Download as pdf or txt
You might also like
- DSM 5 DiagnosesDocument1 pageDSM 5 DiagnosesGen Feliciano100% (4)
- Joel Paris-The Intelligent Clinician's Guide To The DSM-5®-Oxford University Press (2013)Document265 pagesJoel Paris-The Intelligent Clinician's Guide To The DSM-5®-Oxford University Press (2013)JC Barrientos100% (10)
- DSM 5 SummaryDocument61 pagesDSM 5 Summaryroxxifoxxi88% (16)
- Mental Health NotesDocument21 pagesMental Health Notesbazahoor97% (35)
- DSM 5 ChartDocument2 pagesDSM 5 ChartJanie VandeBerg93% (28)
- DSM 5 - DSM 5Document7 pagesDSM 5 - DSM 5Roxana ClsNo ratings yet
- Diagnostic System: Why the Classification of Psychiatric Disorders Is Necessary, Difficult, and Never SettledFrom EverandDiagnostic System: Why the Classification of Psychiatric Disorders Is Necessary, Difficult, and Never SettledNo ratings yet
- English 9 Activity Sheet: Quarter 3 - MELC 3Document9 pagesEnglish 9 Activity Sheet: Quarter 3 - MELC 3rai genolos67% (9)
- Site Specific Health Safety Environment Plan HvacDocument74 pagesSite Specific Health Safety Environment Plan Hvacsyed khaja misbhuddin100% (1)
- Case of JessicaDocument2 pagesCase of JessicaElaine Joyce PasiaNo ratings yet
- Writing DSM 5 DiagnosisDocument2 pagesWriting DSM 5 Diagnosiscristina83% (6)
- The Wiley Handbook of Cognitive Behavioral Therapy (2013) PDFDocument1,388 pagesThe Wiley Handbook of Cognitive Behavioral Therapy (2013) PDFIoana Jigau75% (4)
- Psych CardsDocument10 pagesPsych CardsJennifer Rodriguez96% (25)
- DSM-5 Survival Guide Formatted Final PDFDocument73 pagesDSM-5 Survival Guide Formatted Final PDFLuke Bacon100% (2)
- Handbook of Psychological AssessmentDocument843 pagesHandbook of Psychological AssessmentRolly Zsigmond75% (4)
- DSM 5 ChartDocument7 pagesDSM 5 ChartJose Luis Gonzalez Celis100% (1)
- DSM IvDocument915 pagesDSM Ivtitahvega100% (32)
- DSM VDocument9 pagesDSM VAddie Espiritu100% (4)
- Certified Mental Health Counselor: Passbooks Study GuideFrom EverandCertified Mental Health Counselor: Passbooks Study GuideNo ratings yet
- Structured Clinical Interview For The DSM-IV Axis I Disorders (SCID PTSD Module)Document2 pagesStructured Clinical Interview For The DSM-IV Axis I Disorders (SCID PTSD Module)Doomimummo100% (1)
- Standard 2-Family ScenariosDocument13 pagesStandard 2-Family Scenariosapi-249216975No ratings yet
- DSM 5 EssentialsDocument8 pagesDSM 5 EssentialsAlyssa Gervacio100% (2)
- Suicide Risk Assessment Summary.08Document1 pageSuicide Risk Assessment Summary.08Pintiliciuc-aga MihaiNo ratings yet
- The Dsm-5 Survival Guide: a Navigational Tool for Mental Health ProfessionalsFrom EverandThe Dsm-5 Survival Guide: a Navigational Tool for Mental Health ProfessionalsRating: 3 out of 5 stars3/5 (2)
- DSM 5 Cross Cutting Over ViewDocument9 pagesDSM 5 Cross Cutting Over Viewapi-4201886000% (1)
- Personalitydisorders Gabbard PDFDocument3 pagesPersonalitydisorders Gabbard PDFmkecikNo ratings yet
- DSM V at A GlanceDocument39 pagesDSM V at A GlanceSubas Pradhan100% (6)
- Charles Scott-DSM-5® and The Law - Changes and Challenges-Oxford University Press (2015) PDFDocument305 pagesCharles Scott-DSM-5® and The Law - Changes and Challenges-Oxford University Press (2015) PDFfpsearhiva personala100% (3)
- DSM 5 Update 2016Document33 pagesDSM 5 Update 2016Monica Putri Damayanti100% (1)
- Psychiatric Clinical SkillsDocument376 pagesPsychiatric Clinical SkillsSamuel Agunbiade100% (5)
- HTTP WWW - Nami.org Template - CFM Section Borderline Personality Disorder (BPD) &template ContentManagement ContentDisplayDocument20 pagesHTTP WWW - Nami.org Template - CFM Section Borderline Personality Disorder (BPD) &template ContentManagement ContentDisplayCorina MihaelaNo ratings yet
