
Allergic Conjunctivitis: A Comprehensive Review of The Literature
Allergic Conjunctivitis: A Comprehensive Review of The Literature
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Useful Vocabs For OET Writing & Speaking PDFDocument2 pagesUseful Vocabs For OET Writing & Speaking PDFLiju K Oommen100% (3)
- Building Plumbing Systems Design - (Lecture 01-Introduction)Document30 pagesBuilding Plumbing Systems Design - (Lecture 01-Introduction)محمد إسلام عبابنه100% (3)
- Drugs Acting On The Endocrine SystemDocument58 pagesDrugs Acting On The Endocrine SystemAmiel Francisco ReyesNo ratings yet
- Lapsus: (Report Subtitle)Document3 pagesLapsus: (Report Subtitle)Justy GuavaNo ratings yet
- Spontaneous Closure of Macular Holes Secondary To Posterior Uveitis: Case Series and A Literature ReviewDocument7 pagesSpontaneous Closure of Macular Holes Secondary To Posterior Uveitis: Case Series and A Literature ReviewJusty GuavaNo ratings yet
- Leaflet KatarakDocument5 pagesLeaflet KatarakJusty GuavaNo ratings yet
- FEES4Document115 pagesFEES4Justy Guava100% (1)
- FEES6Document36 pagesFEES6Justy GuavaNo ratings yet
- IndianJAnaesth5815-3581899 095658Document2 pagesIndianJAnaesth5815-3581899 095658Justy GuavaNo ratings yet
- Cover Journal ReadingDocument1 pageCover Journal ReadingJusty GuavaNo ratings yet
- Bab IiDocument1 pageBab IiJusty GuavaNo ratings yet
- Induction of Diabetes by Streptozotocin in RatsDocument5 pagesInduction of Diabetes by Streptozotocin in RatsJusty GuavaNo ratings yet
- Release Adrenalin Release Corticotro PinDocument1 pageRelease Adrenalin Release Corticotro PinJusty GuavaNo ratings yet
- PDF 9Document7 pagesPDF 9Justy GuavaNo ratings yet
- Daftar Pustaka: Research Bulletin 154: 5-21Document3 pagesDaftar Pustaka: Research Bulletin 154: 5-21Justy GuavaNo ratings yet
- Candida-Induced Oral Epithelial Cell Responses: E.A. Lilly, J.E. Leigh, S.H. Joseph, & P.L. Fidel JRDocument9 pagesCandida-Induced Oral Epithelial Cell Responses: E.A. Lilly, J.E. Leigh, S.H. Joseph, & P.L. Fidel JRJusty GuavaNo ratings yet
- PDF 8Document8 pagesPDF 8Justy GuavaNo ratings yet
- Wastewater Study GuideDocument46 pagesWastewater Study GuideManjunath NadarajanNo ratings yet
- Medication Reconcillation in Home Care Getting Started KitDocument74 pagesMedication Reconcillation in Home Care Getting Started Kitjopet8180No ratings yet
- ABC of Wound Healing WWW - Dof3tna - Net WWW - Egydr.com Drhamdy2009Document49 pagesABC of Wound Healing WWW - Dof3tna - Net WWW - Egydr.com Drhamdy2009steadiNo ratings yet
- Study of Some Biochemical Changes in Serum & Saliva PDFDocument254 pagesStudy of Some Biochemical Changes in Serum & Saliva PDFManisha SinghNo ratings yet
- Pathogenesis, Diagnosis, and Treatment of Lumbar Zygapophysial (Facet) Joint PainDocument6 pagesPathogenesis, Diagnosis, and Treatment of Lumbar Zygapophysial (Facet) Joint PainErika KusumawatiNo ratings yet
- Healing TouchDocument2 pagesHealing Touchdmarkee4No ratings yet
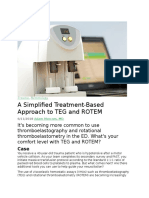
- A Simplified Treatment-Based Approach To TEG and ROTEMDocument7 pagesA Simplified Treatment-Based Approach To TEG and ROTEMCraigbud99No ratings yet
- Theobromine Inhibits CoughDocument16 pagesTheobromine Inhibits CoughRaffaello MobiliaNo ratings yet
- Bodyweight Torch Metabolic Workouts PDFDocument29 pagesBodyweight Torch Metabolic Workouts PDFyuretz100% (4)
- Effect of Preparation Processing On Foods and NutrientsDocument5 pagesEffect of Preparation Processing On Foods and Nutrientsapi-19768570No ratings yet
- Australian Ironman Magazine July 2016 PDFDocument140 pagesAustralian Ironman Magazine July 2016 PDFgeorgeNo ratings yet
- Neurological Assessment 1 - Assessing Level of ConsciousnessDocument1 pageNeurological Assessment 1 - Assessing Level of ConsciousnesskyawswakyawswaNo ratings yet
