
Know Common Disease Management
Know Common Disease Management
You might also like
- Heart Failure Topic DiscussionDocument11 pagesHeart Failure Topic Discussionapi-665372449No ratings yet
- Antibiotic Mixing Chart With SAMF InfoDocument8 pagesAntibiotic Mixing Chart With SAMF Infosumayyah995No ratings yet
- EKG RhythmsDocument10 pagesEKG RhythmsQueenNo ratings yet
- Antiarrhythmic Medication Chart - EBM Consult v3Document2 pagesAntiarrhythmic Medication Chart - EBM Consult v3Linlin100% (1)
- Diabetes Topic DiscussionDocument9 pagesDiabetes Topic DiscussionSamNo ratings yet
- A Drug For IntDocument58 pagesA Drug For IntVajirawit PetchsriNo ratings yet
- Calculations IDocument17 pagesCalculations INisreen SalameNo ratings yet
- Noradrenaline Infusion Rate BSUH Critical CareDocument4 pagesNoradrenaline Infusion Rate BSUH Critical CareAndreiCostei100% (1)
- Antihyperglycemic Agents Comparison Chart PDFDocument9 pagesAntihyperglycemic Agents Comparison Chart PDFconcoz100% (1)
- Acute MedicineDocument54 pagesAcute MedicineTipuNo ratings yet
- Spinal Cord CompressionDocument4 pagesSpinal Cord Compressionian3yeung-2No ratings yet
- Essenc I Al TherapyDocument9 pagesEssenc I Al TherapyFabian Ramirez HincapiéNo ratings yet
- OTC Pain Relievers Dosage Chart For Adults and Children 12 Years and OlderDocument2 pagesOTC Pain Relievers Dosage Chart For Adults and Children 12 Years and OlderAdocueNo ratings yet
- NOAC ChartDocument2 pagesNOAC Chartsgod34No ratings yet
- Review Handouts For Medical Pharmacology PDFDocument21 pagesReview Handouts For Medical Pharmacology PDFAndres F. TorresNo ratings yet
- DrugsDocument155 pagesDrugsAkankshaNo ratings yet
- Pharmacology of Cardiac Diseases MINEDocument3 pagesPharmacology of Cardiac Diseases MINEMitu Miressa تNo ratings yet
- Malaria Treatment IndiaDocument1 pageMalaria Treatment IndiaSubzer OmerNo ratings yet
- 2015 Pain Management For PediatricDocument2 pages2015 Pain Management For Pediatricdiany astutiNo ratings yet
- OTC Labels HorizontalDocument1 pageOTC Labels HorizontalTsoojiNo ratings yet
- C. Anti-Hypertensive Drugs.Document10 pagesC. Anti-Hypertensive Drugs.Nabeel AsifNo ratings yet
- IV PO Conversion CAPDocument3 pagesIV PO Conversion CAPdamondouglasNo ratings yet
- Pedia Stickers PDFDocument8 pagesPedia Stickers PDFAshNo ratings yet
- Ans 2 PDFDocument101 pagesAns 2 PDFrab yoNo ratings yet
- Antibiotic IV Administration During COVID-19Document5 pagesAntibiotic IV Administration During COVID-19David Hines LopezNo ratings yet
- Drug Side EffectsDocument2 pagesDrug Side EffectsAngelic khanNo ratings yet
- Insulin Chart: Insulin Type Onset of Action Peak Duration of ActionDocument1 pageInsulin Chart: Insulin Type Onset of Action Peak Duration of ActionGeorge ZachariahNo ratings yet
- Critical Care Drugs 2Document23 pagesCritical Care Drugs 2Asri Ernadi100% (1)
- Vancomycin Protocol RQHRDocument15 pagesVancomycin Protocol RQHRl1o2stNo ratings yet
- Prefix Suffix MnemonicsDocument5 pagesPrefix Suffix MnemonicsPj MontecilloNo ratings yet
- Drug Interactions: What Is An Interaction?Document4 pagesDrug Interactions: What Is An Interaction?Leyla MajundaNo ratings yet
