
Management of Duodenal Trauma: Review
Management of Duodenal Trauma: Review
You might also like
- Post Test 5Document18 pagesPost Test 5amarisanti98% (49)
- AtlsDocument9 pagesAtlsabjah100% (1)
- Abdominal TraumaDocument52 pagesAbdominal TraumaDONALD UNASHENo ratings yet
- Jay Patrick Vitamin C ArticlesDocument63 pagesJay Patrick Vitamin C ArticlesKrys Weaver0% (1)
- Management of Duodenal Trauma: Chinese Journal of Traumatology (English Edition) February 2011Document5 pagesManagement of Duodenal Trauma: Chinese Journal of Traumatology (English Edition) February 2011dr muddssar sattarNo ratings yet
- Evaluation and Management of Splenic Injury in Blunt Abdominal TraumaDocument32 pagesEvaluation and Management of Splenic Injury in Blunt Abdominal TraumaImam Hakim SuryonoNo ratings yet
- Multilevel Duodenal Injury After Blunt TraumaDocument5 pagesMultilevel Duodenal Injury After Blunt TraumaHanny RusliNo ratings yet
- WES GuidelineDocument28 pagesWES Guidelinesolo surgical forumNo ratings yet
- Surgicalmanagementof Abdominaltrauma: Hollow Viscus InjuryDocument11 pagesSurgicalmanagementof Abdominaltrauma: Hollow Viscus Injurysyairodhi rodziNo ratings yet
- Blunt Abdominal Trauma: Severity Factors in Hollow Viscus InjuriesDocument4 pagesBlunt Abdominal Trauma: Severity Factors in Hollow Viscus InjuriesRajan KarmakarNo ratings yet
- A1504050119 PDFDocument19 pagesA1504050119 PDFImam Hakim SuryonoNo ratings yet
- Trauma ColonDocument7 pagesTrauma Colonricardo arreguiNo ratings yet
- Posterior Urethral Valves (PUV) - Children's Hospital of PhiladelphiaDocument5 pagesPosterior Urethral Valves (PUV) - Children's Hospital of PhiladelphiaAndri Feisal NasutionNo ratings yet
- V23I2 05 FREE DrChouhan PDFDocument7 pagesV23I2 05 FREE DrChouhan PDFBimo PramestaNo ratings yet
- The Management of Pancreatic Injuries: JEJ Krige, E Jonas, SR Thomson and SJ BeningfieldDocument11 pagesThe Management of Pancreatic Injuries: JEJ Krige, E Jonas, SR Thomson and SJ BeningfieldHenry Espinoz ChavNo ratings yet
- EScholarship UC Item 14n977sgDocument7 pagesEScholarship UC Item 14n977sgcindyamandaNo ratings yet
- Urological Injuries During Colorectal SurgeryDocument8 pagesUrological Injuries During Colorectal Surgeryfatima chrystelle nuñalNo ratings yet
- Tbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite: DOI: 10.1590/S0100-69912014000300016Document4 pagesTbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite: DOI: 10.1590/S0100-69912014000300016Hanny RusliNo ratings yet
- American College of Surgeons (ACS)Document8 pagesAmerican College of Surgeons (ACS)perkakas78No ratings yet
- Duodenal Trauma: Luke R Johnston, Gary Wind and Matthew J BradleyDocument9 pagesDuodenal Trauma: Luke R Johnston, Gary Wind and Matthew J BradleyHenry Espinoz ChavNo ratings yet
- Abdomen CerradoDocument32 pagesAbdomen CerradoNina JácomeNo ratings yet
- B - Bile Duct Injuries in The Era of Laparoscopic Cholecystectomies - 2010Document16 pagesB - Bile Duct Injuries in The Era of Laparoscopic Cholecystectomies - 2010Battousaih1No ratings yet
- Management of Duodenal InjuriesDocument11 pagesManagement of Duodenal InjuriesZam HusNo ratings yet
- 1 PB PDFDocument11 pages1 PB PDFTheodore LiwonganNo ratings yet
- Abdomen TraumaDocument74 pagesAbdomen TraumajeevanNo ratings yet
- Pancreatic TraumaDocument11 pagesPancreatic TraumaAriniDwiYulianNo ratings yet
- Rhode Island Hospital: Related Emedicine TopicsDocument6 pagesRhode Island Hospital: Related Emedicine TopicsApril Shane OreiroNo ratings yet
- Erik Pancreatic TraumaDocument31 pagesErik Pancreatic TraumaIgnatius JesinNo ratings yet
