Download as ppt, pdf, or txt
You might also like
- MCQ Review 2Document76 pagesMCQ Review 2Kholoud Almaabdi0% (1)
- Ruminant Digestive System PPT PresDocument11 pagesRuminant Digestive System PPT Pressophie67% (3)
- Bowel PreparationDocument16 pagesBowel PreparationKateAngeliRebosuraNo ratings yet
- Modul F2 Science C2Document14 pagesModul F2 Science C2NorelyanaAli67% (3)
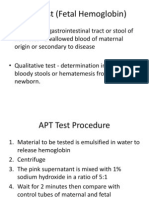
- APT Test (Fetal Hemoglobin)Document11 pagesAPT Test (Fetal Hemoglobin)Diovic TanNo ratings yet
- The Human Digestive System:: Its Functions, Stages, and The Pathway of FoodDocument15 pagesThe Human Digestive System:: Its Functions, Stages, and The Pathway of FoodMichelle Casayuran - Regala100% (2)
- Digestive System Lesson PlanDocument8 pagesDigestive System Lesson PlanLester Eslava Orpilla50% (2)
- Jha2 2 118Document3 pagesJha2 2 118Renato DantasNo ratings yet
- MD MCQ NewDocument109 pagesMD MCQ Newhimantha20059918100% (5)
- Oncologic Emergencies: Greg V. MansonDocument43 pagesOncologic Emergencies: Greg V. Mansonalarajpoetry100% (2)
- Inbound 988634411507331531Document7 pagesInbound 988634411507331531Jeannelle Landiza AmeninNo ratings yet
- Acute PancreatitisDocument48 pagesAcute PancreatitisapocruNo ratings yet
- InjuryDocument50 pagesInjuryRenaldas AugulisNo ratings yet
- Acute Pancreatitis: Tim Pieh, MDDocument48 pagesAcute Pancreatitis: Tim Pieh, MDSamina GulNo ratings yet
- Trauma Pancreas ManagementDocument20 pagesTrauma Pancreas Managementazis aimaduddinNo ratings yet
- 11.21.07 Necrotizing Fasciitis RavanosDocument16 pages11.21.07 Necrotizing Fasciitis RavanosMarc OnitosNo ratings yet
- 19Document3 pages19Elizabeth ToapantaNo ratings yet
- A 26-Year-Old White Man With A Systemic Lupus Erythematosus Flare and Acute Multiorgan Ischemia: Vasculitis or Thrombosis?Document9 pagesA 26-Year-Old White Man With A Systemic Lupus Erythematosus Flare and Acute Multiorgan Ischemia: Vasculitis or Thrombosis?Wendy SetiawanNo ratings yet
- Letter To The Editor Henoch-Schönlein Purpura in Adults: Clinics 2008 63 (2) :273-6Document4 pagesLetter To The Editor Henoch-Schönlein Purpura in Adults: Clinics 2008 63 (2) :273-6donkeyendutNo ratings yet
- (Doi 10.1089/neu.2014.3497) A. D. Sauerbeck J. L. Laws V. v. Bandaru P. G. Popovich N. J - Spinal Cord Injury Causes Chronic Liver Pathology in RatsDocument11 pages(Doi 10.1089/neu.2014.3497) A. D. Sauerbeck J. L. Laws V. v. Bandaru P. G. Popovich N. J - Spinal Cord Injury Causes Chronic Liver Pathology in RatsDitaIsnainiNo ratings yet
- Lascano, Joanne Alyssa - RheumatologyDocument13 pagesLascano, Joanne Alyssa - RheumatologyJoanne Alyssa Hernandez LascanoNo ratings yet
- Losifina Giannakikou - Hyperkalemia and Elective Cataract Surgery (Autosaved)Document30 pagesLosifina Giannakikou - Hyperkalemia and Elective Cataract Surgery (Autosaved)Pooja PoojaNo ratings yet
- Acute Pancreatitis 2012Document36 pagesAcute Pancreatitis 2012Alex TofanNo ratings yet
- Faintuch2006 Article RhabdomyolysisAfterGastricBypaDocument5 pagesFaintuch2006 Article RhabdomyolysisAfterGastricBypaRamyNo ratings yet
- Acute Kidney InjuryDocument42 pagesAcute Kidney Injurymedpedshospitalist100% (1)
- Pancreatic DiseasesDocument21 pagesPancreatic DiseasesRidwan kalibNo ratings yet
- CPC PancreatitisDocument67 pagesCPC PancreatitisM. Baidar SaeedNo ratings yet
- Manajemen Pasien CKD Di Instalasi Gawat DaruratDocument48 pagesManajemen Pasien CKD Di Instalasi Gawat DaruratUmar MukhNo ratings yet
- CBM 11 02 134 1 PDFDocument5 pagesCBM 11 02 134 1 PDFSipkhotunWindayaniNo ratings yet
- Lactate Use in Dem: Praneel Kumar Bundaberg Emergency DepartmentDocument19 pagesLactate Use in Dem: Praneel Kumar Bundaberg Emergency DepartmentPraneel KumarNo ratings yet
