and Concealed ConductionTemptationNo ratings yet
- Med Surg Care StudyDocument32 pagesMed Surg Care StudyNaFizzNo ratings yet
- Acute Coronary SyndromeDocument24 pagesAcute Coronary SyndromeSANU RAMASWAMYNo ratings yet
- Nitroglycerin Drug StudyDocument5 pagesNitroglycerin Drug StudyjuancristoNo ratings yet
- An Introduction To The 12 Lead EcgDocument85 pagesAn Introduction To The 12 Lead EcgAris Diyan YulistiawanNo ratings yet
- VEGFDocument20 pagesVEGFLivia Rhea AlvitaNo ratings yet
- Pharmacology Questions CardiacDocument5 pagesPharmacology Questions CardiacAmanda SimpsonNo ratings yet
- Cardiac Disease in PregnancyDocument21 pagesCardiac Disease in PregnancyRenata CilestrinaNo ratings yet
- Drug StudyDocument8 pagesDrug StudySarie LevitaNo ratings yet
- LipnCott Summary SmallerDocument21 pagesLipnCott Summary SmallerAdil Yousaf0% (1)
- Case Report: Medical Faculty of Hasanuddin University, Makassar 2013Document30 pagesCase Report: Medical Faculty of Hasanuddin University, Makassar 2013awalcybercityNo ratings yet
- Anaesthetic Management of Ihd Patients For Non Cardiac SurgeryDocument18 pagesAnaesthetic Management of Ihd Patients For Non Cardiac SurgerySuresh KumarNo ratings yet
- DR R.V.S.N. Sarma., Consultant Physician and Chest SpecialistDocument58 pagesDR R.V.S.N. Sarma., Consultant Physician and Chest SpecialistVaibhav BharatNo ratings yet
- CVS TimetableDocument6 pagesCVS TimetableKai BinNo ratings yet