Download as docx, pdf, or txt
You might also like
- Kingdom Come (1996) (Digital) (TheHand-Empire) PDFDocument222 pagesKingdom Come (1996) (Digital) (TheHand-Empire) PDFBarack Abomasum93% (14)
- Imci FormDocument3 pagesImci FormVon Jethro Palas100% (1)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationHeavenNo ratings yet
- Risk For Injury Nursing Care Plan Assessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluation Subjective Data: Short Term: Goal Met Short TermDocument3 pagesRisk For Injury Nursing Care Plan Assessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluation Subjective Data: Short Term: Goal Met Short TermSherry Ann FayeNo ratings yet
- NCP-Acute Postpartum Perineal PainDocument2 pagesNCP-Acute Postpartum Perineal PainFrenzylane Diane CoralNo ratings yet
- CaseanalysisDocument2 pagesCaseanalysisChrislyn Dian Pene100% (1)
- NCP GCS Powerlessness - LIADocument3 pagesNCP GCS Powerlessness - LIADickson,Emilia Jade100% (1)
- Nursing Care Plan Acute Pain For Ceasarean BirthDocument2 pagesNursing Care Plan Acute Pain For Ceasarean BirthjajalerNo ratings yet
- Nursing Care Plan For Subconjunctival Hemorrhage OSDocument8 pagesNursing Care Plan For Subconjunctival Hemorrhage OSRosemarie CarpioNo ratings yet
- Nursing Care Plan (Post Op Exlap)Document2 pagesNursing Care Plan (Post Op Exlap)Kay D. BeredoNo ratings yet
- Common Instruments in ORDocument3 pagesCommon Instruments in ORbladimer_ria100% (1)
- Nursing Care Plan GlaucomaDocument3 pagesNursing Care Plan Glaucomasephirus77750% (4)
- Nursing Care PlansDocument2 pagesNursing Care PlansatchiekNo ratings yet
- Basics of The CMM 120Document4 pagesBasics of The CMM 120cqi9nNo ratings yet
- RRLfor Gasoline StationDocument6 pagesRRLfor Gasoline StationWellan Joy Dela Fuerta100% (1)
- TK3723+Data+Sheet+v0 23Document89 pagesTK3723+Data+Sheet+v0 23Phong LêNo ratings yet
- Guided Wave System ComparisonDocument3 pagesGuided Wave System ComparisonsenthilndtNo ratings yet
- Cefuroxime Drug StudyDocument2 pagesCefuroxime Drug StudyDanica Kate Galleon100% (1)
- NCP - AnxietyDocument4 pagesNCP - AnxietyRoyce Vincent Tizon100% (1)
- Nursing Care Plan: Subjective Data " GoalDocument2 pagesNursing Care Plan: Subjective Data " GoalJay VillasotoNo ratings yet
- NCP MS DbiDocument2 pagesNCP MS DbiSj EclipseNo ratings yet
- HONRADO-Group 3 - Pedia NCPDocument7 pagesHONRADO-Group 3 - Pedia NCP2A - Nicole Marrie HonradoNo ratings yet
- Surgical Instrument SETSDocument16 pagesSurgical Instrument SETSChanel FordNo ratings yet
- Name of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesDocument2 pagesName of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesKarl Lourenz DeysolongNo ratings yet
- Drug StudyDocument16 pagesDrug StudyAlessandra Franchesca CortezNo ratings yet
- NCP SEIZURE DISORDERDocument2 pagesNCP SEIZURE DISORDERPatricia FaraonNo ratings yet
- DeficientDocument2 pagesDeficientVANNEZA TRIXZY TAMPARONGNo ratings yet
- NCP Actual and PotentialDocument4 pagesNCP Actual and PotentialKristian Karl Bautista Kiw-isNo ratings yet
- Drug Study TramadolDocument2 pagesDrug Study TramadolJemina Rafanan Racadio100% (1)
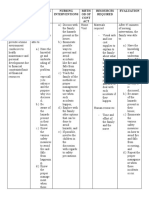
- Family Nursing Problems Objectives of Care Nursing Interventions Meth Od of Cont ACT Resources Required EvaluationDocument2 pagesFamily Nursing Problems Objectives of Care Nursing Interventions Meth Od of Cont ACT Resources Required EvaluationWenalyn Grace Abella LlavanNo ratings yet
- Orbital Trauma NCP and Drug StudyDocument5 pagesOrbital Trauma NCP and Drug StudyDersly LaneNo ratings yet