- Summary of Antidiabetic Drugs PDFDocument3 pagesSummary of Antidiabetic Drugs PDFZinc YuloNo ratings yet
- Drug Card Emergency Department-1 PDFDocument2 pagesDrug Card Emergency Department-1 PDFdrmohdtanveerNo ratings yet
- Finished Ekg Study GuideDocument4 pagesFinished Ekg Study Guideapi-652914452No ratings yet
- Emergency Drugs: Drug Action Indications Adverse Effects Contraindications Nursing Management Atropine SulfateDocument15 pagesEmergency Drugs: Drug Action Indications Adverse Effects Contraindications Nursing Management Atropine Sulfate092109No ratings yet
- Review Handouts For Medical Pharmacology: Terriann Crisp, PH.DDocument28 pagesReview Handouts For Medical Pharmacology: Terriann Crisp, PH.Dmus zaharaNo ratings yet
- Drug ListsDocument10 pagesDrug ListsAmber Merritt100% (1)
- All Types of InsulinDocument18 pagesAll Types of Insulinali mohammedNo ratings yet
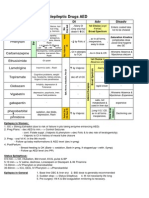
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 pageAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88No ratings yet
- Antibiotic Sensitivity FINAL V4 Sheet1Document1 pageAntibiotic Sensitivity FINAL V4 Sheet1JHNo ratings yet
- Neonate: TPR of Newborns BW 1500gDocument9 pagesNeonate: TPR of Newborns BW 1500gAnne Lorraine BringasNo ratings yet
- Smart Pumps Adult ITU Library v3Document73 pagesSmart Pumps Adult ITU Library v3Aqsa Ahmed SiddiquiNo ratings yet
- Total Pharmacy Notes TPN For EEDocument1,601 pagesTotal Pharmacy Notes TPN For EEClaire Cura100% (2)
- Pharmacology Drug ChartDocument50 pagesPharmacology Drug ChartEssentialForLivingNo ratings yet
- Infusions in CCU 2Document1 pageInfusions in CCU 2MimiNo ratings yet
- Pharmacology SummaryDocument16 pagesPharmacology Summaryshenric16No ratings yet
- APHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDocument13 pagesAPHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDrSamia El WakilNo ratings yet
- Drugs To Watch With WARFARINDocument3 pagesDrugs To Watch With WARFARINRajendra RaiNo ratings yet
- Antimicrobial Renal DosingDocument5 pagesAntimicrobial Renal DosingdamondouglasNo ratings yet
- Kaplan Notes. ExamenSO IMPORTANTDocument145 pagesKaplan Notes. ExamenSO IMPORTANTLisaNo ratings yet
- Drug Recommendation GuideDocument6 pagesDrug Recommendation GuideGenNo ratings yet
- Brad Hinton CVDocument6 pagesBrad Hinton CVapi-486072801No ratings yet
- DosesDocument16 pagesDosesAli Adnan AfridiNo ratings yet
- Hypertension Drugs Cheat Sheet: by ViaDocument3 pagesHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharNo ratings yet
- Neuro Psych - Antiepileptic Drug ChartDocument5 pagesNeuro Psych - Antiepileptic Drug ChartMonica J Ortiz Pereira100% (1)
- CeftriaxoneDocument7 pagesCeftriaxoneGreats HalomoanNo ratings yet
- Common TreatmentsDocument5 pagesCommon TreatmentsRaj MandumulaNo ratings yet
- OB - Hypertensive DisordersDocument4 pagesOB - Hypertensive DisordersJasmine Nicole RemetreNo ratings yet
- 37 Page Revised NCLEXDocument38 pages37 Page Revised NCLEXJohnasse Sebastian NavalNo ratings yet
- (New) Common Paeds Long CasesDocument19 pages(New) Common Paeds Long CasesHengkai NeoNo ratings yet