- Acute Pancreatitis by DR DilmoDocument50 pagesAcute Pancreatitis by DR Dilmosinan kNo ratings yet
- Liver and BiliaryDocument247 pagesLiver and BiliarySimionescu FlorentinaNo ratings yet
- Who Was Hilidanus: A. AdegbesanDocument31 pagesWho Was Hilidanus: A. AdegbesanUloko ChristopherNo ratings yet
- Acute Pancreatitis: Presented By: DAHAL SHIRISHADocument25 pagesAcute Pancreatitis: Presented By: DAHAL SHIRISHASiruNo ratings yet
- Cancer - June 1979 - Diasio - Adenocarcinoma of The Pancreas Associated With Hypoglycemia Case Report and Review of TheDocument8 pagesCancer - June 1979 - Diasio - Adenocarcinoma of The Pancreas Associated With Hypoglycemia Case Report and Review of Theabdullah shamshirNo ratings yet
- 5.15 SepsisDocument44 pages5.15 SepsisOnSolomonNo ratings yet
- Diabetes Mellitus Directs NKT Cells Toward Type 2 and Regulatory PhenotypeDocument7 pagesDiabetes Mellitus Directs NKT Cells Toward Type 2 and Regulatory PhenotypefragaNo ratings yet
- IT 9 - Arthritis in SLE - HMSDocument38 pagesIT 9 - Arthritis in SLE - HMSRurie Awalia Suhardi0% (1)
- Acute Abdominal Pain: A Practical ApproachDocument32 pagesAcute Abdominal Pain: A Practical ApproachWiwin SyaifudinNo ratings yet
- MR GastroDocument31 pagesMR GastroAdefuye AbiolaNo ratings yet
- A Case of Emphysematous Pyelonephritis: Grand RoundDocument3 pagesA Case of Emphysematous Pyelonephritis: Grand RoundEriet HidayatNo ratings yet
- Syok Hipovolemik PerbaikanDocument24 pagesSyok Hipovolemik Perbaikanyoelpurnama1991No ratings yet
- CholecystitisDocument48 pagesCholecystitisP Michael AwuyNo ratings yet
- Febrile Neutropenia Final 7-29Document74 pagesFebrile Neutropenia Final 7-29Juliyanti FuNo ratings yet
- Cholangitis and Cholecystitis (DR - Dr. Hery Djagat Purnomo, SpPD-KGEH)Document47 pagesCholangitis and Cholecystitis (DR - Dr. Hery Djagat Purnomo, SpPD-KGEH)Aditya SahidNo ratings yet
- RevisionLevel 3 SectionB MedSurge Case Study2Document113 pagesRevisionLevel 3 SectionB MedSurge Case Study2Milagros FloritaNo ratings yet
- Acute Liver Failure in Dengue Shock SyndromeDocument3 pagesAcute Liver Failure in Dengue Shock SyndromeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- KROK 2 1 профиль (315 Q 2004-2005)Document54 pagesKROK 2 1 профиль (315 Q 2004-2005)Ali ZeeshanNo ratings yet
- Thoracic Cancer - 2016 - Zhang - Ectopic Cushing Syndrome in Small Cell Lung Cancer A Case Report and Literature ReviewDocument4 pagesThoracic Cancer - 2016 - Zhang - Ectopic Cushing Syndrome in Small Cell Lung Cancer A Case Report and Literature ReviewandresconcilionNo ratings yet
- Post Polypectomy Electrocoagulation Syndrome A Rare Cause of Acute Abdominal PainDocument5 pagesPost Polypectomy Electrocoagulation Syndrome A Rare Cause of Acute Abdominal PainCom DigfulNo ratings yet
- Acute Pyelonephritis in Adults: A Case Series of 223 PatientsDocument6 pagesAcute Pyelonephritis in Adults: A Case Series of 223 PatientsshiaNo ratings yet
- General Pathology 2nd BM Neoplasia Blood Vessel Cardiovascular Pathology Pulmonary PathologyDocument64 pagesGeneral Pathology 2nd BM Neoplasia Blood Vessel Cardiovascular Pathology Pulmonary PathologyCherry RahimaNo ratings yet
- Case StudiesDocument6 pagesCase StudiesPatricia CruzNo ratings yet
- Renal FailureDocument31 pagesRenal Failureapi-195799092No ratings yet
- Rheumatic Fever and Rheumatic Heart DiseaseDocument132 pagesRheumatic Fever and Rheumatic Heart DiseaseDamie FernandezNo ratings yet
- DC ExerciseDocument3 pagesDC Exercisetaylors versionNo ratings yet
- Poliadenitis NodosaDocument5 pagesPoliadenitis NodosaRicardo Uzcategui ArreguiNo ratings yet
- Journal of DiabetesDocument6 pagesJournal of DiabetesSartika Rizky HapsariNo ratings yet