- Complicationsafter Pancreaticoduodenectomy: Robert SimonDocument10 pagesComplicationsafter Pancreaticoduodenectomy: Robert SimonŞükriye AngaNo ratings yet
- Clinical Review: Modern Management of Splenic TraumaDocument7 pagesClinical Review: Modern Management of Splenic TraumaputraNo ratings yet
- Diagnosis and Treatment of Perforated or Bleeding Peptic Ulcers 2013 WSES PositionDocument15 pagesDiagnosis and Treatment of Perforated or Bleeding Peptic Ulcers 2013 WSES PositionDauz ArashNo ratings yet
- 1757 7241 17 13 PDFDocument5 pages1757 7241 17 13 PDFzafira anandaNo ratings yet
- DPLDocument5 pagesDPLngenevaNo ratings yet
- Peitzman Trauma HepáticoDocument11 pagesPeitzman Trauma HepáticoLety Carmona ArevaloNo ratings yet
- Blunt Abdominal TraumaDocument24 pagesBlunt Abdominal TraumaDen SinyoNo ratings yet
- 3Document8 pages3polomska.kmNo ratings yet
- Gastroduodenal PerforationDocument4 pagesGastroduodenal PerforationMaresp21No ratings yet
- Abdominal TraumaDocument10 pagesAbdominal TraumadeddybedahmksNo ratings yet
- Editorial - Operative Strategies in Pancreatic Trauma - Keep It Safe and SimpleDocument4 pagesEditorial - Operative Strategies in Pancreatic Trauma - Keep It Safe and SimpleFauz RamadhanNo ratings yet
- 1 s2.0 S2213576621002050 MainDocument6 pages1 s2.0 S2213576621002050 MainHusnul HanifaNo ratings yet
- Jiang 2012Document9 pagesJiang 2012DH SiriruiNo ratings yet
- 10 Yang Sebenarnya PDFDocument29 pages10 Yang Sebenarnya PDFSriarbiatiNo ratings yet
- Delayed Presentation of Isolated Jejunal Perforation Following Accidental TraumaDocument2 pagesDelayed Presentation of Isolated Jejunal Perforation Following Accidental TraumapricillyaNo ratings yet
- Operative Management of Anastomotic Leaks After Colorectal SurgeryDocument6 pagesOperative Management of Anastomotic Leaks After Colorectal SurgeryJorge OsorioNo ratings yet
- Current Therapy of Trauma and Surgical Critical CareDocument4 pagesCurrent Therapy of Trauma and Surgical Critical CareAgung TananNo ratings yet
- Duodenal Injuries ReviewDocument7 pagesDuodenal Injuries Revieweztouch12No ratings yet
- Art TH 2012Document9 pagesArt TH 2012Pamela ParedesNo ratings yet
- Current Management of Hepatic TraumaDocument11 pagesCurrent Management of Hepatic TraumaPerla RuizNo ratings yet
- 3 BaruDocument17 pages3 BaruAnditha Namira RSNo ratings yet
- Challenges in The Maagement of Pancreatic and Duodenal InjuriesDocument6 pagesChallenges in The Maagement of Pancreatic and Duodenal InjuriesOpl OplNo ratings yet
- Via BiliarDocument7 pagesVia Biliarahs ahnNo ratings yet
- Duodenal Injuries: E. Degiannis and K. BoffardDocument7 pagesDuodenal Injuries: E. Degiannis and K. BoffardDaniel Suarez ParapatNo ratings yet
- Abdominal Trauma, PenetratingDocument10 pagesAbdominal Trauma, PenetratingdeddybedahmksNo ratings yet
- Kumar - Burst Abdomen Related Factor and Postoperative Challenge For SurgeonsDocument5 pagesKumar - Burst Abdomen Related Factor and Postoperative Challenge For Surgeonsrhyzik reeNo ratings yet
- TraumaDocument10 pagesTraumaIda_Maryani94No ratings yet
- Renal Trauma Medscape PDFDocument21 pagesRenal Trauma Medscape PDFPatricia Prabawati LCNo ratings yet
- Duodenal Injuries: E. Degiannis and K. BoffardDocument7 pagesDuodenal Injuries: E. Degiannis and K. BoffardriftaNo ratings yet
- Analysis of Risk Factors For Postoperative Morbidity in Perforated Peptic UlcerDocument10 pagesAnalysis of Risk Factors For Postoperative Morbidity in Perforated Peptic UlcerNurul Fitrawati RidwanNo ratings yet
- GuidelinesDocument26 pagesGuidelinesmsc3nNo ratings yet
