Download as doc, pdf, or txt
You might also like
- Computerised Payroll Practice Set Using MYOB AccountRight: Australian EditionFrom EverandComputerised Payroll Practice Set Using MYOB AccountRight: Australian EditionNo ratings yet
- Claim Form For Supplementary Welfare Allowance: PleaseDocument4 pagesClaim Form For Supplementary Welfare Allowance: PleaseSparky Jon Bigolow100% (1)
- ESI Declaration Form1Document4 pagesESI Declaration Form1Satvik Manikanth25% (4)
- Joint Declaration Employee With Employer 2Document2 pagesJoint Declaration Employee With Employer 2Deepak Solanki100% (3)
- Dependency Form PDFDocument5 pagesDependency Form PDFVivek VenugopalNo ratings yet
- Declaration of PassesDocument2 pagesDeclaration of PassesSSE OHE PSI CTYL SSE TRDNo ratings yet
- Joint Declaration For Name Change in PFDocument5 pagesJoint Declaration For Name Change in PFRashmi0% (1)
- 1677995328291esic and Uan For New JoinDocument7 pages1677995328291esic and Uan For New JoinALI ASGARNo ratings yet
- JD NewformatDocument1 pageJD Newformatsaravanakumar spNo ratings yet
- Declaration of Family MembersDocument4 pagesDeclaration of Family Membersanandpunna100% (1)
- GF PotatoDocument2 pagesGF PotatoChaitanya KvskNo ratings yet
- Joint Declaration by The Member and The EmployerDocument1 pageJoint Declaration by The Member and The EmployerSagar VasavaNo ratings yet
- SZABIST Fee Installment FormDocument2 pagesSZABIST Fee Installment FormMuhammad Tahir0% (1)
- PF Forms FormatsDocument10 pagesPF Forms FormatsSnehal ChauhanNo ratings yet
- Declaration For The Passes - 2024Document2 pagesDeclaration For The Passes - 2024Manohara BabuNo ratings yet
- ESP - Application FormDocument9 pagesESP - Application FormAbdul qadeerNo ratings yet
- PF No Break CertificateDocument1 pagePF No Break CertificateSagar Rajput100% (4)
- Formats Pensioners NHIS 2014Document4 pagesFormats Pensioners NHIS 2014Raj RudrapaaNo ratings yet
- NKF PD Application FormDocument10 pagesNKF PD Application FormSuesheena AliciaNo ratings yet
- Application For Financial Assistance For Undergraduate Studies in 2013Document6 pagesApplication For Financial Assistance For Undergraduate Studies in 2013211505006No ratings yet
- Diya Pakistan Registered: (Office Telephone Timings: 3:00pm To 5:00pm)Document12 pagesDiya Pakistan Registered: (Office Telephone Timings: 3:00pm To 5:00pm)Arsalan ArifNo ratings yet
- Form 2 RevisedDocument2 pagesForm 2 RevisedSatvik ManikanthNo ratings yet
- New EPF JD For Correction - PuneDocument1 pageNew EPF JD For Correction - Punesavan anvekarNo ratings yet
- APTF Pension Software by KSR - Trial VersionDocument29 pagesAPTF Pension Software by KSR - Trial Versionsrinivasa chary b86% (7)
- Nageena ESP - ApplicationFormDocument9 pagesNageena ESP - ApplicationFormDr. Inam Ullah WattooNo ratings yet
- Jioint Declaration FormDocument1 pageJioint Declaration FormRohit GuptaNo ratings yet
- Form 2Document92 pagesForm 2Bhattacharjee ShaibalNo ratings yet
- Joining Kit All FormsDocument13 pagesJoining Kit All FormsgopamaheshwariNo ratings yet
- SEED Application FormDocument4 pagesSEED Application FormPratik V PandhareNo ratings yet
- 002 - Employment Application Form (Rev 01)Document4 pages002 - Employment Application Form (Rev 01)Davylandon RubbinNo ratings yet
- New Starter FormDocument5 pagesNew Starter FormRajagopal BojanapalliNo ratings yet
- SuperannuationForms For IndividualDocument19 pagesSuperannuationForms For Individualkrishna kumarNo ratings yet
- Provident Fund Nomination Form-2 (Revised) - MarriedDocument3 pagesProvident Fund Nomination Form-2 (Revised) - MarriedSrihari ChaturvedulaNo ratings yet
