Download as pptx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Musculoskeletal SystemDocument56 pagesThe Musculoskeletal SystemMaria Dini AdmiratiNo ratings yet
- Rangkuman Week 3 (PBL) - RADocument27 pagesRangkuman Week 3 (PBL) - RAMaria Dini AdmiratiNo ratings yet
- Week 1 HumanAnat&Fisio - 6 Agustus 2012Document17 pagesWeek 1 HumanAnat&Fisio - 6 Agustus 2012Maria Dini AdmiratiNo ratings yet
- Week 2 Blpressoureoduph - 20 Februari 2012week 2 Blpressoureoduph - 20 Februari 2012Document43 pagesWeek 2 Blpressoureoduph - 20 Februari 2012week 2 Blpressoureoduph - 20 Februari 2012Maria Dini AdmiratiNo ratings yet
- Week 1 BlockMuscle - 6 Agustus 2012Document21 pagesWeek 1 BlockMuscle - 6 Agustus 2012Maria Dini AdmiratiNo ratings yet
- Rangkuman Week 5 (PBL) - OsteomyelitisDocument9 pagesRangkuman Week 5 (PBL) - OsteomyelitisMaria Dini AdmiratiNo ratings yet
- Week 3 JointInflammatoryDisease - 27 Agustus 2012Document19 pagesWeek 3 JointInflammatoryDisease - 27 Agustus 2012Maria Dini AdmiratiNo ratings yet
- Week 4 BackBoneAnatomy - 3 September 2012Document20 pagesWeek 4 BackBoneAnatomy - 3 September 2012Maria Dini AdmiratiNo ratings yet
- Week 4 MetabolicBoneDisease - 3 September 2012week 4 MetabolicBoneDisease - 3 September 2012Document16 pagesWeek 4 MetabolicBoneDisease - 3 September 2012week 4 MetabolicBoneDisease - 3 September 2012Maria Dini AdmiratiNo ratings yet
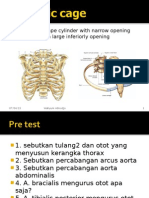
- Is An Irregular Shape Cylinder With Narrow Opening Superiorly and A Large Inferiorly OpeningDocument27 pagesIs An Irregular Shape Cylinder With Narrow Opening Superiorly and A Large Inferiorly OpeningMaria Dini AdmiratiNo ratings yet
- Heat Related Illnesses: Erwin Mulyawan, DR, Span, DpbaDocument42 pagesHeat Related Illnesses: Erwin Mulyawan, DR, Span, DpbaMaria Dini AdmiratiNo ratings yet
- Communication Between Nerve Cells.: V. Sutarmo SetiadjiDocument35 pagesCommunication Between Nerve Cells.: V. Sutarmo SetiadjiMaria Dini AdmiratiNo ratings yet
- Week 4 Embryology Development of Gastrointestinal: DR Marselina TanDocument29 pagesWeek 4 Embryology Development of Gastrointestinal: DR Marselina TanMaria Dini AdmiratiNo ratings yet
- Bones: A Hard SubjectDocument16 pagesBones: A Hard SubjectMaria Dini AdmiratiNo ratings yet
- Penyuluhan Pencegahan Penyakit Tuberkulosis (TBC) Era New NormalDocument8 pagesPenyuluhan Pencegahan Penyakit Tuberkulosis (TBC) Era New NormalTrihandi PamungkasNo ratings yet
- Drug Resistant TuberculosisDocument94 pagesDrug Resistant Tuberculosistummalapalli venkateswara raoNo ratings yet
- MycobacteriumDocument14 pagesMycobacteriumLuqman Al-Bashir FauziNo ratings yet
- Deteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Document8 pagesDeteksi Mycobacterium Tuberculosis Pada Sampel Sputum Menggunakan Teknik Loop-Mediated Isothermal Amplification (LAMP-TB)Anonymous iJc2y0No ratings yet
