Download as pdf or txt
You might also like
- ATLS Practice Test 2 Answers & ExplanationsDocument8 pagesATLS Practice Test 2 Answers & ExplanationsCarl Sars75% (4)
- School Health Policy in NigeriaDocument40 pagesSchool Health Policy in NigeriaMahalim Fivebuckets100% (5)
- Losing My ReligionDocument4 pagesLosing My ReligionMuhammad Reza100% (1)
- Acticide CL1: ® Technical InformationDocument2 pagesActicide CL1: ® Technical InformationОлександр МацукаNo ratings yet
- Emergency Surgery 2: Perforated Peptic UlcerDocument11 pagesEmergency Surgery 2: Perforated Peptic Ulcerjidottt kejedotNo ratings yet
- 6 Osteoporotic Fractures in Older Adults: Cathleen S. Colo N-EmericDocument12 pages6 Osteoporotic Fractures in Older Adults: Cathleen S. Colo N-EmericRafael CastellarNo ratings yet
- Blood Transfusion 2Document7 pagesBlood Transfusion 2omarragabselimNo ratings yet
- (HTTP://WWW - Who.int/bulletin/volumes/90/3/11-093732/en/) : Epidemiology of SurgeriesDocument3 pages(HTTP://WWW - Who.int/bulletin/volumes/90/3/11-093732/en/) : Epidemiology of SurgeriesJoy ChalisseryNo ratings yet
- Global Action On Patient SafetyDocument8 pagesGlobal Action On Patient SafetycynthiaNo ratings yet
- 2023 Article 13352Document9 pages2023 Article 13352Rubén LimaNo ratings yet
- Chugh 2013Document61 pagesChugh 2013dharsandipan86No ratings yet
- Late Immune Consequences of Combat Trauma: A Review of Trauma-Related Immune Dysfunction and Potential TherapiesDocument13 pagesLate Immune Consequences of Combat Trauma: A Review of Trauma-Related Immune Dysfunction and Potential TherapiesQariahMaulidiahAminNo ratings yet
- 14 - Towards Best Practice in Acute Stroke Care in Ghana A Survey of Hospital ServicesDocument11 pages14 - Towards Best Practice in Acute Stroke Care in Ghana A Survey of Hospital ServicesChristel CibalonzaNo ratings yet
- Research ProporsalDocument12 pagesResearch ProporsalStanley JuniorNo ratings yet
- 2017 Article 66Document8 pages2017 Article 66Zuhratul LathifaNo ratings yet
- Propofol-TIVA Versus Inhalational Anesthesia For Cancer SurgeryDocument9 pagesPropofol-TIVA Versus Inhalational Anesthesia For Cancer SurgerygonjdelzNo ratings yet
- JCO 2014 Ñamendys Silva 1169 70Document2 pagesJCO 2014 Ñamendys Silva 1169 70Eward Rod SalNo ratings yet
- Chest Masive TransfDocument16 pagesChest Masive TransfMacario Ismael Chavez CutzNo ratings yet
- Primary Care For Cancers - Epidemiology, Causes, Prevention and Classification - A Narrative ReviewDocument7 pagesPrimary Care For Cancers - Epidemiology, Causes, Prevention and Classification - A Narrative ReviewChew Boon HowNo ratings yet
- WFSA UpdateDocument60 pagesWFSA UpdateSyaiful FatahNo ratings yet
- Evaluation of Clotting Factor Activities Early After Severe Multiple Trauma and Their Correlation With Coagulation Tests and Clinical Data (2015)Document9 pagesEvaluation of Clotting Factor Activities Early After Severe Multiple Trauma and Their Correlation With Coagulation Tests and Clinical Data (2015)Dsm DsmNo ratings yet
- Early Surgery Confers One-Year Mortality Benefit in Hip-Fracture PatientsDocument12 pagesEarly Surgery Confers One-Year Mortality Benefit in Hip-Fracture PatientsMartin MontesNo ratings yet
- (Ghiduri) (Cancer) ACCP Diagnosis and Management of Lung Cancer - Evidence-Based GuidelinesDocument395 pages(Ghiduri) (Cancer) ACCP Diagnosis and Management of Lung Cancer - Evidence-Based GuidelinesMario AndersonNo ratings yet