- Florida Nurse-Practice-ActDocument117 pagesFlorida Nurse-Practice-Actapi-251653314No ratings yet
- Iksir-e-Badan (Elixir) : Unique Influence From Unani Medicine - A ReviewDocument6 pagesIksir-e-Badan (Elixir) : Unique Influence From Unani Medicine - A ReviewAmjad NaseerNo ratings yet
- Wpt2011 Programme Final 20may Web VersionDocument226 pagesWpt2011 Programme Final 20may Web VersionEdgarAntenorLópez100% (1)
- Diabetes Mellitus RPTDocument17 pagesDiabetes Mellitus RPTMichael BoadoNo ratings yet
- Microalbuminuria As An Early Postoperative Detector of Sepsis After Major SurgeriesDocument7 pagesMicroalbuminuria As An Early Postoperative Detector of Sepsis After Major SurgeriesaliNo ratings yet
- Far Eastern University-Institute of Nursing In-House NursingDocument25 pagesFar Eastern University-Institute of Nursing In-House Nursingjonasdelacruz1111No ratings yet
- Dental Common Proposal TKDocument42 pagesDental Common Proposal TKTonderai KurewaNo ratings yet
- IMUNOterapi HCCDocument12 pagesIMUNOterapi HCCAri Dwi PrasetyoNo ratings yet
- Jurnal AklimatisasiDocument5 pagesJurnal AklimatisasiMelianaMogaYufitaNo ratings yet
- NCP DFDocument4 pagesNCP DFqweqweqweNo ratings yet
- Before and After The Haiti Earthquake An Interview With MSF Physician Dr. Wendy LaiDocument6 pagesBefore and After The Haiti Earthquake An Interview With MSF Physician Dr. Wendy LaiThavam RatnaNo ratings yet
- IWGDF Guidelines On The Prevention and Management of Diabetic Foot Disease 2019Document47 pagesIWGDF Guidelines On The Prevention and Management of Diabetic Foot Disease 2019Sidan EmozieNo ratings yet
- IMCIDocument11 pagesIMCIJoshua Villarba100% (1)
- Episode 242 PDFDocument25 pagesEpisode 242 PDFZeeshan KhanNo ratings yet
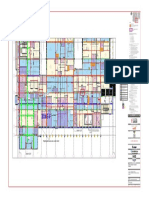
- OR4100-1-ATNM-AB4-SDW-00001-4A - Level-00-ZONE FDocument1 pageOR4100-1-ATNM-AB4-SDW-00001-4A - Level-00-ZONE FAhmed SolankiNo ratings yet


















































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Useful Vocabs For OET Writing & Speaking PDFDocument2 pagesUseful Vocabs For OET Writing & Speaking PDFLiju K Oommen100% (3)
- Building Plumbing Systems Design - (Lecture 01-Introduction)Document30 pagesBuilding Plumbing Systems Design - (Lecture 01-Introduction)محمد إسلام عبابنه100% (3)
- Drugs Acting On The Endocrine SystemDocument58 pagesDrugs Acting On The Endocrine SystemAmiel Francisco ReyesNo ratings yet
- Lapsus: (Report Subtitle)Document3 pagesLapsus: (Report Subtitle)Justy GuavaNo ratings yet
- Spontaneous Closure of Macular Holes Secondary To Posterior Uveitis: Case Series and A Literature ReviewDocument7 pagesSpontaneous Closure of Macular Holes Secondary To Posterior Uveitis: Case Series and A Literature ReviewJusty GuavaNo ratings yet
- Leaflet KatarakDocument5 pagesLeaflet KatarakJusty GuavaNo ratings yet
- FEES4Document115 pagesFEES4Justy Guava100% (1)
- FEES6Document36 pagesFEES6Justy GuavaNo ratings yet
- IndianJAnaesth5815-3581899 095658Document2 pagesIndianJAnaesth5815-3581899 095658Justy GuavaNo ratings yet
- Cover Journal ReadingDocument1 pageCover Journal ReadingJusty GuavaNo ratings yet
- Bab IiDocument1 pageBab IiJusty GuavaNo ratings yet
- Induction of Diabetes by Streptozotocin in RatsDocument5 pagesInduction of Diabetes by Streptozotocin in RatsJusty GuavaNo ratings yet
- Release Adrenalin Release Corticotro PinDocument1 pageRelease Adrenalin Release Corticotro PinJusty GuavaNo ratings yet
- PDF 9Document7 pagesPDF 9Justy GuavaNo ratings yet
- Daftar Pustaka: Research Bulletin 154: 5-21Document3 pagesDaftar Pustaka: Research Bulletin 154: 5-21Justy GuavaNo ratings yet
