Download as pdf or txt
You might also like
- National Objectives For HealthDocument85 pagesNational Objectives For HealthJesserene SorianoNo ratings yet
- Ministry of Health, Republic of Zambia - 2018 - National Human Resources For Health Strategic Plan 2018-2024Document100 pagesMinistry of Health, Republic of Zambia - 2018 - National Human Resources For Health Strategic Plan 2018-2024Sandra Barteit71% (7)
- Patients' Right (English-Tagalog)Document2 pagesPatients' Right (English-Tagalog)Rochelle Escalada - Ibanez100% (1)
- Nigeria: National Policy On HIV/AIDSDocument65 pagesNigeria: National Policy On HIV/AIDSState House NigeriaNo ratings yet
- Guidelines For Health CampsDocument1 pageGuidelines For Health Campsgarg_rishu0% (1)
- Effective Regulation - Issues and Challenges For The Nigerian Electricity Regulatory CommissionDocument20 pagesEffective Regulation - Issues and Challenges For The Nigerian Electricity Regulatory CommissionState House NigeriaNo ratings yet
- Carol Meyers-Discovering Eve Ancient Israelite Women in Context (1991) PDFDocument246 pagesCarol Meyers-Discovering Eve Ancient Israelite Women in Context (1991) PDFBeBent100% (3)
- Health System Delivery in BangladeshDocument50 pagesHealth System Delivery in BangladeshDip Ayan M100% (1)
- Primary Health CareDocument68 pagesPrimary Health CareShena Mie Adis Vallecera100% (1)
- 8 Risk Management in Contemporary Pharmacy PracticeDocument36 pages8 Risk Management in Contemporary Pharmacy PracticeLollyNo ratings yet
- Integrating Severe Acute Malnutrition Into The Management of Childhood Diseases at Community Level in South SudanDocument36 pagesIntegrating Severe Acute Malnutrition Into The Management of Childhood Diseases at Community Level in South Sudanmalaria_consortium100% (1)
- Mukinge College of Nursing PHN JAN 2018: Port HealthDocument39 pagesMukinge College of Nursing PHN JAN 2018: Port HealthBa Mulenga100% (3)
- Guidelines For Training Under ARSH For NIHFW 14.7.11Document26 pagesGuidelines For Training Under ARSH For NIHFW 14.7.11National Child Health Resource Centre (NCHRC)50% (2)
- DILG-DOH-NCIP Joint Circulars On Delivery of Health Services To IPsDocument18 pagesDILG-DOH-NCIP Joint Circulars On Delivery of Health Services To IPsVincent BautistaNo ratings yet
- Assessment of Knowledge, Attitude, and Practice of Telemedicine in IndiaDocument8 pagesAssessment of Knowledge, Attitude, and Practice of Telemedicine in IndiaIJRASETPublicationsNo ratings yet
- Community Diagnosis - Ms. Dorothy - 13476Document91 pagesCommunity Diagnosis - Ms. Dorothy - 13476Janet MbandiNo ratings yet
- Doh ProgramsDocument250 pagesDoh Programsjoyshe111No ratings yet
- Primary Health Care Maternal & Child HealthDocument32 pagesPrimary Health Care Maternal & Child HealthAbidah Rahmi HilmyNo ratings yet
- Health Sector Reform PDFDocument54 pagesHealth Sector Reform PDFCherry Mae L. VillanuevaNo ratings yet
- Scope & Concerns of Public HealthDocument56 pagesScope & Concerns of Public Healthraosaadi60% (5)
- Ghana's Health Care SystemDocument14 pagesGhana's Health Care SystemTheophilus BaidooNo ratings yet
- Aschiana: Afghan Children and New Approach Project ProposalDocument6 pagesAschiana: Afghan Children and New Approach Project Proposalsaher8901100% (1)
- Presentation On Primary Health CareDocument9 pagesPresentation On Primary Health Caresamragya rajkhadkaNo ratings yet
- Maternal Health, ICPDDocument24 pagesMaternal Health, ICPDHadley AuliaNo ratings yet
- Introduction To Health FinancingDocument101 pagesIntroduction To Health FinancingArianne A ZamoraNo ratings yet
- Primary Health Care Hand Outs For StudentsDocument35 pagesPrimary Health Care Hand Outs For StudentsGreggy VenturaNo ratings yet
- Malaria and Health Promotion ApproachDocument20 pagesMalaria and Health Promotion ApproachSantepromoNo ratings yet
- FCHVDocument22 pagesFCHVSamzana ShresthaNo ratings yet
- Supranational Organisations - FinalDocument26 pagesSupranational Organisations - FinalgeetrahiNo ratings yet
