Download as pptx, pdf, or txt
You might also like
- Reflection Refraction WorksheetDocument2 pagesReflection Refraction WorksheetJfoxx Samuel71% (7)
- Kidney MCQDocument14 pagesKidney MCQNikita Nanwani86% (36)
- Urinary System Review GuideDocument3 pagesUrinary System Review Guideapi-305436791100% (1)
- PhysioEx Exercise 9 Activity 2Document3 pagesPhysioEx Exercise 9 Activity 2MARILYN MARIANA HERNANDEZ MENDOZANo ratings yet
- Liverpool SDL CRRTDocument62 pagesLiverpool SDL CRRTupul85No ratings yet
- Case Study On Chronic Kidney DiseaseDocument101 pagesCase Study On Chronic Kidney DiseaseZNEROL100% (6)
- Drug MetabolismDocument52 pagesDrug MetabolismUsman AkhtarNo ratings yet
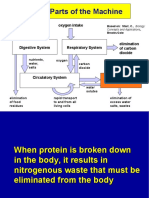
- Major Parts of The Machine: Food, Water Intake Oxygen IntakeDocument24 pagesMajor Parts of The Machine: Food, Water Intake Oxygen Intakecarl.lontoc2928No ratings yet
- ExcretionDocument13 pagesExcretionjerome jeromeNo ratings yet
- Excretory System-IDocument29 pagesExcretory System-IAkash KumarNo ratings yet
- The Excretory SystemDocument11 pagesThe Excretory Systemapi-3759646100% (2)
- Excretion & Homeostasis.Document142 pagesExcretion & Homeostasis.Jharell CaravlhoNo ratings yet
- Topic 6 - Excretory System 2021Document49 pagesTopic 6 - Excretory System 2021Ralph Rezin MooreNo ratings yet
- BIOLOGYDocument15 pagesBIOLOGYmanigbasrea15No ratings yet
- Edexcel Ial Biology Unit 5: The KidneyDocument24 pagesEdexcel Ial Biology Unit 5: The KidneyMithun ParanitharanNo ratings yet
- Excretory SystemDocument37 pagesExcretory SystemPatrick DeeNo ratings yet
- Excretory SystemDocument61 pagesExcretory Systemalayca cabatanaNo ratings yet
- ExcretionDocument54 pagesExcretionSarah SabirNo ratings yet
- EXCRETIONDocument9 pagesEXCRETIONMaira CanashinNo ratings yet
- Kidney, Excretion & OsmoregulationDocument65 pagesKidney, Excretion & OsmoregulationZaura100% (1)
- The Excretory SystemDocument3 pagesThe Excretory SystemMariel Abatayo0% (1)
- 11 Biology Notes ch19 Excretory Products and Their Elimination 1Document4 pages11 Biology Notes ch19 Excretory Products and Their Elimination 1Sumanth SY 1119No ratings yet
- Filtering Wastes From The Bloodstream: Dihydroxycholecalciferol (Calcitriol) and ProstaglandinsDocument7 pagesFiltering Wastes From The Bloodstream: Dihydroxycholecalciferol (Calcitriol) and ProstaglandinsJerome Miguel SantosNo ratings yet
- The Excretory System: Back To TopDocument10 pagesThe Excretory System: Back To TopDANIA PURNAMANo ratings yet
- Notes Grade: IX Subject: Biology Unit: 12 Topic: Excretion ObjectivesDocument21 pagesNotes Grade: IX Subject: Biology Unit: 12 Topic: Excretion Objectivespraneeth satishNo ratings yet
- GR11 Module 10 Notes and Excercise ActivitiesDocument27 pagesGR11 Module 10 Notes and Excercise Activitiescxhk6tgmybNo ratings yet
- Excretory System of BirdDocument20 pagesExcretory System of BirdPrakash PanthiNo ratings yet
- Life Processes - Excretion - Humans & Plants - OriginalDocument36 pagesLife Processes - Excretion - Humans & Plants - Originalnouraft.07No ratings yet
- Class 10 Biology Chapter 8 Revision NotesDocument5 pagesClass 10 Biology Chapter 8 Revision NotesOm KapoorNo ratings yet
- Excretory SystemDocument6 pagesExcretory SystemAJAYI PETERNo ratings yet
- Urinary SystemDocument29 pagesUrinary SystemRuwan WijesooriyaNo ratings yet