- Pharmacology Test 3 - Cardiovascular Drugs, Part I Flashcards - QuizletDocument10 pagesPharmacology Test 3 - Cardiovascular Drugs, Part I Flashcards - QuizletBhopesh Kadian0% (1)
- Renr Practice Test 7 FinalDocument13 pagesRenr Practice Test 7 FinalTk100% (1)
- MCQ Base Clinical Pharmacology PDFDocument30 pagesMCQ Base Clinical Pharmacology PDFTesfa HopeNo ratings yet
- AneedzDocument60 pagesAneedzMjd ObiedNo ratings yet
- Amiodarone Hydrochloride in JDocument18 pagesAmiodarone Hydrochloride in JChrizzna HaryantoNo ratings yet
- Quizzes SubsDocument36 pagesQuizzes SubsApril Mae Agomo-oNo ratings yet
- Drugs 3Document43 pagesDrugs 3IonuțHerpeșNo ratings yet
- AKC Dogs Poisonous Plant GuideDocument1 pageAKC Dogs Poisonous Plant GuidestallionrpNo ratings yet
- ArrhythmiaDocument31 pagesArrhythmiaAbdallah Essam Al-ZireeniNo ratings yet
- Histological Effects of Abelmoschus Esculentus Extract and Its Isolated Flavonoid Glycosides and Triterpene On Mice HeartDocument4 pagesHistological Effects of Abelmoschus Esculentus Extract and Its Isolated Flavonoid Glycosides and Triterpene On Mice HeartInternational Journal of Innovative Science and Research Technology100% (1)
- 10 Peri Arrest ArrhythmiasDocument39 pages10 Peri Arrest ArrhythmiasAnaid FourevaNo ratings yet
- Emergency Drug Review: UHHS BMH Paramedic Training ProgramDocument116 pagesEmergency Drug Review: UHHS BMH Paramedic Training ProgramShailja HanumantaNo ratings yet
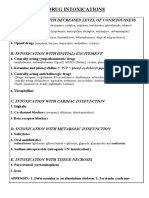
- Drug Intoxications: A. Intoxication With Decreased Level of ConsciousnessDocument22 pagesDrug Intoxications: A. Intoxication With Decreased Level of ConsciousnessVika ShoniaNo ratings yet
- Fundamentals of Nursing 1Document6 pagesFundamentals of Nursing 1Ruel M. BersabeNo ratings yet
- NCLEX Review Cardiovascular QuizDocument17 pagesNCLEX Review Cardiovascular Quizdany tesemaNo ratings yet
- Central Nervous System: Drug of Choices Notes - Kent Andrei Paelma Bsn-2FDocument22 pagesCentral Nervous System: Drug of Choices Notes - Kent Andrei Paelma Bsn-2FOfficially RandomNo ratings yet
- McqsDocument13 pagesMcqsDr. Anil LandgeNo ratings yet
- Lanoxin: (Digoxin) InjectionDocument35 pagesLanoxin: (Digoxin) InjectionZainNo ratings yet
- Crash CartDocument15 pagesCrash CartCLaui SagibalNo ratings yet
- Topic 5 - Fluid & ElectrolytesDocument3 pagesTopic 5 - Fluid & Electrolyteschristy INo ratings yet
- Pharmacology Questions CardiacDocument5 pagesPharmacology Questions CardiacAmanda SimpsonNo ratings yet
- Anti Arrhythmic DrugsDocument67 pagesAnti Arrhythmic DrugsMohammedMujahedNo ratings yet
- Answers PrescriptionDocument31 pagesAnswers PrescriptionAjay WadjeNo ratings yet
- Wellington ICU Drug Manual 2013Document444 pagesWellington ICU Drug Manual 2013khangsiean89No ratings yet
- 2017 Medical Pharmacology Practice Exam 4Document6 pages2017 Medical Pharmacology Practice Exam 4Franklin garryNo ratings yet
- Pharmacology ReviewersDocument5 pagesPharmacology ReviewersNeisha Halil VillarealNo ratings yet
- JalapDocument3 pagesJalapGulzar Ahmad RawnNo ratings yet
- Drugs For Heart FailureDocument39 pagesDrugs For Heart FailureOngKahYeeNo ratings yet