- NURSING CARE PLAN Dog Bite InjuryDocument3 pagesNURSING CARE PLAN Dog Bite Injurykarrey danielNo ratings yet
- NCP Acute PainDocument2 pagesNCP Acute PainMillicent Faye G. Gelit50% (2)
- NCP Risk For InjuryDocument1 pageNCP Risk For InjuryRenz Kier L. ComaNo ratings yet
- Nursing Care PlanDocument13 pagesNursing Care PlanRen DolosaNo ratings yet
- Care of Older PersonDocument3 pagesCare of Older PersonIt's EllaaaNo ratings yet
- Nursing Care Plan - HyperDocument4 pagesNursing Care Plan - HyperJennalyn Casapao100% (1)
- FNCPDocument5 pagesFNCPMajojay AmadorNo ratings yet
- Perioperative Nursing Care Plan TAHBSODocument4 pagesPerioperative Nursing Care Plan TAHBSOPatricia OrtegaNo ratings yet
- Constipation NCPDocument2 pagesConstipation NCPAbby GonzalesNo ratings yet
- FDAR Chart - CamahalanDocument1 pageFDAR Chart - CamahalanCamahalan, Johnry G.100% (1)
- Assignment No.1 OB High Risk Grp.1Document3 pagesAssignment No.1 OB High Risk Grp.1YongNo ratings yet
- NCP Acute Pain FURUNCOLOSISDocument2 pagesNCP Acute Pain FURUNCOLOSISMaria Imogen MilambilingNo ratings yet
- Nursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPDocument2 pagesNursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPLP Benoza100% (2)
- NCP Acute Pain VaDocument3 pagesNCP Acute Pain VaKate ClarosNo ratings yet
- Nurse Patient InteractionDocument14 pagesNurse Patient InteractionIrish Eunice FelixNo ratings yet
- NCP AfDocument3 pagesNCP AfAngelica Mercado SirotNo ratings yet
- Nursing Care Plan #1Document6 pagesNursing Care Plan #1Yamete KudasaiNo ratings yet
- Acute Pain OsteosarcomaDocument8 pagesAcute Pain OsteosarcomaMaryjoy Gabriellee De La Cruz100% (1)
- Family NCPDocument3 pagesFamily NCPmarohunk50% (2)
- Nursing Care Plan For Nitumusiina Billy Admitted With Acute Otitis Media and TonsillitisDocument6 pagesNursing Care Plan For Nitumusiina Billy Admitted With Acute Otitis Media and TonsillitisNatukunda Dianah100% (1)
- Spina Bifida NCPDocument3 pagesSpina Bifida NCPShahzad GulfamNo ratings yet
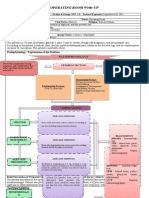
- Operating Room Write-Up: PathophysiologyDocument4 pagesOperating Room Write-Up: PathophysiologyArian May MarcosNo ratings yet
- Degenerative Diseases NCMB316 SEC1 AMENINDocument4 pagesDegenerative Diseases NCMB316 SEC1 AMENINHermin TorresNo ratings yet
- Hypothyroidism Nursing Care PlanDocument3 pagesHypothyroidism Nursing Care PlanRizza Mae MaglacionNo ratings yet
- Fracture NCPDocument4 pagesFracture NCPCharlene Grace ReginoNo ratings yet
- NCP 1 - Chicken PoxDocument2 pagesNCP 1 - Chicken Poxphearlie100% (2)
- Nursing Care PlanDocument2 pagesNursing Care PlanRALPH VINZ NABATARNo ratings yet
- Nursing Care Plan For Diarrhea 2Document1 pageNursing Care Plan For Diarrhea 2Skyla FiestaNo ratings yet
- Nursing Care Plan - Risk For Falls (Antepartum)Document2 pagesNursing Care Plan - Risk For Falls (Antepartum)kaimimiyaNo ratings yet
- Head-To-Toe AssessmentDocument10 pagesHead-To-Toe AssessmentJenny Rose Colico RNNo ratings yet
- Drug Ang NCPDocument9 pagesDrug Ang NCPMelanie GaledoNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- Nursing Care PlansDocument2 pagesNursing Care PlansatchiekNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanAmsh RosalNo ratings yet
- Acute Pain NCPDocument2 pagesAcute Pain NCPfbarlicosNo ratings yet
- What Is The ReasonDocument2 pagesWhat Is The ReasonatchiekNo ratings yet
- Tramadol UltramDocument2 pagesTramadol UltramatchiekNo ratings yet
- Diabetic NephropathyDocument2 pagesDiabetic NephropathyatchiekNo ratings yet