- The Renal SystemDocument53 pagesThe Renal SystemDarvey LongaraNo ratings yet
- 3.4.6 Excretory System H 3.4.8Document9 pages3.4.6 Excretory System H 3.4.8Joy FernandezNo ratings yet
- Biology 13Document11 pagesBiology 13Katlego MedupeNo ratings yet
- 0610 Biology EXCRETIONDocument27 pages0610 Biology EXCRETIONMunir LakhaNo ratings yet
- Excretory Organ PDF Invertebrates.Document13 pagesExcretory Organ PDF Invertebrates.E RAMESHBABUNo ratings yet
- The Excretory System-14 Dr. Hazim AL-RAWIDocument11 pagesThe Excretory System-14 Dr. Hazim AL-RAWIDrAli Al-FendiNo ratings yet
- Zoo 1 Excretion and OsmoregulationDocument17 pagesZoo 1 Excretion and OsmoregulationMaheshkumar KalalNo ratings yet
- ExcretionDocument10 pagesExcretionAhra KamruddinNo ratings yet
- Life Processes - ExcretionDocument18 pagesLife Processes - ExcretionraghavrungtambwaNo ratings yet
- 1.6 EXCRETION-The Removal of WasteDocument13 pages1.6 EXCRETION-The Removal of WastesamiktshyagiriNo ratings yet
- Al Wadi International School Biology Grade 9 13. Excretion in Humans NotesDocument42 pagesAl Wadi International School Biology Grade 9 13. Excretion in Humans NotesMohammed HelmyNo ratings yet
- Biokimia Urine, Sisa Metabolisme Dan Pembentukan BatuDocument104 pagesBiokimia Urine, Sisa Metabolisme Dan Pembentukan BatuHenny Taufik GosalNo ratings yet
- 46.2 Excretory and Urinary SystemDocument32 pages46.2 Excretory and Urinary Systemapi-520057338No ratings yet
- Anatomy and Physiology: Urinary System (Renal System)Document27 pagesAnatomy and Physiology: Urinary System (Renal System)dima_FlaviaNo ratings yet
- The Kidney Excretion and OsmoregulationDocument12 pagesThe Kidney Excretion and OsmoregulationLashaunte Hodge HobsonNo ratings yet
- The Kidneys and Formation of Urine 3 New 0Document22 pagesThe Kidneys and Formation of Urine 3 New 0Iph anyiNo ratings yet
- Urinary SystemDocument10 pagesUrinary Systemapi-19824701No ratings yet
- Water-Salt Metabolism in The Body: Intracellular Fluid CompositionDocument6 pagesWater-Salt Metabolism in The Body: Intracellular Fluid CompositionFranklyn Favour FlorenceNo ratings yet
- EXCRETIONDocument3 pagesEXCRETIONchristinakumari05No ratings yet
- Excretory System by Macalin Axmed OmaarDocument9 pagesExcretory System by Macalin Axmed OmaarAhmed OmaarNo ratings yet
- Homeostasis and ExcretionDocument22 pagesHomeostasis and Excretionmunzeerlubna4No ratings yet
- Biology Notes IGCSE Excretion NoteDocument9 pagesBiology Notes IGCSE Excretion NoteCorina HuNo ratings yet
- The Physiology of The Urine Production (2021)Document80 pagesThe Physiology of The Urine Production (2021)Shelly NobelNo ratings yet
- HomeostasisDocument10 pagesHomeostasiszainah jabrNo ratings yet
- ExcretionDocument26 pagesExcretionfatima zahraNo ratings yet
- Urinary System 25 Feb 2013Document44 pagesUrinary System 25 Feb 2013adystiNo ratings yet
- Excretionn in Humans (Word)Document1 pageExcretionn in Humans (Word)Technical NihalNo ratings yet
- Chapter 13 ExcretionDocument5 pagesChapter 13 ExcretionWezu heavenNo ratings yet
- Unit 2.43: Excretion: Removal of Waste Products of MetabolismDocument20 pagesUnit 2.43: Excretion: Removal of Waste Products of MetabolismxspiirONo ratings yet
- S3 Biology HOMEOSTASIS Notes - pdf417539Document26 pagesS3 Biology HOMEOSTASIS Notes - pdf417539SsebuumaNo ratings yet