- Introduction To Public Health, FWACPDocument16 pagesIntroduction To Public Health, FWACPOlascholar0% (1)
- Health Promotion DiabetesDocument20 pagesHealth Promotion Diabetesharshotsai100% (1)
- Child Health Promotion-1Document6 pagesChild Health Promotion-1Oke Adasen100% (1)
- 3 Puntland Health Policy FrameworkDocument46 pages3 Puntland Health Policy Frameworkkunciil100% (1)
- Nat'l Health Program of The DOHDocument55 pagesNat'l Health Program of The DOHNathaniel PulidoNo ratings yet
- Yaws Eradication ProgrammeDocument1 pageYaws Eradication ProgrammeArchana SahuNo ratings yet
- Introduction To Public HealthDocument23 pagesIntroduction To Public HealthNhial Nyachol BolNo ratings yet
- Elements of Primary Health CareDocument55 pagesElements of Primary Health Caremskot100% (1)
- Health Promotion PolicyDocument12 pagesHealth Promotion PolicyLalita A/P AnbarasenNo ratings yet
- Health Financing: Dr. Jamelah R. Usman-PasagiDocument27 pagesHealth Financing: Dr. Jamelah R. Usman-PasagiGada AbdulcaderNo ratings yet
- Surveillance and Response To Notifiable Diseases, EpidemicsDocument10 pagesSurveillance and Response To Notifiable Diseases, EpidemicsRacquel FrondaNo ratings yet
- 2021 Budget BrieferDocument24 pages2021 Budget Brieferyg loveNo ratings yet
- Breastfeeding HospitalDocument37 pagesBreastfeeding Hospitalemmanjabasa100% (1)
- health care system of swedenبDocument34 pageshealth care system of swedenبAhmedAljebouli0% (1)
- A Training Program in Community-Directed Intervention To Improve Access To Essential Health Services Training GuideDocument48 pagesA Training Program in Community-Directed Intervention To Improve Access To Essential Health Services Training GuideBushra AlMakaleh100% (1)
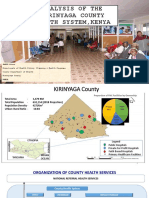
- Analysis of The Kirinyaga County Health System - Esbon - GakuuDocument18 pagesAnalysis of The Kirinyaga County Health System - Esbon - Gakuuesbon gakuu100% (1)
- 6-Global Health and Globalization and Public HealthDocument67 pages6-Global Health and Globalization and Public HealthMoreiyamNo ratings yet
- Who Actions Towards SDGS: MR Sharad Adhikary Technical Officer Who IndonesiaDocument14 pagesWho Actions Towards SDGS: MR Sharad Adhikary Technical Officer Who IndonesiaReny Widya AstutiNo ratings yet
- Writing A Health Policy Brief With OutlineDocument14 pagesWriting A Health Policy Brief With OutlineyandhiasNo ratings yet
- BHW TRAINING Child HealtDocument36 pagesBHW TRAINING Child HealtWilma BeraldeNo ratings yet
- Community Health A Complete Guide - 2020 EditionFrom EverandCommunity Health A Complete Guide - 2020 EditionRating: 5 out of 5 stars5/5 (1)
- The Health Promotion HandbookDocument63 pagesThe Health Promotion HandbookOnyd Subingsubing100% (1)
- DOH ARV Guidelines 2018Document27 pagesDOH ARV Guidelines 2018rommel mendoza100% (1)
- Nutrition Course For PHO Dec, 2022Document142 pagesNutrition Course For PHO Dec, 2022Semon YohannesNo ratings yet
- Port Health - OverviewDocument30 pagesPort Health - OverviewKay BristolNo ratings yet
- Lesson 1 - Public Health ConceptsDocument33 pagesLesson 1 - Public Health ConceptsCindy Rose MisenaNo ratings yet
- Complete CHEW CurriculumDocument162 pagesComplete CHEW CurriculumAbdulhamidNo ratings yet
- Maternal HealthDocument17 pagesMaternal HealthMartinNo ratings yet
- Summary Mobile HealthDocument31 pagesSummary Mobile HealthmhemaraNo ratings yet
- Capstone Paper Summative FINAL VERSIONDocument10 pagesCapstone Paper Summative FINAL VERSIONoliviajuolaNo ratings yet
- Primary Health CareDocument30 pagesPrimary Health CareSan SiddzNo ratings yet
- Universal Healthcare and Access to the Lower-Income Population: An Exploration of Capitation in Lagos, NigeriaFrom EverandUniversal Healthcare and Access to the Lower-Income Population: An Exploration of Capitation in Lagos, NigeriaNo ratings yet
- Dorcas Idowu PHD Thesis..FINAL-July-2016Document286 pagesDorcas Idowu PHD Thesis..FINAL-July-2016Abiola Babatunde AbimbolaNo ratings yet