- Tramadol UltramDocument2 pagesTramadol UltramatchiekNo ratings yet
- Nursing Care PlansDocument2 pagesNursing Care PlansatchiekNo ratings yet
- Diabetic NephopathyDocument2 pagesDiabetic NephopathyatchiekNo ratings yet
- Drug StudyDocument3 pagesDrug StudyatchiekNo ratings yet
- Diagnostic TestDocument7 pagesDiagnostic TestatchiekNo ratings yet
- Mock Test 1 (Q.e.)Document3 pagesMock Test 1 (Q.e.)Mehul PatilNo ratings yet
- Pre-Excavation ChecklistDocument2 pagesPre-Excavation ChecklistminimeezyNo ratings yet
- Resource Pack - Science - Year 1 - Human Body and SensesDocument19 pagesResource Pack - Science - Year 1 - Human Body and Sensesnur fazlynaNo ratings yet
- Principles and Interpretation of CardiotocographyDocument9 pagesPrinciples and Interpretation of CardiotocographyCKNo ratings yet
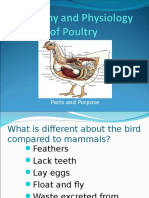
- Poultry Anatomy and PhysiologyDocument40 pagesPoultry Anatomy and PhysiologyMamtaNo ratings yet
- V 0226012420 0007 PDFDocument6 pagesV 0226012420 0007 PDFKhairulNo ratings yet
- 22 - Relative Permeability Effects On The Miscible CO2 WAG Injection SchemesDocument9 pages22 - Relative Permeability Effects On The Miscible CO2 WAG Injection SchemesheviNo ratings yet
- Straight / Angulated Multi-Unit System: © MIS Corporation. All Rights ReservedDocument12 pagesStraight / Angulated Multi-Unit System: © MIS Corporation. All Rights ReservedKrupali JainNo ratings yet
- GY 112 Lecture NotesDocument13 pagesGY 112 Lecture NotesSyed Jabed Miadad AliNo ratings yet
- REPORTDocument6 pagesREPORTrachana singhNo ratings yet
- Daniel Dennett-Philosophy Has A Big Role To Play, "If Only It Will Play It" (Prospect)Document3 pagesDaniel Dennett-Philosophy Has A Big Role To Play, "If Only It Will Play It" (Prospect)AidanNo ratings yet
- Fartlek - WikipediaDocument7 pagesFartlek - Wikipediamohan raoNo ratings yet
- YC450 Traveling Block Instruction ManualDocument9 pagesYC450 Traveling Block Instruction ManualMohamed el attarNo ratings yet
- Poitivism - Post PositivismDocument3 pagesPoitivism - Post PositivismANSH FFNo ratings yet
- Badminton 1Document32 pagesBadminton 1MaroLynn Natalia RominaNo ratings yet
- 1 Chapter 6 SPE 116633 PA An Integrated Geomechanical and Passive Sand Control ApproachDocument13 pages1 Chapter 6 SPE 116633 PA An Integrated Geomechanical and Passive Sand Control ApproachViệt Toàn ĐỗNo ratings yet
- Annex 52A Selection of Wiring Systems: (Normative)Document10 pagesAnnex 52A Selection of Wiring Systems: (Normative)Mihaela AntonNo ratings yet
- Executive SummaryDocument9 pagesExecutive SummaryJessNo ratings yet
- EthambutolDocument1 pageEthambutolSibel ErtuğrulNo ratings yet
- Chang Chemistry - Assessment Chapter 7Document10 pagesChang Chemistry - Assessment Chapter 7haha_le12No ratings yet
- CHALLENGES IN IMPLEMENTING A NEW SIGNALLING SYSTEM TO REPLACE AN EXISTING SIGNALLING SYSTEM WHILE MAINTAINING NORMAL TRAIN SERVICE-good ReferenceDocument47 pagesCHALLENGES IN IMPLEMENTING A NEW SIGNALLING SYSTEM TO REPLACE AN EXISTING SIGNALLING SYSTEM WHILE MAINTAINING NORMAL TRAIN SERVICE-good ReferencePulin ChaudhariNo ratings yet
- Spec Sheet Scania R730la4x2mnaDocument4 pagesSpec Sheet Scania R730la4x2mnaRoman PopulikNo ratings yet
- Waite TarotDocument134 pagesWaite TarotTammy ChauNo ratings yet
- Gyoza RecipeDocument10 pagesGyoza Recipemaylisa anggrainiNo ratings yet
- Practical Stress Analysis For Design... by Flabel, Jean-ClaudeDocument1 pagePractical Stress Analysis For Design... by Flabel, Jean-ClaudeDAVID GRACEYNo ratings yet