- Application Forms For Admission in Class I Under SEEPin AEES 2015-16Document2 pagesApplication Forms For Admission in Class I Under SEEPin AEES 2015-16jlsinghNo ratings yet
- Joining FormDocument20 pagesJoining Formmansikapoor610No ratings yet
- Pass Declare 2023Document2 pagesPass Declare 2023Prabhu RadhaNo ratings yet
- New Application For Providing Dr. YSR Aarogyasri Health CardDocument2 pagesNew Application For Providing Dr. YSR Aarogyasri Health CardAswani TholchuriNo ratings yet
- Joint Declaration NewDocument1 pageJoint Declaration Newsarvang shahNo ratings yet
- Inclusivion of Child Name in Birth Certificate & ProcedureDocument2 pagesInclusivion of Child Name in Birth Certificate & Procedurebala bmeNo ratings yet
- Qarz e HasnaFormDocument12 pagesQarz e HasnaFormAli AbidNo ratings yet
- Application Form: Sggs Engineers' Alumni Association (Seaa)Document4 pagesApplication Form: Sggs Engineers' Alumni Association (Seaa)Priya BahetiNo ratings yet
- LHS ExemptionForm Final-1Document6 pagesLHS ExemptionForm Final-1rayghanaachmatNo ratings yet
- PF - Form 11Document2 pagesPF - Form 11Log SquareNo ratings yet
- Bay Family DeclarationDocument2 pagesBay Family DeclarationWASIMNo ratings yet
- Pension Papers Death After RetirementDocument17 pagesPension Papers Death After RetirementIjaz MaqboolNo ratings yet
- Income Details - (From All Sources)Document2 pagesIncome Details - (From All Sources)Aadi HilalNo ratings yet
- OutSourced Employee FormDocument2 pagesOutSourced Employee Formanilkc9No ratings yet
- Employment On Compassionate GroundsDocument12 pagesEmployment On Compassionate Groundshimadri_bhattacharjeNo ratings yet
- Application Form USAID Funded Merit & Need Based Scholarship For Regular Mba Students Seeking Admission in Fall 2014Document13 pagesApplication Form USAID Funded Merit & Need Based Scholarship For Regular Mba Students Seeking Admission in Fall 2014IrtizahussainNo ratings yet
- ESP - Application FormDocument9 pagesESP - Application FormgimagNo ratings yet
- Medical Fuel LTA and Telephone BillsDocument4 pagesMedical Fuel LTA and Telephone Billsabhi852004No ratings yet
- Irs Debtor Questionnaire 08 16Document4 pagesIrs Debtor Questionnaire 08 16api-326615022100% (1)
- Pen AppllicationDocument2 pagesPen AppllicationTagore NavabothuNo ratings yet
- Fin - e - 321 - 2019 - Pensiom GODocument32 pagesFin - e - 321 - 2019 - Pensiom GORytham Puni100% (2)
- Indian Bank - Education Loan Application FormDocument2 pagesIndian Bank - Education Loan Application Formabhishek100% (4)
- SssDocument46 pagesSsseyNo ratings yet
- Application Form - Kindergarten - Revised - 9jul09Document7 pagesApplication Form - Kindergarten - Revised - 9jul09inabansNo ratings yet
- IT Declaration Form 2014 15 - KreplDocument2 pagesIT Declaration Form 2014 15 - KreplGoyal AbhijeetNo ratings yet
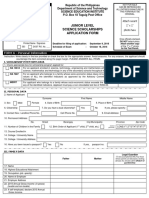
- Junior Level Science Scholarships Application Form: FORM A - Personal InformationDocument4 pagesJunior Level Science Scholarships Application Form: FORM A - Personal InformationAbigail SaballeNo ratings yet
- Tax Invoice: Bill From Invoice # CurrencyDocument1 pageTax Invoice: Bill From Invoice # CurrencyAnkur DuttaNo ratings yet
- Dos and Donts For CitizensDocument1 pageDos and Donts For CitizensAnkur DuttaNo ratings yet
- RBE No 80-2013Document6 pagesRBE No 80-2013Ankur DuttaNo ratings yet
- Mou 2004Document3 pagesMou 2004Ankur DuttaNo ratings yet
- Reimbursement of Cost of Spectacles Contact LenseDocument4 pagesReimbursement of Cost of Spectacles Contact LenseAnkur DuttaNo ratings yet