- Asset Securitisation and Long Term Financing in The Power SectorDocument63 pagesAsset Securitisation and Long Term Financing in The Power SectorState House NigeriaNo ratings yet
- Update On Activities in The Nigerian Power SectorDocument28 pagesUpdate On Activities in The Nigerian Power SectorState House NigeriaNo ratings yet
- The Law As A Guide in The Performance of Police DutiesDocument17 pagesThe Law As A Guide in The Performance of Police DutiesState House NigeriaNo ratings yet
- Strategies For Re-Organisation and Re-Orientation of The Nigeria PoliceDocument39 pagesStrategies For Re-Organisation and Re-Orientation of The Nigeria PoliceState House NigeriaNo ratings yet
- Harnessing Science and Technology Research For Sustainable National DevelopmentDocument21 pagesHarnessing Science and Technology Research For Sustainable National DevelopmentState House NigeriaNo ratings yet
- R&D and The Challenges of Wealth Creation in NigeriaDocument47 pagesR&D and The Challenges of Wealth Creation in NigeriaState House Nigeria100% (1)
- The Exploitation of Natural Energy Resources in Nigeria For Accelerated Socio-Economic Development - Strategies and Opportunities For InvestmentDocument57 pagesThe Exploitation of Natural Energy Resources in Nigeria For Accelerated Socio-Economic Development - Strategies and Opportunities For InvestmentState House NigeriaNo ratings yet
- Repositioning Science, Technology and Innovation System To Meet The Challenges of Vision 20:2020Document41 pagesRepositioning Science, Technology and Innovation System To Meet The Challenges of Vision 20:2020State House NigeriaNo ratings yet
- Factors Inhibiting Police Performance in NigeriaDocument26 pagesFactors Inhibiting Police Performance in NigeriaState House NigeriaNo ratings yet
- Role of Judges in RegulationDocument21 pagesRole of Judges in RegulationState House NigeriaNo ratings yet
- Existing Structures For The Protection of Consumer Rights in The Nigerian Electricity MarketDocument25 pagesExisting Structures For The Protection of Consumer Rights in The Nigerian Electricity MarketState House NigeriaNo ratings yet
- Institutional Mechanisms For Research Institutions/Industry Linkages: Feasibility Study of The Obafemi Awolowo University Knowledge ParkDocument32 pagesInstitutional Mechanisms For Research Institutions/Industry Linkages: Feasibility Study of The Obafemi Awolowo University Knowledge ParkState House NigeriaNo ratings yet
- Optimizing The Exploitation of Natural Energy Resources in Nigeria For Accelerated Socio-Economic Development: Strategies and Opportunities For InvestmentDocument57 pagesOptimizing The Exploitation of Natural Energy Resources in Nigeria For Accelerated Socio-Economic Development: Strategies and Opportunities For InvestmentState House Nigeria100% (1)
- The Powers of The Nigerian Electricity Regulatory Commission (NERC) To Regulate Electricity Consumers' RightsDocument26 pagesThe Powers of The Nigerian Electricity Regulatory Commission (NERC) To Regulate Electricity Consumers' RightsState House NigeriaNo ratings yet
- Geometric Power Limited: National Conference On Electricity Consumers in NigeriaDocument13 pagesGeometric Power Limited: National Conference On Electricity Consumers in NigeriaState House NigeriaNo ratings yet
- Proposed Energy Efficiency Labeling and Standards For Electrical AppliancesDocument32 pagesProposed Energy Efficiency Labeling and Standards For Electrical AppliancesState House Nigeria100% (1)
- Modalities For Importation of Goods and IncentivesDocument4 pagesModalities For Importation of Goods and IncentivesState House NigeriaNo ratings yet
- Harnessing Science and Technology Research Results For Sustainable National DevelopmentDocument21 pagesHarnessing Science and Technology Research Results For Sustainable National DevelopmentState House NigeriaNo ratings yet