- Ventricular Tachycardia Bsn3b-Grp1Document35 pagesVentricular Tachycardia Bsn3b-Grp1Jessica RamosNo ratings yet























































































Download as pdf or txt
You might also like
- Heart Failure Topic DiscussionDocument11 pagesHeart Failure Topic Discussionapi-665372449No ratings yet
- Antibiotic Mixing Chart With SAMF InfoDocument8 pagesAntibiotic Mixing Chart With SAMF Infosumayyah995No ratings yet
- EKG RhythmsDocument10 pagesEKG RhythmsQueenNo ratings yet
- Antiarrhythmic Medication Chart - EBM Consult v3Document2 pagesAntiarrhythmic Medication Chart - EBM Consult v3Linlin100% (1)
- Diabetes Topic DiscussionDocument9 pagesDiabetes Topic DiscussionSamNo ratings yet
- A Drug For IntDocument58 pagesA Drug For IntVajirawit PetchsriNo ratings yet
- Calculations IDocument17 pagesCalculations INisreen SalameNo ratings yet
- Noradrenaline Infusion Rate BSUH Critical CareDocument4 pagesNoradrenaline Infusion Rate BSUH Critical CareAndreiCostei100% (1)
- Antihyperglycemic Agents Comparison Chart PDFDocument9 pagesAntihyperglycemic Agents Comparison Chart PDFconcoz100% (1)
- Acute MedicineDocument54 pagesAcute MedicineTipuNo ratings yet
- Spinal Cord CompressionDocument4 pagesSpinal Cord Compressionian3yeung-2No ratings yet
- Essenc I Al TherapyDocument9 pagesEssenc I Al TherapyFabian Ramirez HincapiéNo ratings yet
- OTC Pain Relievers Dosage Chart For Adults and Children 12 Years and OlderDocument2 pagesOTC Pain Relievers Dosage Chart For Adults and Children 12 Years and OlderAdocueNo ratings yet
- NOAC ChartDocument2 pagesNOAC Chartsgod34No ratings yet
- Review Handouts For Medical Pharmacology PDFDocument21 pagesReview Handouts For Medical Pharmacology PDFAndres F. TorresNo ratings yet
- DrugsDocument155 pagesDrugsAkankshaNo ratings yet
- Pharmacology of Cardiac Diseases MINEDocument3 pagesPharmacology of Cardiac Diseases MINEMitu Miressa تNo ratings yet
- Malaria Treatment IndiaDocument1 pageMalaria Treatment IndiaSubzer OmerNo ratings yet
- 2015 Pain Management For PediatricDocument2 pages2015 Pain Management For Pediatricdiany astutiNo ratings yet
- OTC Labels HorizontalDocument1 pageOTC Labels HorizontalTsoojiNo ratings yet
- C. Anti-Hypertensive Drugs.Document10 pagesC. Anti-Hypertensive Drugs.Nabeel AsifNo ratings yet
- IV PO Conversion CAPDocument3 pagesIV PO Conversion CAPdamondouglasNo ratings yet
- Pedia Stickers PDFDocument8 pagesPedia Stickers PDFAshNo ratings yet
- Ans 2 PDFDocument101 pagesAns 2 PDFrab yoNo ratings yet
- Antibiotic IV Administration During COVID-19Document5 pagesAntibiotic IV Administration During COVID-19David Hines LopezNo ratings yet
- Drug Side EffectsDocument2 pagesDrug Side EffectsAngelic khanNo ratings yet
- Insulin Chart: Insulin Type Onset of Action Peak Duration of ActionDocument1 pageInsulin Chart: Insulin Type Onset of Action Peak Duration of ActionGeorge ZachariahNo ratings yet
- Critical Care Drugs 2Document23 pagesCritical Care Drugs 2Asri Ernadi100% (1)
- Vancomycin Protocol RQHRDocument15 pagesVancomycin Protocol RQHRl1o2stNo ratings yet
- Prefix Suffix MnemonicsDocument5 pagesPrefix Suffix MnemonicsPj MontecilloNo ratings yet
- Drug Interactions: What Is An Interaction?Document4 pagesDrug Interactions: What Is An Interaction?Leyla MajundaNo ratings yet