- Jasmin 1Document22 pagesJasmin 1angel angelNo ratings yet
- 017 - Revised PDFDocument9 pages017 - Revised PDFAdityaNo ratings yet
- CIAVDocument5 pagesCIAVAdolfo KwanNo ratings yet
- Multidrug-Resistant Tuberculosis: Agus Suharto BasukiDocument45 pagesMultidrug-Resistant Tuberculosis: Agus Suharto BasukidrhendraagusNo ratings yet
- 1ST Quarter 2013 TBL Reports Deder WoredaDocument58 pages1ST Quarter 2013 TBL Reports Deder WoredaEbsa MohammedNo ratings yet
- Jurnal Ilmiah Maksitek ISSN. 2655-4399 Vol. 5 No. 4 Desember 2020Document6 pagesJurnal Ilmiah Maksitek ISSN. 2655-4399 Vol. 5 No. 4 Desember 2020MasithaNo ratings yet
- Daftar PustakaDocument6 pagesDaftar PustakaChintiaNo ratings yet
- Daftar Harga VaksinDocument1 pageDaftar Harga VaksinIF RS Surya AsihNo ratings yet
- Pelaksanaan Promosi Kesehatan Dalam Penanggulangan Penyakit TuberkulosisDocument7 pagesPelaksanaan Promosi Kesehatan Dalam Penanggulangan Penyakit Tuberkulosiskalkun ingNo ratings yet
- Naskah PublikasiDocument10 pagesNaskah PublikasiSarah Certainly' CleverNo ratings yet
- Buku Panduan TBDocument111 pagesBuku Panduan TBwidia mujtiawatiNo ratings yet
- Marrow UpdatesDocument9 pagesMarrow UpdatesVirat KohliNo ratings yet
- Jurnal Reading TBCDocument19 pagesJurnal Reading TBCnikiNo ratings yet
- Istc 2014Document67 pagesIstc 2014Rosy KusumaNo ratings yet
- List TB Screening ClinicsDocument2 pagesList TB Screening ClinicsArvind K VinayakNo ratings yet
- (MDR-TB) Di Indonesia: Tinjauan Sistematik: Faktor Keberhasilan Pengobatan Multi Drug Resistance TuberculosaDocument7 pages(MDR-TB) Di Indonesia: Tinjauan Sistematik: Faktor Keberhasilan Pengobatan Multi Drug Resistance TuberculosaAngieNo ratings yet
- Rsau Dr.M. Salamun: Jadwal DokterDocument3 pagesRsau Dr.M. Salamun: Jadwal DokterFuad alfathanahNo ratings yet
- Drug Resistance TB Mono Drug Resistant TBDocument2 pagesDrug Resistance TB Mono Drug Resistant TBMalavath PavithranNo ratings yet
- gramPosOrganisms PDFDocument1 pagegramPosOrganisms PDFPurple basket100% (1)
- ID Perbandingan Pemeriksaan ToksigenisitasDocument9 pagesID Perbandingan Pemeriksaan ToksigenisitasindahdwirahNo ratings yet
- Pedoman Nasional Pengendalian TuberkulosisDocument111 pagesPedoman Nasional Pengendalian TuberkulosisYusriNo ratings yet
- PSmarkup - Revisi 1 TeshalonicaDocument28 pagesPSmarkup - Revisi 1 TeshalonicaBrian TonioNo ratings yet
- Tata Laksana TB MDR Dr. PrayudiDocument58 pagesTata Laksana TB MDR Dr. PrayudiDeaNo ratings yet
- Genus Mycobacterium by Dr. MesolaDocument79 pagesGenus Mycobacterium by Dr. MesolaDegee GonzalesNo ratings yet
- National Anti-TB Drug Resistance SurveyDocument36 pagesNational Anti-TB Drug Resistance Surveydr satnam kaurNo ratings yet
- MDR TB Made EasyDocument58 pagesMDR TB Made EasyNezly IderusNo ratings yet