- Ab PenetranteDocument29 pagesAb PenetranteNina JácomeNo ratings yet
- Classification and Management of Bile Duct Injuries: EditorialDocument6 pagesClassification and Management of Bile Duct Injuries: EditorialSINAN SHAWKATNo ratings yet
- Anatomy. Eight Edition. Saint Louis: Mosby.: Ped PDFDocument10 pagesAnatomy. Eight Edition. Saint Louis: Mosby.: Ped PDFannisa ussalihahNo ratings yet
- Case Studies of Postoperative Complications after Digestive SurgeryFrom EverandCase Studies of Postoperative Complications after Digestive SurgeryNo ratings yet
- Leg or Foot Amputation Pref CardDocument2 pagesLeg or Foot Amputation Pref CardPerrilyn PereyNo ratings yet
- Anamesis & Fisis BedahDocument15 pagesAnamesis & Fisis BedahIriamana Liasyarah MarudinNo ratings yet
- Chest and Abdominal Injuries: Forensic Medicine by Yazan AbueidehDocument54 pagesChest and Abdominal Injuries: Forensic Medicine by Yazan AbueidehRayyan Alali100% (1)
- TecarDocument9 pagesTecarMarco PastoreNo ratings yet
- 9-12 BurnsDocument32 pages9-12 BurnsralukNo ratings yet
- Basic Clinical SkillsDocument15 pagesBasic Clinical SkillsPriza RazunipNo ratings yet
- HemoperitoneumDocument14 pagesHemoperitoneumMiguel MuunguiiaNo ratings yet
- TrumaDocument13 pagesTrumaShrestha Anjiv100% (1)
- Research Paper RaptorDocument3 pagesResearch Paper Raptorapi-318114801No ratings yet
- National Registry Skill SheetsDocument21 pagesNational Registry Skill SheetsKemzo AbarquezNo ratings yet
- Trauma Triad of DeathDocument5 pagesTrauma Triad of DeathTomNo ratings yet
- TLS Chapter1Document27 pagesTLS Chapter1TeojNo ratings yet
- PJ Medical HandbookDocument210 pagesPJ Medical HandbookJared A. Lang100% (3)
- Recognition & Treatment of Pneumothorax Hemothorax, Flail Chest, Stove in ChestDocument59 pagesRecognition & Treatment of Pneumothorax Hemothorax, Flail Chest, Stove in ChestAnusha VergheseNo ratings yet
- Accident and Emergency MedicineDocument391 pagesAccident and Emergency MedicineKhalid Labadi100% (7)
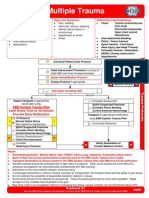
- Multiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationDocument1 pageMultiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationKelly JacksonNo ratings yet
- Primary SurveyDocument25 pagesPrimary Surveyapi-98304344No ratings yet
- Fire Works InjuryDocument39 pagesFire Works Injurynnaesor_1091No ratings yet
- 1 Early Management of Trauma Patient in The HospitalDocument23 pages1 Early Management of Trauma Patient in The HospitalkgnmatinNo ratings yet
- Zygomatic Bone FracturesDocument5 pagesZygomatic Bone FracturesAgung SajaNo ratings yet
- Abdominal Ultrasound Is An Unreliable Modality For The Detection of Hemoperitoneum in Patients With Pelvic FractureDocument6 pagesAbdominal Ultrasound Is An Unreliable Modality For The Detection of Hemoperitoneum in Patients With Pelvic FractureEvelyn GrandaNo ratings yet
- Chemical Eye Injuries PDFDocument4 pagesChemical Eye Injuries PDFGeraldine TGNo ratings yet
- Emergensi Urologi UiiDocument83 pagesEmergensi Urologi UiitrianaamaliaNo ratings yet
- Clinical Skill Handout Forensic Medicine and MedicolegalDocument20 pagesClinical Skill Handout Forensic Medicine and MedicolegalCici MutiaNo ratings yet
- Preparation of The Resuscitation Room and PatientDocument7 pagesPreparation of The Resuscitation Room and PatientRaydoon SadeqNo ratings yet
- AllRefer Health - PerichondritisDocument2 pagesAllRefer Health - PerichondritisandosaputraNo ratings yet
- Disaster Management Plan: Sir J.J. Group of Hospitals, MumbaiDocument100 pagesDisaster Management Plan: Sir J.J. Group of Hospitals, MumbaiektapatelbmsNo ratings yet
























































