- Summary of Antidiabetic Drugs PDFDocument3 pagesSummary of Antidiabetic Drugs PDFZinc YuloNo ratings yet
- Drug Card Emergency Department-1 PDFDocument2 pagesDrug Card Emergency Department-1 PDFdrmohdtanveerNo ratings yet
- Finished Ekg Study GuideDocument4 pagesFinished Ekg Study Guideapi-652914452No ratings yet
- Emergency Drugs: Drug Action Indications Adverse Effects Contraindications Nursing Management Atropine SulfateDocument15 pagesEmergency Drugs: Drug Action Indications Adverse Effects Contraindications Nursing Management Atropine Sulfate092109No ratings yet
- Review Handouts For Medical Pharmacology: Terriann Crisp, PH.DDocument28 pagesReview Handouts For Medical Pharmacology: Terriann Crisp, PH.Dmus zaharaNo ratings yet
- Drug ListsDocument10 pagesDrug ListsAmber Merritt100% (1)
- All Types of InsulinDocument18 pagesAll Types of Insulinali mohammedNo ratings yet
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 pageAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88No ratings yet
- Antibiotic Sensitivity FINAL V4 Sheet1Document1 pageAntibiotic Sensitivity FINAL V4 Sheet1JHNo ratings yet
- Neonate: TPR of Newborns BW 1500gDocument9 pagesNeonate: TPR of Newborns BW 1500gAnne Lorraine BringasNo ratings yet
- Smart Pumps Adult ITU Library v3Document73 pagesSmart Pumps Adult ITU Library v3Aqsa Ahmed SiddiquiNo ratings yet
- Total Pharmacy Notes TPN For EEDocument1,601 pagesTotal Pharmacy Notes TPN For EEClaire Cura100% (2)
- Pharmacology Drug ChartDocument50 pagesPharmacology Drug ChartEssentialForLivingNo ratings yet
- Infusions in CCU 2Document1 pageInfusions in CCU 2MimiNo ratings yet
- Pharmacology SummaryDocument16 pagesPharmacology Summaryshenric16No ratings yet
- APHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDocument13 pagesAPHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDrSamia El WakilNo ratings yet
- Drugs To Watch With WARFARINDocument3 pagesDrugs To Watch With WARFARINRajendra RaiNo ratings yet
- Antimicrobial Renal DosingDocument5 pagesAntimicrobial Renal DosingdamondouglasNo ratings yet
- Kaplan Notes. ExamenSO IMPORTANTDocument145 pagesKaplan Notes. ExamenSO IMPORTANTLisaNo ratings yet
- Drug Recommendation GuideDocument6 pagesDrug Recommendation GuideGenNo ratings yet
- Brad Hinton CVDocument6 pagesBrad Hinton CVapi-486072801No ratings yet
- DosesDocument16 pagesDosesAli Adnan AfridiNo ratings yet
- Hypertension Drugs Cheat Sheet: by ViaDocument3 pagesHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharNo ratings yet
- Neuro Psych - Antiepileptic Drug ChartDocument5 pagesNeuro Psych - Antiepileptic Drug ChartMonica J Ortiz Pereira100% (1)
- CeftriaxoneDocument7 pagesCeftriaxoneGreats HalomoanNo ratings yet
- Common TreatmentsDocument5 pagesCommon TreatmentsRaj MandumulaNo ratings yet
- OB - Hypertensive DisordersDocument4 pagesOB - Hypertensive DisordersJasmine Nicole RemetreNo ratings yet
- 37 Page Revised NCLEXDocument38 pages37 Page Revised NCLEXJohnasse Sebastian NavalNo ratings yet
- (New) Common Paeds Long CasesDocument19 pages(New) Common Paeds Long CasesHengkai NeoNo ratings yet
