Download as docx, pdf, or txt
You might also like
- 2013 Spyder ST Owners ManualDocument171 pages2013 Spyder ST Owners ManualMelvin Quezada67% (6)
- NCP Excess Fluid VolumeDocument2 pagesNCP Excess Fluid VolumeMei Payumo100% (1)
- Fluid Volume ExcessDocument4 pagesFluid Volume ExcessTamil Villardo100% (2)
- Environmental Impact Assessment ModuleDocument39 pagesEnvironmental Impact Assessment ModuleJoshua Landoy100% (2)
- Fluid Volume Excess (CRF)Document4 pagesFluid Volume Excess (CRF)NursesLabs.com100% (1)
- NCP: Chronic Renal FailureDocument14 pagesNCP: Chronic Renal FailureJavie77% (13)
- Activity Intolerance Related To Decrease Blood FlowDocument3 pagesActivity Intolerance Related To Decrease Blood FlowDarkCeades100% (3)
- CKD NCPDocument2 pagesCKD NCPMark Angelo Chan100% (13)
- NCP - Fluid RetentionDocument3 pagesNCP - Fluid RetentionMichelle Teodoro100% (1)
- Decreased Cardiac OutputDocument9 pagesDecreased Cardiac OutputChinita Sangbaan75% (4)
- Assessment Diagnosis Planning Implementation Rationale EvaluationDocument3 pagesAssessment Diagnosis Planning Implementation Rationale Evaluationria_soriano_2No ratings yet
- Decreased Cardiac OutputDocument4 pagesDecreased Cardiac OutputChristine MatasNo ratings yet
- Impaired Physical Mobility Related To Neuromuscular ImpairmentDocument17 pagesImpaired Physical Mobility Related To Neuromuscular ImpairmentAileen Lopez83% (6)
- Nursing Care Plan Hemorrhagic StrokeDocument8 pagesNursing Care Plan Hemorrhagic StrokeJeffrey Dela Cruz50% (4)
- If Ye Know These Things Ross DrysdaleDocument334 pagesIf Ye Know These Things Ross DrysdaleBernardo Rasimo100% (1)
- NCP HemoDocument2 pagesNCP HemoJigs HechNo ratings yet
- Fluid Volume ExcessDocument2 pagesFluid Volume ExcessRodel Yacas100% (5)
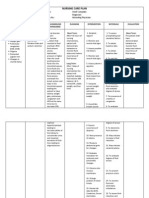
- Nursing Care PlanDocument2 pagesNursing Care PlanAldrein GonzalesNo ratings yet
- NCP CKDDocument9 pagesNCP CKDDanica Salinas100% (1)
- Ineffective Tissue PerfusionDocument1 pageIneffective Tissue PerfusionRhae RaynogNo ratings yet
- NCP EsrdDocument9 pagesNCP EsrdMarisol Dizon100% (1)
- Ineffective Renal Tissue PerfusionDocument2 pagesIneffective Renal Tissue PerfusionHendra Tanjung100% (4)
- Renal Failure NCPDocument3 pagesRenal Failure NCPJet Ray-Ann GaringanNo ratings yet
- Fluid Volume Excess Related To Decrease Glomerular Filtration Rate and Sodium RetentionDocument6 pagesFluid Volume Excess Related To Decrease Glomerular Filtration Rate and Sodium RetentionKristel Abe100% (1)
- NCP - Excess Fluid Volume (Aortic Stenosis)Document3 pagesNCP - Excess Fluid Volume (Aortic Stenosis)Daniel Vergara Arce100% (3)
- Ineffective Tissue PerfusionDocument4 pagesIneffective Tissue PerfusionClariz Basco100% (1)
- CRF Fluid Volume Excess NCPDocument3 pagesCRF Fluid Volume Excess NCPchubbielitaNo ratings yet
- NCP For CHF 3 Activity IntoleranceDocument2 pagesNCP For CHF 3 Activity IntoleranceAngelyn ArdinesNo ratings yet
- Chronic Renal Failure Nursing Care PlanDocument6 pagesChronic Renal Failure Nursing Care PlanRuva Oscass JimmyNo ratings yet
- Glaucoma NCPDocument4 pagesGlaucoma NCPChantal CaraganNo ratings yet
- NCP CKDDocument6 pagesNCP CKDBenjie Dimayacyac100% (2)
- Lumunok at Huminga, Nabibilaukan Din Ako Madalas" AsDocument4 pagesLumunok at Huminga, Nabibilaukan Din Ako Madalas" AsPatricia Ortega100% (1)
- HemodialysisDocument4 pagesHemodialysisJon Adam Bermudez SamatraNo ratings yet
- Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7Document2 pagesIneffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7dana100% (4)
- Ncp-Ineffective Tissue Perfusion (Aortic Stenosis)Document2 pagesNcp-Ineffective Tissue Perfusion (Aortic Stenosis)Daniel Vergara Arce67% (3)
- Acute Renal Failure Nursing Care PlanDocument4 pagesAcute Renal Failure Nursing Care PlanKrisianne Mae Lorenzo Francisco80% (5)
- NCP Near DrowningDocument1 pageNCP Near Drowningchristine louise bernardoNo ratings yet
- Activity Intolerance Related To AmeniaDocument1 pageActivity Intolerance Related To AmeniaSiti Syazana Mohamad MogriNo ratings yet
- Anemia NCPDocument20 pagesAnemia NCPNursidar Pascual Mukattil80% (5)
- Risk For Impaired Skin Integrity and Readiness For Enhanced PowerDocument3 pagesRisk For Impaired Skin Integrity and Readiness For Enhanced PowerdanaNo ratings yet
- A Renal Failure (NCP)Document2 pagesA Renal Failure (NCP)Julie Aranda Hapin100% (1)
- Liver NCPDocument5 pagesLiver NCPMerrill HansNo ratings yet
- NCP Heart FailureDocument11 pagesNCP Heart FailureaZhermAine100% (1)
- Nursing Care PlanDocument11 pagesNursing Care Planaycee0316100% (1)
- NCP For StrokeDocument4 pagesNCP For StrokeJASON OGALESCO100% (1)
- DM NCPDocument7 pagesDM NCPMichael Anthony Cardenas Macaballug67% (3)
- NCPDocument9 pagesNCPTracy Camille EscobarNo ratings yet
- NCP Tissue PerfusionDocument4 pagesNCP Tissue PerfusionLisa Tandog100% (1)
- Nursing Care Plan (NCP)Document3 pagesNursing Care Plan (NCP)Sha PinedaNo ratings yet
- NCP EsrdDocument9 pagesNCP EsrdWilmar AngeloNo ratings yet
- NCP - CapDocument4 pagesNCP - CapSherryNo ratings yet
- Heart Failure Care PlanDocument2 pagesHeart Failure Care PlanJonathon100% (1)
- Esrd NCPDocument7 pagesEsrd NCPSharmaine Camille de LeonNo ratings yet
- Assessment Diagnosis Inference Planning Interventions Evaluation SubjectiveDocument2 pagesAssessment Diagnosis Inference Planning Interventions Evaluation SubjectiveMikaela Carisse F. BalbonNo ratings yet
- Nursing Care Plan Neonatal PneumoniaDocument2 pagesNursing Care Plan Neonatal Pneumoniaderic93% (42)
- NCP - Risk For InfectionDocument2 pagesNCP - Risk For InfectionJet Bautista100% (1)
- Rubeola Update For Nurses: Infection PreventionDocument3 pagesRubeola Update For Nurses: Infection PreventionAnabelle ReyesNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationJamie Haravata0% (1)
- Risk For Infection - NCPDocument3 pagesRisk For Infection - NCPHamil BanagNo ratings yet
- RusheDocument1 pageRusheCallie ParkNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanJehan Lois QuinesNo ratings yet
- Drug Order Mechanism of Action Indications Contraindications Adverse Reactions NX Consideration Generic Name: Brand Name: DosageDocument2 pagesDrug Order Mechanism of Action Indications Contraindications Adverse Reactions NX Consideration Generic Name: Brand Name: DosageEdel MartinezNo ratings yet
- Data Nursing Diagnosis Scientific Rationale Objectives Intervention Rationale EvaluationDocument5 pagesData Nursing Diagnosis Scientific Rationale Objectives Intervention Rationale EvaluationsteffiNo ratings yet
- Abruptio Placenta FullDocument10 pagesAbruptio Placenta FullChester ManaloNo ratings yet
- Nursing Care Plan TBIDocument5 pagesNursing Care Plan TBIChester Manalo87% (15)
- Pathophysiology TBIDocument1 pagePathophysiology TBIChester ManaloNo ratings yet