- DSM-5 LCA Case Formulation Rev.Document31 pagesDSM-5 LCA Case Formulation Rev.Khadeeja Rana100% (3)
- Practice Guidelines For Psychiatric Consultation in The General Medical SettingDocument23 pagesPractice Guidelines For Psychiatric Consultation in The General Medical Settingpsychforall100% (1)
- Handouts Practice ExercisesDocument14 pagesHandouts Practice ExercisesAdan InzunzaNo ratings yet
- Abnormal Psychology VocabularyDocument5 pagesAbnormal Psychology VocabularyMelanie Blankenship100% (1)
- Chapter 1 - What Is BiopsychologyDocument32 pagesChapter 1 - What Is BiopsychologyKaren Mari0% (1)
- Behavioral Guide To Personality Disorders - (DSM-5) (2015) by Douglas H. RubenDocument275 pagesBehavioral Guide To Personality Disorders - (DSM-5) (2015) by Douglas H. RubenCristianBale100% (9)
- Forensic Psychology and Correctional PsychologyDocument41 pagesForensic Psychology and Correctional PsychologyLorena Rodríguez100% (2)
- Psychological Disorder Quiz Key sp15Document3 pagesPsychological Disorder Quiz Key sp15api-2612679760% (3)
- Conversion Disorder TreatmentDocument9 pagesConversion Disorder Treatmentapi-241111102No ratings yet
- DSM V PDFDocument33 pagesDSM V PDFRizky YantoroNo ratings yet
- Assessment of Children and AdolescentsDocument17 pagesAssessment of Children and AdolescentsadrianaNo ratings yet
- Recommended Texts and Useful Resources For Psychiatry Trainees (2019)Document6 pagesRecommended Texts and Useful Resources For Psychiatry Trainees (2019)Ave Claudiu100% (2)
- Borderline Personality DisorderDocument2 pagesBorderline Personality DisorderIeternalleo100% (1)
- Borderline Personality DisorderDocument6 pagesBorderline Personality DisorderPersephona13No ratings yet
- Theories of AggressionDocument22 pagesTheories of Aggressiongirploom100% (1)
- The Five-Factor Model of Personality Disorder and DSM-5Document24 pagesThe Five-Factor Model of Personality Disorder and DSM-5Lucas SouzaNo ratings yet
- Assessment of MalingeringDocument12 pagesAssessment of MalingeringkosmicNo ratings yet
- Motivational Interviewing (MI) Refers To ADocument5 pagesMotivational Interviewing (MI) Refers To AJefri JohanesNo ratings yet
- Fact Sheet ASD DSM-5Document2 pagesFact Sheet ASD DSM-5Tony BeresNo ratings yet
- Adult Psychopathology, Second Edition: A Social Work PerspectiveFrom EverandAdult Psychopathology, Second Edition: A Social Work PerspectiveRating: 4 out of 5 stars4/5 (5)
- DBT Workshop PDFDocument36 pagesDBT Workshop PDFNica Nario Asuncion100% (2)
- ASWB EXAMINATION IN SOCIAL WORK [ASWB] (1 VOL.): Passbooks Study GuideFrom EverandASWB EXAMINATION IN SOCIAL WORK [ASWB] (1 VOL.): Passbooks Study GuideNo ratings yet
- Psychotherapist'S Guide To Psychopharmacology: Second EditionFrom EverandPsychotherapist'S Guide To Psychopharmacology: Second EditionRating: 5 out of 5 stars5/5 (6)
- An Overview of Psychopathology: by Arlin Cuncic Updated February 05, 2019Document14 pagesAn Overview of Psychopathology: by Arlin Cuncic Updated February 05, 2019Andrea González100% (3)
- Autism, PDD-NOS & Asperger's Fact Sheets A Guide To Classification and Diagnosis of Autism and Asperger's SyndromeDocument2 pagesAutism, PDD-NOS & Asperger's Fact Sheets A Guide To Classification and Diagnosis of Autism and Asperger's SyndromethenmeunseenNo ratings yet
- Mood Disorders: Jaycee M. Delos SantosDocument48 pagesMood Disorders: Jaycee M. Delos SantosDerek Walker100% (4)
- ADHD Screening in AdultsDocument3 pagesADHD Screening in AdultsPanduRespatiNo ratings yet
- DSM-5 Personality DisordersDocument2 pagesDSM-5 Personality DisordersIqbal BaryarNo ratings yet