- Pharmacology Test 3 - Cardiovascular Drugs, Part I Flashcards - QuizletDocument10 pagesPharmacology Test 3 - Cardiovascular Drugs, Part I Flashcards - QuizletBhopesh Kadian0% (1)
- Renr Practice Test 7 FinalDocument13 pagesRenr Practice Test 7 FinalTk100% (1)
- MCQ Base Clinical Pharmacology PDFDocument30 pagesMCQ Base Clinical Pharmacology PDFTesfa HopeNo ratings yet
- AneedzDocument60 pagesAneedzMjd ObiedNo ratings yet
- Amiodarone Hydrochloride in JDocument18 pagesAmiodarone Hydrochloride in JChrizzna HaryantoNo ratings yet
- Quizzes SubsDocument36 pagesQuizzes SubsApril Mae Agomo-oNo ratings yet
- Drugs 3Document43 pagesDrugs 3IonuțHerpeșNo ratings yet
- AKC Dogs Poisonous Plant GuideDocument1 pageAKC Dogs Poisonous Plant GuidestallionrpNo ratings yet
- ArrhythmiaDocument31 pagesArrhythmiaAbdallah Essam Al-ZireeniNo ratings yet
- Histological Effects of Abelmoschus Esculentus Extract and Its Isolated Flavonoid Glycosides and Triterpene On Mice HeartDocument4 pagesHistological Effects of Abelmoschus Esculentus Extract and Its Isolated Flavonoid Glycosides and Triterpene On Mice HeartInternational Journal of Innovative Science and Research Technology100% (1)
- 10 Peri Arrest ArrhythmiasDocument39 pages10 Peri Arrest ArrhythmiasAnaid FourevaNo ratings yet
- Emergency Drug Review: UHHS BMH Paramedic Training ProgramDocument116 pagesEmergency Drug Review: UHHS BMH Paramedic Training ProgramShailja HanumantaNo ratings yet
- Drug Intoxications: A. Intoxication With Decreased Level of ConsciousnessDocument22 pagesDrug Intoxications: A. Intoxication With Decreased Level of ConsciousnessVika ShoniaNo ratings yet
- Fundamentals of Nursing 1Document6 pagesFundamentals of Nursing 1Ruel M. BersabeNo ratings yet
- NCLEX Review Cardiovascular QuizDocument17 pagesNCLEX Review Cardiovascular Quizdany tesemaNo ratings yet
- Central Nervous System: Drug of Choices Notes - Kent Andrei Paelma Bsn-2FDocument22 pagesCentral Nervous System: Drug of Choices Notes - Kent Andrei Paelma Bsn-2FOfficially RandomNo ratings yet
- McqsDocument13 pagesMcqsDr. Anil LandgeNo ratings yet
- Lanoxin: (Digoxin) InjectionDocument35 pagesLanoxin: (Digoxin) InjectionZainNo ratings yet
- Crash CartDocument15 pagesCrash CartCLaui SagibalNo ratings yet
- Topic 5 - Fluid & ElectrolytesDocument3 pagesTopic 5 - Fluid & Electrolyteschristy INo ratings yet
- Pharmacology Questions CardiacDocument5 pagesPharmacology Questions CardiacAmanda SimpsonNo ratings yet
- Anti Arrhythmic DrugsDocument67 pagesAnti Arrhythmic DrugsMohammedMujahedNo ratings yet
- Answers PrescriptionDocument31 pagesAnswers PrescriptionAjay WadjeNo ratings yet
- Wellington ICU Drug Manual 2013Document444 pagesWellington ICU Drug Manual 2013khangsiean89No ratings yet
- 2017 Medical Pharmacology Practice Exam 4Document6 pages2017 Medical Pharmacology Practice Exam 4Franklin garryNo ratings yet
- Pharmacology ReviewersDocument5 pagesPharmacology ReviewersNeisha Halil VillarealNo ratings yet
- JalapDocument3 pagesJalapGulzar Ahmad RawnNo ratings yet
- Drugs For Heart FailureDocument39 pagesDrugs For Heart FailureOngKahYeeNo ratings yet
- Ventricular Tachycardia Bsn3b-Grp1Document35 pagesVentricular Tachycardia Bsn3b-Grp1Jessica RamosNo ratings yet