- Arthroplasty TodayDocument4 pagesArthroplasty TodayCristina SavaNo ratings yet
- Survival Analysis and Mortality Predictors of Hospitalized Severe Burn Victims in A Malaysian Burns Intensive Care UnitDocument8 pagesSurvival Analysis and Mortality Predictors of Hospitalized Severe Burn Victims in A Malaysian Burns Intensive Care UnitKenjiNo ratings yet
- 10 Facts On Patient SafetyDocument3 pages10 Facts On Patient SafetySafiqulatif AbdillahNo ratings yet
- Splenectomy For Immune Thrombocytopenic Purpura: Surgery For The 21st CenturyDocument4 pagesSplenectomy For Immune Thrombocytopenic Purpura: Surgery For The 21st Centurykevin stefanoNo ratings yet
- En A10v16n3Document4 pagesEn A10v16n3Just MahasiswaNo ratings yet
- Challenges of Meeting Surgical Needs in The Developing WorldDocument4 pagesChallenges of Meeting Surgical Needs in The Developing WorldTheGongziNo ratings yet
- Picot Synthesis SummativeDocument14 pagesPicot Synthesis Summativeapi-259394980No ratings yet
- The Satisfactionof Patients On Maintenance Hemodialysis Concerning The Provided Nursing Care in Hemodialysis UnitsDocument11 pagesThe Satisfactionof Patients On Maintenance Hemodialysis Concerning The Provided Nursing Care in Hemodialysis Unitsbe a doctor for you Medical studentNo ratings yet
- End of The Road For Heparin Thromboprophylaxis 2016Document3 pagesEnd of The Road For Heparin Thromboprophylaxis 2016Michael FreudigerNo ratings yet
- Jurnal LainDocument22 pagesJurnal LainBudi ArsanaNo ratings yet
- Blood Transfusion in Critical Care: Giora Netzer, Richard P Dutton and John R HessDocument3 pagesBlood Transfusion in Critical Care: Giora Netzer, Richard P Dutton and John R Hessnevermore11No ratings yet
- Radiation Safety Paper Week 2Document4 pagesRadiation Safety Paper Week 2api-313040758No ratings yet
- Blunt Abdominal TraumaDocument8 pagesBlunt Abdominal TraumaYudis Wira PratamaNo ratings yet
- Pre Hos TraumaDocument11 pagesPre Hos TraumaGel OmugtongNo ratings yet
- Surgery Public Health and PakistanDocument10 pagesSurgery Public Health and PakistanFatima ColonelNo ratings yet
- Research Article: Risk Factors of Lymph Edema in Breast Cancer PatientsDocument8 pagesResearch Article: Risk Factors of Lymph Edema in Breast Cancer PatientsidaNo ratings yet
- Acute ProctitisDocument3 pagesAcute ProctitisAdreiTheTripleANo ratings yet
- Simou Non-Blood Medical Care in Gynecologic... (22051161) World J Surg Oncol 2011 9 142Document6 pagesSimou Non-Blood Medical Care in Gynecologic... (22051161) World J Surg Oncol 2011 9 142Walter Ramos TelesNo ratings yet
- 2016 Article 329Document6 pages2016 Article 329anon_242145531No ratings yet
- 31 - Can Older Adults Benefitfrom Smart Devices, Wearables, and Other DigitalHealth Options To EnhanceCardiac RehabilitationDocument9 pages31 - Can Older Adults Benefitfrom Smart Devices, Wearables, and Other DigitalHealth Options To EnhanceCardiac RehabilitationMariaNo ratings yet
- 1 s2.0 S0140673616314878 MainDocument1 page1 s2.0 S0140673616314878 MainAntzela MoumtziNo ratings yet
- Prevention of Gastric CancerDocument2 pagesPrevention of Gastric CancerAndhika Bintang MahardhikaNo ratings yet
- Anesthesia Needs Large International Clinical Trials: Mcmaster University, Ontario, CanadaDocument4 pagesAnesthesia Needs Large International Clinical Trials: Mcmaster University, Ontario, Canadaserena7205No ratings yet