- Leslie Estrada-Sandoval - Personal Statement 1Document3 pagesLeslie Estrada-Sandoval - Personal Statement 1api-719526054No ratings yet
- Chain Exercise Terhadap Penurunan Intensitas Nyeri Pada LansiaDocument9 pagesChain Exercise Terhadap Penurunan Intensitas Nyeri Pada LansiaFitria NHNo ratings yet
- Pma Memo No 2022 10 24 020Document9 pagesPma Memo No 2022 10 24 020Emma AustriaNo ratings yet
- Grande MultiparaDocument6 pagesGrande MultiparaAgus Wijaya100% (2)
- Classification of Proteins and Their Functions PDFDocument1 pageClassification of Proteins and Their Functions PDFConfidentro BlospotNo ratings yet
- En - Avol Oxy White - 10Document9 pagesEn - Avol Oxy White - 10Twaha M&SNo ratings yet
- Const221 Document caughtInHazardsAccessibleDocument22 pagesConst221 Document caughtInHazardsAccessiblelurawi2023No ratings yet
- BODY Valiao SemiDocument38 pagesBODY Valiao SemiMay Chelle ErazoNo ratings yet
- Communication Skills in MedicineDocument5 pagesCommunication Skills in MedicineSGD blima semlimanamNo ratings yet
- Test Bank Interpersonal Relationships 7th Edition Boggs ArnoldDocument24 pagesTest Bank Interpersonal Relationships 7th Edition Boggs ArnoldRyanMillertxip100% (39)
- EU - Guidance On GMP For Food Contact Plastic Materials and Articles (60p)Document60 pagesEU - Guidance On GMP For Food Contact Plastic Materials and Articles (60p)Kram NawkNo ratings yet
- ReflectionDocument1 pageReflectionRIMANDO LAFUENTENo ratings yet
- Passive Voice - HSDocument9 pagesPassive Voice - HSKhôi Nguyên ĐặngNo ratings yet
- Carbohydrate-Related Diseases Term PaperDocument5 pagesCarbohydrate-Related Diseases Term Paperheiress comiaNo ratings yet
- From Start To Phase 1 in 30 Months - Insilico MedicineDocument9 pagesFrom Start To Phase 1 in 30 Months - Insilico MedicinejeanNo ratings yet
- Read Online Textbook Behavior Modification What It Is and How To Do It 10Th Edition Garry Martin Ebook All Chapter PDFDocument22 pagesRead Online Textbook Behavior Modification What It Is and How To Do It 10Th Edition Garry Martin Ebook All Chapter PDFhilda.rufe918100% (2)
- Transkrip Sementara Universitas Wahid Hasyim: (Certificate of Establishment)Document3 pagesTranskrip Sementara Universitas Wahid Hasyim: (Certificate of Establishment)Lailatuz ZakiyahNo ratings yet
- Health Declaration and Screening Form For Pedia VaxDocument1 pageHealth Declaration and Screening Form For Pedia VaxMark Lawrence Bael0% (1)
- English Level 4 Writing ProjectDocument5 pagesEnglish Level 4 Writing ProjectvalentinaNo ratings yet
- 2018-089. NASKAH PUBLIKASI Elsi Nursyahdin MayaranaDocument12 pages2018-089. NASKAH PUBLIKASI Elsi Nursyahdin MayaranaElsi NursyahdinNo ratings yet
- HEADSS AssessmentDocument3 pagesHEADSS AssessmentjonnyjhartNo ratings yet
- Efusi PleuraDocument26 pagesEfusi PleuraAhmad Isyai RamadhanNo ratings yet
- Community Health Nursing Part 1 & 2Document35 pagesCommunity Health Nursing Part 1 & 2mark OrpillaNo ratings yet
- History TakingDocument51 pagesHistory TakingJAMES TONNY OKINYINo ratings yet
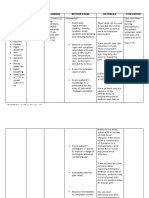
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument5 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationArian May MarcosNo ratings yet
- Scba-Sample CertDocument2 pagesScba-Sample CertSHAHID KHAN CHANNARNo ratings yet
- (Final) 2023 SGLGB Form 2-Data Capture Form (DCF)Document36 pages(Final) 2023 SGLGB Form 2-Data Capture Form (DCF)Rosalie T. Orbon-Tamondong100% (2)






















































![ASWB EXAMINATION IN SOCIAL WORK [ASWB] (1 VOL.): Passbooks Study Guide](https://imgv2-1-f.scribdassets.com/img/word_document/402068986/149x198/afec08b5ad/1718643612?v=1)