- Evolving Strategies For Sustainable Financing R&D Activities Through The Public-Private Partnership Arrangement in A Developing Country Like Nigeria - Bank of Industries (BOI)Document13 pagesEvolving Strategies For Sustainable Financing R&D Activities Through The Public-Private Partnership Arrangement in A Developing Country Like Nigeria - Bank of Industries (BOI)State House NigeriaNo ratings yet
- Nigeria: Vision 20:2020 Economic Transformation BlueprintDocument218 pagesNigeria: Vision 20:2020 Economic Transformation BlueprintState House NigeriaNo ratings yet
- The Spectrum DictionaryDocument41 pagesThe Spectrum DictionaryLey Lortie100% (1)
- ABCs LGBTQ Script 201124Document4 pagesABCs LGBTQ Script 201124orsabiamarieleNo ratings yet
- Activity Design For Pamana Esp and San LuisDocument12 pagesActivity Design For Pamana Esp and San LuisMarceliano Monato IIINo ratings yet
- Effect of Parent's Gender On Academic Achievement of AdolosecentsDocument9 pagesEffect of Parent's Gender On Academic Achievement of Adolosecentslucylovesbooks6770No ratings yet
- 2.1 Engle MerryDocument9 pages2.1 Engle MerryRitesh RajNo ratings yet
- Influence of Business Ethics Judgments of Malaysiaa AccountantsDocument16 pagesInfluence of Business Ethics Judgments of Malaysiaa AccountantsCyrilraincreamNo ratings yet
- Doe v. FCPS ExhibitsDocument314 pagesDoe v. FCPS Exhibitsweb-producersNo ratings yet
- Big Picture On Sex and Gender (Read in "Fullscreen")Document17 pagesBig Picture On Sex and Gender (Read in "Fullscreen")Wellcome Trust50% (6)
- This Is A Man's Problem REPORTDocument146 pagesThis Is A Man's Problem REPORTHong Lien TranNo ratings yet
- 45 Buckingham Ecof 21st CenturyDocument80 pages45 Buckingham Ecof 21st CenturyPonyo LilpondNo ratings yet
- SOP, Hypothesis, RRLDocument7 pagesSOP, Hypothesis, RRLHavier EsparagueraNo ratings yet
- Research GRP G. ProposalDocument38 pagesResearch GRP G. ProposalAndy GarciaNo ratings yet
- Revised Social Content GuidelinesDocument14 pagesRevised Social Content GuidelinesDimpleNo ratings yet
- Project AssignmentDocument5 pagesProject AssignmentFariha Younas DarNo ratings yet
- Final Fnis Assignment 3Document6 pagesFinal Fnis Assignment 3api-521537122No ratings yet
- On Glass CeilingDocument20 pagesOn Glass Ceilingnidhipatell0% (1)
- Read Letitia James's LetterDocument2 pagesRead Letitia James's LetterNewsdayNo ratings yet
- Template D Gender Equality PolicyDocument2 pagesTemplate D Gender Equality PolicyLorena Beltrán VillamilNo ratings yet
- SS Philosophy ProjectDocument24 pagesSS Philosophy ProjectCE SherNo ratings yet
- The Challenges of Middle and Late Adolescence: A CompilationDocument10 pagesThe Challenges of Middle and Late Adolescence: A CompilationDanellNo ratings yet
- Gender Discrimination AssignmentDocument3 pagesGender Discrimination AssignmentAli SchehzadNo ratings yet
- Sex and Gender Not So Binary TealDocument2 pagesSex and Gender Not So Binary TealJo InglesNo ratings yet
- Development and Gender Stereotype ScaleDocument10 pagesDevelopment and Gender Stereotype Scale3PA01Safana QamaraniNo ratings yet
- Marginal LiteratureDocument3 pagesMarginal LiteratureKamalNo ratings yet
- HSR ParentDocument9 pagesHSR ParentsevattapillaiNo ratings yet
- Factors Affecting College Degree Preferences of Shs Stem Students of The College of Engineering and Technology of Western Mindanao State UniversityDocument11 pagesFactors Affecting College Degree Preferences of Shs Stem Students of The College of Engineering and Technology of Western Mindanao State UniversityBianca Marie Uypala ErquilangNo ratings yet
- English ProjectDocument23 pagesEnglish Projectyuvanshankar2024No ratings yet
- A Feminist Reading of The Fluidity of Gender Roles and The Ramifications of This in Bram Stoker's Dracula (Stoker, 1897) and Anne Rice's Interview With The Vampire (Rice, 1976)Document45 pagesA Feminist Reading of The Fluidity of Gender Roles and The Ramifications of This in Bram Stoker's Dracula (Stoker, 1897) and Anne Rice's Interview With The Vampire (Rice, 1976)Chelsbelle100% (1)
- Yup, It's Great To Be A White Male LawyerDocument2 pagesYup, It's Great To Be A White Male LawyerJosephine MillerNo ratings yet