- Damage Control Management y Polytrauma PatientDocument324 pagesDamage Control Management y Polytrauma PatientMauri ParadedaNo ratings yet
- Wound Management For The 21st Century: Combining Effectiveness and EfficiencyDocument11 pagesWound Management For The 21st Century: Combining Effectiveness and EfficiencyHeba VerebceanNo ratings yet
- IPHMILitRev V5.2Document5 pagesIPHMILitRev V5.2miguel angel camachoNo ratings yet
- Who 2016 PDFDocument2 pagesWho 2016 PDFRefialy WahyyNo ratings yet
- Malignidad Post TrasplanteDocument7 pagesMalignidad Post TrasplantePao MoralesNo ratings yet
- Sepsis 2016 PDFDocument10 pagesSepsis 2016 PDFRicardo Ortiz NovilloNo ratings yet
- Blood in TraumaDocument17 pagesBlood in TraumaEmtha SeeniNo ratings yet
- Noncompliance in Organ Transplant Recipients A Literature ReviewDocument5 pagesNoncompliance in Organ Transplant Recipients A Literature ReviewtkpmzasifNo ratings yet
- Critical Care for Potential Liver Transplant CandidatesFrom EverandCritical Care for Potential Liver Transplant CandidatesDmitri BezinoverNo ratings yet
- Patient Selection in Ambulatory Surgery: Jeremy Lermitte and Frances ChungDocument5 pagesPatient Selection in Ambulatory Surgery: Jeremy Lermitte and Frances ChungMartin Víctor Flores JimenezNo ratings yet
- Martin 2005Document23 pagesMartin 2005Petrucio Augusto SDNo ratings yet
- Jurnal Efusi Pleura MalignaDocument12 pagesJurnal Efusi Pleura MalignaAsyraf HabibieNo ratings yet
- Clinical Guide SEOM On Venous Thromboembolism in Cancer PatientsDocument12 pagesClinical Guide SEOM On Venous Thromboembolism in Cancer PatientsGaby ValenzuelaNo ratings yet
- 775 FullDocument9 pages775 FullidaNo ratings yet
- First Draft DVT ProphylaxisDocument6 pagesFirst Draft DVT ProphylaxisRundNo ratings yet
- Mortality and Infectious Complications of Therapeutic Endovascular Interventional Radiology: A Systematic and Meta-Analysis ProtocolDocument8 pagesMortality and Infectious Complications of Therapeutic Endovascular Interventional Radiology: A Systematic and Meta-Analysis ProtocolgtNo ratings yet
- Cancer Screening in the Developing World: Case Studies and Strategies from the FieldFrom EverandCancer Screening in the Developing World: Case Studies and Strategies from the FieldMadelon L. FinkelNo ratings yet
- Resident On Call PDFDocument143 pagesResident On Call PDFMuhammad RezaNo ratings yet
- Chapter 22: Lacerations and Scar Revision Terence M. Davidson Lacerations Wound ClassificationsDocument16 pagesChapter 22: Lacerations and Scar Revision Terence M. Davidson Lacerations Wound ClassificationsMuhammad RezaNo ratings yet
- The Four Imams by Muhammad Abu ZahraDocument3 pagesThe Four Imams by Muhammad Abu ZahraMuhammad RezaNo ratings yet
- Radical ReformDocument1 pageRadical ReformMuhammad RezaNo ratings yet
- Is The Bible The Word of God-718314Document37 pagesIs The Bible The Word of God-718314Muhammad RezaNo ratings yet
- The Four MadhabDocument1 pageThe Four MadhabMuhammad RezaNo ratings yet
- Tokyo Guideline 2018 - Cholecystitis (Small Size)Document69 pagesTokyo Guideline 2018 - Cholecystitis (Small Size)Muhammad RezaNo ratings yet
- Jurnal On Hand SurgeryDocument187 pagesJurnal On Hand SurgeryMuhammad RezaNo ratings yet
- Closed Reduction of Posterior Hip DislocationDocument4 pagesClosed Reduction of Posterior Hip DislocationMuhammad RezaNo ratings yet
- Amputation Guideline EN PDFDocument3 pagesAmputation Guideline EN PDFMuhammad RezaNo ratings yet