- Pathophysiology of DM ESRD HPNDocument1 pagePathophysiology of DM ESRD HPNChester ManaloNo ratings yet
- Poster FinalDocument1 pagePoster FinalKrish vasisthaNo ratings yet
- In Re Plagiarism Case Against Justice Del CastilloDocument112 pagesIn Re Plagiarism Case Against Justice Del CastilloRaffyLaguesmaNo ratings yet
- Chaliyama Steel Plant-Rungta Mines Limited Hazard Identification & Risk AssessmentDocument3 pagesChaliyama Steel Plant-Rungta Mines Limited Hazard Identification & Risk AssessmentCPP EI DSpNo ratings yet
- Subdivision of LandDocument6 pagesSubdivision of Land林诗倩No ratings yet
- Stable Fixed Points of Card Trick FunctionsDocument10 pagesStable Fixed Points of Card Trick FunctionsDerekNo ratings yet
- EmpiricalBasis GottmanDocument10 pagesEmpiricalBasis GottmanMundoSinViolenciaNo ratings yet
- ACCA P5 Question 2 June 2013 QaDocument4 pagesACCA P5 Question 2 June 2013 QaFarhan AlchiNo ratings yet
- Consumer Protection Act - SeminarDocument16 pagesConsumer Protection Act - SeminarAbdul KhadeerNo ratings yet
- Research PaperDocument7 pagesResearch PaperHazirah AmniNo ratings yet
- Lawrance Africa Imagined in The Spanish Renaissance - Henry Thomas LectureDocument20 pagesLawrance Africa Imagined in The Spanish Renaissance - Henry Thomas LecturejlawranceNo ratings yet
- Introduction To Python For Science & Engineering: David J. PineDocument18 pagesIntroduction To Python For Science & Engineering: David J. PineWasimNo ratings yet
- N. Mixture, CombinationDocument2 pagesN. Mixture, CombinationYareniNo ratings yet
- MAD Practical 6Document15 pagesMAD Practical 6DIVYESH PATELNo ratings yet
- Comm 130 PortfolioDocument23 pagesComm 130 PortfolioSami MossNo ratings yet
- MalappuramDocument20 pagesMalappuramFayizNo ratings yet
- Oma TS MLP V3 - 2 20110719 ADocument128 pagesOma TS MLP V3 - 2 20110719 AkennychanklNo ratings yet
- Whittington 22e Solutions Manual Ch14Document14 pagesWhittington 22e Solutions Manual Ch14潘妍伶No ratings yet
- Application of Buoyancy-Power Generator For Compressed Air Energy Storage Using A Fluid-Air Displacement System - ScienceDirectDocument7 pagesApplication of Buoyancy-Power Generator For Compressed Air Energy Storage Using A Fluid-Air Displacement System - ScienceDirectJoel Stanley TylerNo ratings yet
- Dsm-5 Icd-10 HandoutDocument107 pagesDsm-5 Icd-10 HandoutAakanksha Verma100% (1)
- Cell Structure & Cell OrganisationDocument35 pagesCell Structure & Cell OrganisationNaida Mohd SalehNo ratings yet
- Ballistic - August September 2021Document168 pagesBallistic - August September 2021andrewrowe100% (2)
- HB-1193-006 HB PlasmidPurif 0723 WWDocument68 pagesHB-1193-006 HB PlasmidPurif 0723 WWDiana DiasNo ratings yet
- Offer For C Check On NT-495-MG Harbour Generator Engine Against Customer Job No. E20006Document1 pageOffer For C Check On NT-495-MG Harbour Generator Engine Against Customer Job No. E20006bkrNo ratings yet
- Drug Dosage and IV Rates Calculations PDFDocument6 pagesDrug Dosage and IV Rates Calculations PDFvarmaNo ratings yet
- PP QM Integration With PS MM FICODocument26 pagesPP QM Integration With PS MM FICOAshwini Harwale SonwaneNo ratings yet
- Vernacular Terms 2 PDFDocument3 pagesVernacular Terms 2 PDFsmmNo ratings yet
- ECDIS JRC JAN-7201-9201 Instruct Manual BasicDocument294 pagesECDIS JRC JAN-7201-9201 Instruct Manual BasicRanjeet singhNo ratings yet