Download as pdf or txt
You might also like
- Post Test 5Document18 pagesPost Test 5amarisanti98% (49)
- AtlsDocument9 pagesAtlsabjah100% (1)
- Abdominal TraumaDocument52 pagesAbdominal TraumaDONALD UNASHENo ratings yet
- Jay Patrick Vitamin C ArticlesDocument63 pagesJay Patrick Vitamin C ArticlesKrys Weaver0% (1)
- Management of Duodenal Trauma: Chinese Journal of Traumatology (English Edition) February 2011Document5 pagesManagement of Duodenal Trauma: Chinese Journal of Traumatology (English Edition) February 2011dr muddssar sattarNo ratings yet
- Evaluation and Management of Splenic Injury in Blunt Abdominal TraumaDocument32 pagesEvaluation and Management of Splenic Injury in Blunt Abdominal TraumaImam Hakim SuryonoNo ratings yet
- Multilevel Duodenal Injury After Blunt TraumaDocument5 pagesMultilevel Duodenal Injury After Blunt TraumaHanny RusliNo ratings yet
- WES GuidelineDocument28 pagesWES Guidelinesolo surgical forumNo ratings yet
- Surgicalmanagementof Abdominaltrauma: Hollow Viscus InjuryDocument11 pagesSurgicalmanagementof Abdominaltrauma: Hollow Viscus Injurysyairodhi rodziNo ratings yet
- Blunt Abdominal Trauma: Severity Factors in Hollow Viscus InjuriesDocument4 pagesBlunt Abdominal Trauma: Severity Factors in Hollow Viscus InjuriesRajan KarmakarNo ratings yet
- A1504050119 PDFDocument19 pagesA1504050119 PDFImam Hakim SuryonoNo ratings yet
- Trauma ColonDocument7 pagesTrauma Colonricardo arreguiNo ratings yet
- Posterior Urethral Valves (PUV) - Children's Hospital of PhiladelphiaDocument5 pagesPosterior Urethral Valves (PUV) - Children's Hospital of PhiladelphiaAndri Feisal NasutionNo ratings yet
- V23I2 05 FREE DrChouhan PDFDocument7 pagesV23I2 05 FREE DrChouhan PDFBimo PramestaNo ratings yet
- The Management of Pancreatic Injuries: JEJ Krige, E Jonas, SR Thomson and SJ BeningfieldDocument11 pagesThe Management of Pancreatic Injuries: JEJ Krige, E Jonas, SR Thomson and SJ BeningfieldHenry Espinoz ChavNo ratings yet
- EScholarship UC Item 14n977sgDocument7 pagesEScholarship UC Item 14n977sgcindyamandaNo ratings yet
- Urological Injuries During Colorectal SurgeryDocument8 pagesUrological Injuries During Colorectal Surgeryfatima chrystelle nuñalNo ratings yet
- Tbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite: DOI: 10.1590/S0100-69912014000300016Document4 pagesTbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite Tbe-Cite: DOI: 10.1590/S0100-69912014000300016Hanny RusliNo ratings yet
- American College of Surgeons (ACS)Document8 pagesAmerican College of Surgeons (ACS)perkakas78No ratings yet
- Duodenal Trauma: Luke R Johnston, Gary Wind and Matthew J BradleyDocument9 pagesDuodenal Trauma: Luke R Johnston, Gary Wind and Matthew J BradleyHenry Espinoz ChavNo ratings yet
- Abdomen CerradoDocument32 pagesAbdomen CerradoNina JácomeNo ratings yet
- B - Bile Duct Injuries in The Era of Laparoscopic Cholecystectomies - 2010Document16 pagesB - Bile Duct Injuries in The Era of Laparoscopic Cholecystectomies - 2010Battousaih1No ratings yet
- Management of Duodenal InjuriesDocument11 pagesManagement of Duodenal InjuriesZam HusNo ratings yet
- 1 PB PDFDocument11 pages1 PB PDFTheodore LiwonganNo ratings yet
- Abdomen TraumaDocument74 pagesAbdomen TraumajeevanNo ratings yet
- Pancreatic TraumaDocument11 pagesPancreatic TraumaAriniDwiYulianNo ratings yet
- Rhode Island Hospital: Related Emedicine TopicsDocument6 pagesRhode Island Hospital: Related Emedicine TopicsApril Shane OreiroNo ratings yet