- Hepatology - 1983 - Viola - Exudative Ascites in The Course of Acute Type B HepatitisDocument3 pagesHepatology - 1983 - Viola - Exudative Ascites in The Course of Acute Type B HepatitisAudryaNo ratings yet
- Am J Surg 2004 p463Document4 pagesAm J Surg 2004 p463olivia magdalenaNo ratings yet
- NBME 2 Block 1-4 All IncludedDocument112 pagesNBME 2 Block 1-4 All Included3592648No ratings yet
- Case 1Document4 pagesCase 1Irsanti SasmitaNo ratings yet
- PancreatitisDocument59 pagesPancreatitisAarif RanaNo ratings yet
- Clinical Pancreatology: For Practising Gastroenterologists and SurgeonsFrom EverandClinical Pancreatology: For Practising Gastroenterologists and SurgeonsJuan Enrique Dominguez-MunozNo ratings yet
- Subtotal Cholecystectomy-''Fenestrating'' Vs ''Reconstituting'' Subtypes and The Prevention of Bile Duct Injury - Definition of The Optimal Procedure In  Difficult Operative ConditionsDocument8 pagesSubtotal Cholecystectomy-''Fenestrating'' Vs ''Reconstituting'' Subtypes and The Prevention of Bile Duct Injury - Definition of The Optimal Procedure In  Difficult Operative ConditionsBolivar Isea100% (1)
- 1.study of Physiological Functions of Digestive System of Farm AnimalsDocument58 pages1.study of Physiological Functions of Digestive System of Farm AnimalsKashifNo ratings yet
- Indications and Complications of ErcpDocument57 pagesIndications and Complications of ErcpNuha AL-YousfiNo ratings yet
- What Are The Types of EndosDocument3 pagesWhat Are The Types of EndosSailu KatragaddaNo ratings yet
- Crohn's: Mucosal FeaturesDocument10 pagesCrohn's: Mucosal Featuresالقناة الرسمية للشيخ عادل ريانNo ratings yet
- Anatomy and Physiologi PF The Digestive TractDocument11 pagesAnatomy and Physiologi PF The Digestive Tractrahtu suzi ameliaNo ratings yet
- Rat DissectionDocument5 pagesRat DissectionAcidri AbdulkarimNo ratings yet
- Classifications of Esophagitis: Who Needs Them?Document5 pagesClassifications of Esophagitis: Who Needs Them?Amanda SaphiraNo ratings yet
- Acute Cholangitis Clinical Presentation - History, Physical, CausesDocument3 pagesAcute Cholangitis Clinical Presentation - History, Physical, Causesm.m.m.mNo ratings yet
- Choledocholithiasis - Clinical Manifestations, Diagnosis, and Management - UpToDateDocument19 pagesCholedocholithiasis - Clinical Manifestations, Diagnosis, and Management - UpToDateFeer VillarrealNo ratings yet
- Astro Diagnosis VirgoDocument42 pagesAstro Diagnosis VirgoOvn Murthy100% (1)
- Normal Flora of Gastrointestinal TractDocument6 pagesNormal Flora of Gastrointestinal TractjoganksNo ratings yet
- Ezzat PaperDocument15 pagesEzzat PaperMohamedAbdelmonaemNo ratings yet
- Surgical JaundiceDocument35 pagesSurgical JaundiceIbsa ShumaNo ratings yet
- Stoma Care BasicsDocument83 pagesStoma Care BasicsTeoh HsNo ratings yet
- Ulcerative ColitisDocument18 pagesUlcerative ColitisKyle Ü D. CunanersNo ratings yet
- Clinical Case: Acute Pancreatitis: Teacher: Arestegui Aguirre Diana LuzDocument13 pagesClinical Case: Acute Pancreatitis: Teacher: Arestegui Aguirre Diana LuzGrimilda PobleteNo ratings yet
- Lower GI BleedingDocument40 pagesLower GI BleedingMohammad Firdaus100% (2)
- Micro Teaching On Colitis: School of Nursing Science and Research Sharda UniversityDocument21 pagesMicro Teaching On Colitis: School of Nursing Science and Research Sharda UniversityPooja SahuNo ratings yet
- Gall Bladder and Bile DuctDocument18 pagesGall Bladder and Bile DuctClint MorrisonNo ratings yet
- Digestion PDFDocument3 pagesDigestion PDFAnonymous uAtcDMeo1No ratings yet
- Antaomy of GITDocument5 pagesAntaomy of GITMike GNo ratings yet
- Q2 - Parts and Functions of The Digestive SystemDocument3 pagesQ2 - Parts and Functions of The Digestive SystemEden BorjaNo ratings yet
- Nutrition in Animals - MCQDocument14 pagesNutrition in Animals - MCQMinuteBrain LearningNo ratings yet