- Candida-Induced Oral Epithelial Cell Responses: E.A. Lilly, J.E. Leigh, S.H. Joseph, & P.L. Fidel JRDocument9 pagesCandida-Induced Oral Epithelial Cell Responses: E.A. Lilly, J.E. Leigh, S.H. Joseph, & P.L. Fidel JRJusty GuavaNo ratings yet
- PDF 8Document8 pagesPDF 8Justy GuavaNo ratings yet
- Wastewater Study GuideDocument46 pagesWastewater Study GuideManjunath NadarajanNo ratings yet
- Medication Reconcillation in Home Care Getting Started KitDocument74 pagesMedication Reconcillation in Home Care Getting Started Kitjopet8180No ratings yet
- ABC of Wound Healing WWW - Dof3tna - Net WWW - Egydr.com Drhamdy2009Document49 pagesABC of Wound Healing WWW - Dof3tna - Net WWW - Egydr.com Drhamdy2009steadiNo ratings yet
- Study of Some Biochemical Changes in Serum & Saliva PDFDocument254 pagesStudy of Some Biochemical Changes in Serum & Saliva PDFManisha SinghNo ratings yet
- Pathogenesis, Diagnosis, and Treatment of Lumbar Zygapophysial (Facet) Joint PainDocument6 pagesPathogenesis, Diagnosis, and Treatment of Lumbar Zygapophysial (Facet) Joint PainErika KusumawatiNo ratings yet
- Healing TouchDocument2 pagesHealing Touchdmarkee4No ratings yet
- A Simplified Treatment-Based Approach To TEG and ROTEMDocument7 pagesA Simplified Treatment-Based Approach To TEG and ROTEMCraigbud99No ratings yet
- Theobromine Inhibits CoughDocument16 pagesTheobromine Inhibits CoughRaffaello MobiliaNo ratings yet
- Bodyweight Torch Metabolic Workouts PDFDocument29 pagesBodyweight Torch Metabolic Workouts PDFyuretz100% (4)
- Effect of Preparation Processing On Foods and NutrientsDocument5 pagesEffect of Preparation Processing On Foods and Nutrientsapi-19768570No ratings yet
- Australian Ironman Magazine July 2016 PDFDocument140 pagesAustralian Ironman Magazine July 2016 PDFgeorgeNo ratings yet
- Neurological Assessment 1 - Assessing Level of ConsciousnessDocument1 pageNeurological Assessment 1 - Assessing Level of ConsciousnesskyawswakyawswaNo ratings yet
- Florida Nurse-Practice-ActDocument117 pagesFlorida Nurse-Practice-Actapi-251653314No ratings yet
- Iksir-e-Badan (Elixir) : Unique Influence From Unani Medicine - A ReviewDocument6 pagesIksir-e-Badan (Elixir) : Unique Influence From Unani Medicine - A ReviewAmjad NaseerNo ratings yet
- Wpt2011 Programme Final 20may Web VersionDocument226 pagesWpt2011 Programme Final 20may Web VersionEdgarAntenorLópez100% (1)
- Diabetes Mellitus RPTDocument17 pagesDiabetes Mellitus RPTMichael BoadoNo ratings yet
- Microalbuminuria As An Early Postoperative Detector of Sepsis After Major SurgeriesDocument7 pagesMicroalbuminuria As An Early Postoperative Detector of Sepsis After Major SurgeriesaliNo ratings yet
- Far Eastern University-Institute of Nursing In-House NursingDocument25 pagesFar Eastern University-Institute of Nursing In-House Nursingjonasdelacruz1111No ratings yet
- Dental Common Proposal TKDocument42 pagesDental Common Proposal TKTonderai KurewaNo ratings yet
- IMUNOterapi HCCDocument12 pagesIMUNOterapi HCCAri Dwi PrasetyoNo ratings yet
- Jurnal AklimatisasiDocument5 pagesJurnal AklimatisasiMelianaMogaYufitaNo ratings yet
- NCP DFDocument4 pagesNCP DFqweqweqweNo ratings yet
- Before and After The Haiti Earthquake An Interview With MSF Physician Dr. Wendy LaiDocument6 pagesBefore and After The Haiti Earthquake An Interview With MSF Physician Dr. Wendy LaiThavam RatnaNo ratings yet
- IWGDF Guidelines On The Prevention and Management of Diabetic Foot Disease 2019Document47 pagesIWGDF Guidelines On The Prevention and Management of Diabetic Foot Disease 2019Sidan EmozieNo ratings yet
- IMCIDocument11 pagesIMCIJoshua Villarba100% (1)
- Episode 242 PDFDocument25 pagesEpisode 242 PDFZeeshan KhanNo ratings yet
- OR4100-1-ATNM-AB4-SDW-00001-4A - Level-00-ZONE FDocument1 pageOR4100-1-ATNM-AB4-SDW-00001-4A - Level-00-ZONE FAhmed SolankiNo ratings yet