- Erik Pancreatic TraumaDocument31 pagesErik Pancreatic TraumaIgnatius JesinNo ratings yet
- Complicationsafter Pancreaticoduodenectomy: Robert SimonDocument10 pagesComplicationsafter Pancreaticoduodenectomy: Robert SimonŞükriye AngaNo ratings yet
- Clinical Review: Modern Management of Splenic TraumaDocument7 pagesClinical Review: Modern Management of Splenic TraumaputraNo ratings yet
- Diagnosis and Treatment of Perforated or Bleeding Peptic Ulcers 2013 WSES PositionDocument15 pagesDiagnosis and Treatment of Perforated or Bleeding Peptic Ulcers 2013 WSES PositionDauz ArashNo ratings yet
- 1757 7241 17 13 PDFDocument5 pages1757 7241 17 13 PDFzafira anandaNo ratings yet
- DPLDocument5 pagesDPLngenevaNo ratings yet
- Peitzman Trauma HepáticoDocument11 pagesPeitzman Trauma HepáticoLety Carmona ArevaloNo ratings yet
- Blunt Abdominal TraumaDocument24 pagesBlunt Abdominal TraumaDen SinyoNo ratings yet
- 3Document8 pages3polomska.kmNo ratings yet
- Gastroduodenal PerforationDocument4 pagesGastroduodenal PerforationMaresp21No ratings yet
- Abdominal TraumaDocument10 pagesAbdominal TraumadeddybedahmksNo ratings yet
- Editorial - Operative Strategies in Pancreatic Trauma - Keep It Safe and SimpleDocument4 pagesEditorial - Operative Strategies in Pancreatic Trauma - Keep It Safe and SimpleFauz RamadhanNo ratings yet
- 1 s2.0 S2213576621002050 MainDocument6 pages1 s2.0 S2213576621002050 MainHusnul HanifaNo ratings yet
- Jiang 2012Document9 pagesJiang 2012DH SiriruiNo ratings yet
- 10 Yang Sebenarnya PDFDocument29 pages10 Yang Sebenarnya PDFSriarbiatiNo ratings yet
- Delayed Presentation of Isolated Jejunal Perforation Following Accidental TraumaDocument2 pagesDelayed Presentation of Isolated Jejunal Perforation Following Accidental TraumapricillyaNo ratings yet
- Operative Management of Anastomotic Leaks After Colorectal SurgeryDocument6 pagesOperative Management of Anastomotic Leaks After Colorectal SurgeryJorge OsorioNo ratings yet
- Current Therapy of Trauma and Surgical Critical CareDocument4 pagesCurrent Therapy of Trauma and Surgical Critical CareAgung TananNo ratings yet
- Duodenal Injuries ReviewDocument7 pagesDuodenal Injuries Revieweztouch12No ratings yet
- Art TH 2012Document9 pagesArt TH 2012Pamela ParedesNo ratings yet
- Current Management of Hepatic TraumaDocument11 pagesCurrent Management of Hepatic TraumaPerla RuizNo ratings yet
- 3 BaruDocument17 pages3 BaruAnditha Namira RSNo ratings yet
- Challenges in The Maagement of Pancreatic and Duodenal InjuriesDocument6 pagesChallenges in The Maagement of Pancreatic and Duodenal InjuriesOpl OplNo ratings yet
- Via BiliarDocument7 pagesVia Biliarahs ahnNo ratings yet
- Duodenal Injuries: E. Degiannis and K. BoffardDocument7 pagesDuodenal Injuries: E. Degiannis and K. BoffardDaniel Suarez ParapatNo ratings yet
- Abdominal Trauma, PenetratingDocument10 pagesAbdominal Trauma, PenetratingdeddybedahmksNo ratings yet
- Kumar - Burst Abdomen Related Factor and Postoperative Challenge For SurgeonsDocument5 pagesKumar - Burst Abdomen Related Factor and Postoperative Challenge For Surgeonsrhyzik reeNo ratings yet
- TraumaDocument10 pagesTraumaIda_Maryani94No ratings yet
- Renal Trauma Medscape PDFDocument21 pagesRenal Trauma Medscape PDFPatricia Prabawati LCNo ratings yet
- Duodenal Injuries: E. Degiannis and K. BoffardDocument7 pagesDuodenal Injuries: E. Degiannis and K. BoffardriftaNo ratings yet
- Analysis of Risk Factors For Postoperative Morbidity in Perforated Peptic UlcerDocument10 pagesAnalysis of Risk Factors For Postoperative Morbidity in Perforated Peptic UlcerNurul Fitrawati RidwanNo ratings yet
- GuidelinesDocument26 pagesGuidelinesmsc3nNo ratings yet