- Urinary SystemDocument6 pagesUrinary SystemCrystal MaidenNo ratings yet
- Excretory SystemDocument19 pagesExcretory SystemElliz DoctoraNo ratings yet
- 1021 Lecture Question Bank PDFDocument44 pages1021 Lecture Question Bank PDFaskldhfdasjkNo ratings yet
- Expelling (Getting Rid Of) Any Undigested Food Eliminates Undigested MaterialsDocument12 pagesExpelling (Getting Rid Of) Any Undigested Food Eliminates Undigested MaterialscamilaNo ratings yet
- KMU-PGCN The Urinary System Shorter Colored 1Document101 pagesKMU-PGCN The Urinary System Shorter Colored 1M Shafique SadiqeeNo ratings yet
- Physics NotesDocument85 pagesPhysics NotesJfoxx Samuel0% (1)
- A Step by Step Guide To Building Your Own Online Income!: 2010 EditionDocument139 pagesA Step by Step Guide To Building Your Own Online Income!: 2010 EditionJfoxx SamuelNo ratings yet
- CAPE Biology-June 2007 SyllabusDocument55 pagesCAPE Biology-June 2007 Syllabusmegs1622No ratings yet
- Edexcel IGCSE Biology Revision Notes (Download From WWW - Shawonnotes.com)Document65 pagesEdexcel IGCSE Biology Revision Notes (Download From WWW - Shawonnotes.com)Hadi Alnaher75% (4)
- Corrected 1041 File Part 1Document160 pagesCorrected 1041 File Part 1walebayo06No ratings yet
- Acute GlomerulonephritisDocument28 pagesAcute GlomerulonephritisPaul SinsNo ratings yet
- Excretory Products and Their EliminationDocument9 pagesExcretory Products and Their EliminationBiju MylachalNo ratings yet
- Atypical Renal Presentation in Severe LeptospirosisDocument3 pagesAtypical Renal Presentation in Severe LeptospirosisADINo ratings yet
- Manual For Medical RepresentativesDocument74 pagesManual For Medical RepresentativesSyedMaqboolRaza100% (2)
- AUBF Reinforcement ExamDocument67 pagesAUBF Reinforcement ExamVanessa May BlancioNo ratings yet
- MS RENALdkcsDocument25 pagesMS RENALdkcsEmeroot RootNo ratings yet
- Dialysis PresentationDocument21 pagesDialysis PresentationRon Anderson100% (1)
- Biology SPM 2020 Model Answers For Predicted QuestionsDocument30 pagesBiology SPM 2020 Model Answers For Predicted Questionskumarantuition100% (1)
- Bio 235 F 12 Final Exam AnswersDocument12 pagesBio 235 F 12 Final Exam AnswersSmartunblurrNo ratings yet
- A Note Pre MedDocument24 pagesA Note Pre Medwan amiera wan malekNo ratings yet
- Renal SystemDocument85 pagesRenal SystemFerasKarajehNo ratings yet
- Anatomy and Physiology of Urinary SystemDocument36 pagesAnatomy and Physiology of Urinary Systemdyah rochmawatiNo ratings yet
- Urinary SystemDocument55 pagesUrinary SystemDiamante MhayaleneNo ratings yet
- Biology Paper 4 Theory Samuel Sierra 11CDocument22 pagesBiology Paper 4 Theory Samuel Sierra 11CGabriela TrujilloNo ratings yet
- HematuriaDocument86 pagesHematuriaMohamad Arif MustaphaNo ratings yet
- Cystatin CDocument4 pagesCystatin CГалина МиловановаNo ratings yet
- Toxic Response of The KidneyDocument22 pagesToxic Response of The KidneyKhara TeanoTanNo ratings yet
- Albumin in Urine/CSF FS : (Microalbumin)Document2 pagesAlbumin in Urine/CSF FS : (Microalbumin)Khuon BunthaNo ratings yet
- 3f Aubf Lec Renal Function Tests PDFDocument11 pages3f Aubf Lec Renal Function Tests PDFBanana QNo ratings yet
- Bence JonesDocument5 pagesBence JonesChristian Eduard de Dios100% (1)
- Renal Physiology PDFDocument12 pagesRenal Physiology PDFLolitaNo ratings yet
- Life ProcessesDocument49 pagesLife ProcessesKaushal SolankeNo ratings yet