- Discipline Code and Student Behavioral Contract: Parent SectionDocument2 pagesDiscipline Code and Student Behavioral Contract: Parent Sectionsir jjNo ratings yet
- Lasso GBRDocument1 pageLasso GBRMohamedAtefNo ratings yet
- Rhinomicosis IndiaDocument4 pagesRhinomicosis IndiaLiz TorresNo ratings yet
- (Report) Medication ErrorDocument4 pages(Report) Medication ErrorJoyce TanNo ratings yet
- Illustrated Objective Toxicology For Veterinary Exams - (WWW - FreeBookBank.net) PDFDocument99 pagesIllustrated Objective Toxicology For Veterinary Exams - (WWW - FreeBookBank.net) PDFAshok BalwadaNo ratings yet
- Aesthetic Panchakarma KSR 2-2-13Document49 pagesAesthetic Panchakarma KSR 2-2-13Technoayurveda DrksrprasadNo ratings yet
- Course CatalogDocument456 pagesCourse CatalogIan Xavier GalloNo ratings yet
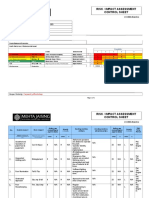
- Risk / Impact Assessment Control Sheet: CC/EHS/RA/014 ContractDocument4 pagesRisk / Impact Assessment Control Sheet: CC/EHS/RA/014 Contractsaurabh juwatkarNo ratings yet
- Clinical Practicum Worksheet: Nursing Care PlanDocument4 pagesClinical Practicum Worksheet: Nursing Care PlanOrlea Francisco-SisioNo ratings yet
- Specification - ISOMALT LM - V007Document4 pagesSpecification - ISOMALT LM - V007Hakan ÇİÇEKNo ratings yet
- 7 Day Intermittent Fasting Meal PlanDocument11 pages7 Day Intermittent Fasting Meal Plandietbykt.planshareNo ratings yet
- Soket ProstesisDocument7 pagesSoket ProstesisAnantaNo ratings yet
- Cloning Technology-Bane or Boon To MankindDocument52 pagesCloning Technology-Bane or Boon To MankindDevain AroraNo ratings yet
- Biofeedback Training For Enhanced Trading PerformanceDocument5 pagesBiofeedback Training For Enhanced Trading PerformancejNo ratings yet
- Reportpdf1 PDFDocument3 pagesReportpdf1 PDFLifetime AbbeyNo ratings yet
- Msds Citrapure - DryDocument2 pagesMsds Citrapure - DryKyle MccoyNo ratings yet
- Elektrokardiografi: DR - Dr. Zaenal Muttaqien Sofro,, AIFM, Sport & Circ - Med School of Medicine Gadjah Mada UniversityDocument71 pagesElektrokardiografi: DR - Dr. Zaenal Muttaqien Sofro,, AIFM, Sport & Circ - Med School of Medicine Gadjah Mada UniversityNadyaNo ratings yet
- Annotated BibliographyDocument14 pagesAnnotated BibliographyDrew TilleyNo ratings yet
- p450 Table Oct 11 2009Document2 pagesp450 Table Oct 11 2009Naresh BabuNo ratings yet
- EHS 085 General Security Procedure For Manufacturing Area SampleDocument3 pagesEHS 085 General Security Procedure For Manufacturing Area Samplerozario100% (1)
- Meniscus TearsDocument29 pagesMeniscus Tearsmaulana ilhamNo ratings yet
- Rituximab Protocol PDFDocument13 pagesRituximab Protocol PDFSenarathKuleeshaKodisinghe100% (1)
- Provincial Veterinary Office: Republic of The Philippines Province of CebuDocument2 pagesProvincial Veterinary Office: Republic of The Philippines Province of CebuKyle Dhon Estrera VelasquezNo ratings yet
- Polysomnograpy: Charmain Beatriz A. AtosDocument62 pagesPolysomnograpy: Charmain Beatriz A. AtosCharmain Beatriz Ayson Atos100% (2)
- Contoh Soal PG Bahasa Inggris Kelas XI Semester 1 K13 Beserta JawabanDocument12 pagesContoh Soal PG Bahasa Inggris Kelas XI Semester 1 K13 Beserta JawabanIntan Wahyu DhamayantiNo ratings yet
- Oldenburg Burnout Inventory ScoringDocument3 pagesOldenburg Burnout Inventory ScoringAnonymous 0uCHZz72vwNo ratings yet
- Hypernatremia: Kidney Case Conference: How I TreatDocument3 pagesHypernatremia: Kidney Case Conference: How I TreatJulian ViggianoNo ratings yet