- Ab PenetranteDocument29 pagesAb PenetranteNina JácomeNo ratings yet
- Classification and Management of Bile Duct Injuries: EditorialDocument6 pagesClassification and Management of Bile Duct Injuries: EditorialSINAN SHAWKATNo ratings yet
- Anatomy. Eight Edition. Saint Louis: Mosby.: Ped PDFDocument10 pagesAnatomy. Eight Edition. Saint Louis: Mosby.: Ped PDFannisa ussalihahNo ratings yet
- Case Studies of Postoperative Complications after Digestive SurgeryFrom EverandCase Studies of Postoperative Complications after Digestive SurgeryNo ratings yet
- Leg or Foot Amputation Pref CardDocument2 pagesLeg or Foot Amputation Pref CardPerrilyn PereyNo ratings yet
- Anamesis & Fisis BedahDocument15 pagesAnamesis & Fisis BedahIriamana Liasyarah MarudinNo ratings yet
- Chest and Abdominal Injuries: Forensic Medicine by Yazan AbueidehDocument54 pagesChest and Abdominal Injuries: Forensic Medicine by Yazan AbueidehRayyan Alali100% (1)
- TecarDocument9 pagesTecarMarco PastoreNo ratings yet
- 9-12 BurnsDocument32 pages9-12 BurnsralukNo ratings yet
- Basic Clinical SkillsDocument15 pagesBasic Clinical SkillsPriza RazunipNo ratings yet
- HemoperitoneumDocument14 pagesHemoperitoneumMiguel MuunguiiaNo ratings yet
- TrumaDocument13 pagesTrumaShrestha Anjiv100% (1)
- Research Paper RaptorDocument3 pagesResearch Paper Raptorapi-318114801No ratings yet
- National Registry Skill SheetsDocument21 pagesNational Registry Skill SheetsKemzo AbarquezNo ratings yet
- Trauma Triad of DeathDocument5 pagesTrauma Triad of DeathTomNo ratings yet
- TLS Chapter1Document27 pagesTLS Chapter1TeojNo ratings yet
- PJ Medical HandbookDocument210 pagesPJ Medical HandbookJared A. Lang100% (3)
- Recognition & Treatment of Pneumothorax Hemothorax, Flail Chest, Stove in ChestDocument59 pagesRecognition & Treatment of Pneumothorax Hemothorax, Flail Chest, Stove in ChestAnusha VergheseNo ratings yet
- Accident and Emergency MedicineDocument391 pagesAccident and Emergency MedicineKhalid Labadi100% (7)
- Multiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationDocument1 pageMultiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationKelly JacksonNo ratings yet
- Primary SurveyDocument25 pagesPrimary Surveyapi-98304344No ratings yet
- Fire Works InjuryDocument39 pagesFire Works Injurynnaesor_1091No ratings yet
- 1 Early Management of Trauma Patient in The HospitalDocument23 pages1 Early Management of Trauma Patient in The HospitalkgnmatinNo ratings yet
- Zygomatic Bone FracturesDocument5 pagesZygomatic Bone FracturesAgung SajaNo ratings yet
- Abdominal Ultrasound Is An Unreliable Modality For The Detection of Hemoperitoneum in Patients With Pelvic FractureDocument6 pagesAbdominal Ultrasound Is An Unreliable Modality For The Detection of Hemoperitoneum in Patients With Pelvic FractureEvelyn GrandaNo ratings yet
- Chemical Eye Injuries PDFDocument4 pagesChemical Eye Injuries PDFGeraldine TGNo ratings yet
- Emergensi Urologi UiiDocument83 pagesEmergensi Urologi UiitrianaamaliaNo ratings yet
- Clinical Skill Handout Forensic Medicine and MedicolegalDocument20 pagesClinical Skill Handout Forensic Medicine and MedicolegalCici MutiaNo ratings yet
- Preparation of The Resuscitation Room and PatientDocument7 pagesPreparation of The Resuscitation Room and PatientRaydoon SadeqNo ratings yet
- AllRefer Health - PerichondritisDocument2 pagesAllRefer Health - PerichondritisandosaputraNo ratings yet
- Disaster Management Plan: Sir J.J. Group of Hospitals, MumbaiDocument100 pagesDisaster Management Plan: Sir J.J. Group of Hospitals, MumbaiektapatelbmsNo ratings yet