Download as ppt, pdf, or txt
You might also like
- Robbins Pathology Chapter 13 - White Blood CellsDocument7 pagesRobbins Pathology Chapter 13 - White Blood Cellsscorpiosphinx7980% (5)
- Science Olympiad 2020 Cheat SheetDocument4 pagesScience Olympiad 2020 Cheat SheetLisa RetbergNo ratings yet
- Tissue CTDocument1 pageTissue CTAditi MishraNo ratings yet
- Cheat Sheet Integumentary SystemDocument4 pagesCheat Sheet Integumentary SystemLisa RetbergNo ratings yet
- 1358453842.3856hematology Question BankDocument182 pages1358453842.3856hematology Question BankKay BristolNo ratings yet
- Anaemia in CatsDocument9 pagesAnaemia in CatsPavel VokrouhlíkNo ratings yet
- Bone Marrow TransplantDocument4 pagesBone Marrow TransplantRea Ann Autor LiraNo ratings yet
- Lecture Guide Assessment-Of-Musculoskeletal-Function HPDocument85 pagesLecture Guide Assessment-Of-Musculoskeletal-Function HPBlessed GarcianoNo ratings yet
- Skeletal SystemDocument117 pagesSkeletal Systemsam bossaNo ratings yet
- Chapter 6 Bone Tissue 2304Document37 pagesChapter 6 Bone Tissue 2304Sav Oli100% (1)
- Anatomy 1.02 Axial SkeletonDocument8 pagesAnatomy 1.02 Axial SkeletonMark AbrazaldoNo ratings yet
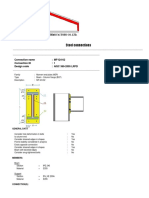
- Steel Connections: Connection Name: MF-I24-02 Connection ID: 1 Design Code: AISC 360-2005 LRFDDocument12 pagesSteel Connections: Connection Name: MF-I24-02 Connection ID: 1 Design Code: AISC 360-2005 LRFDmalikasalNo ratings yet
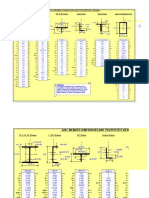
- AISC Properties MM GPP 2017Document87 pagesAISC Properties MM GPP 2017Pablo García PeñaNo ratings yet
- Shear Wave PDFDocument6 pagesShear Wave PDFcutefrenzyNo ratings yet
- Arc Welding ReadingDocument16 pagesArc Welding ReadingJessica S. MellNo ratings yet
- ISO 3834purchasedocumentDocument8 pagesISO 3834purchasedocumenthector-salomonNo ratings yet
- Geometrical TolerancingDocument12 pagesGeometrical TolerancingItalo Venegas100% (1)
- Metrology Lab w2014Document15 pagesMetrology Lab w2014ObaidNo ratings yet
- AWS Catalog 2017 Winter SpringDocument52 pagesAWS Catalog 2017 Winter SpringPilar Medrano MenaNo ratings yet
- How To Specify Fasteners: 3/4 - 10 X 5 Hex Cap Screw Grade 5 Zinc 3/4 - 16 X 5 Hex Cap Screw Grade 5 ZincDocument15 pagesHow To Specify Fasteners: 3/4 - 10 X 5 Hex Cap Screw Grade 5 Zinc 3/4 - 16 X 5 Hex Cap Screw Grade 5 ZincAndré BuysNo ratings yet
- MODULE 4 Skeletal SystemDocument16 pagesMODULE 4 Skeletal SystemKate Andrea PanizalesNo ratings yet
- Simboluri SudareDocument8 pagesSimboluri SudarecornelutsNo ratings yet
- Do Now: Observe The Following Slide. Identify The Type of Epithelium Present. What Else Is Present in This Slide?Document27 pagesDo Now: Observe The Following Slide. Identify The Type of Epithelium Present. What Else Is Present in This Slide?oomphaloomphaNo ratings yet
- Classification of Joints 1Document30 pagesClassification of Joints 1Asmat Ullah QureshiNo ratings yet
- Chapter 16 Anatomy of The HeartDocument5 pagesChapter 16 Anatomy of The Heartphotojockey18No ratings yet
- Types of Tissues: Lesson 02Document33 pagesTypes of Tissues: Lesson 02DASH100% (2)
- General Pathology, Histopathologic and Cytologic TechniquesDocument28 pagesGeneral Pathology, Histopathologic and Cytologic TechniquesMarl EstradaNo ratings yet
- Bone Joint Cartilage PowerpointDocument81 pagesBone Joint Cartilage PowerpointChevie WisemanNo ratings yet
- The Nelson System Catalouge Version 2 2017 Shear StudsDocument8 pagesThe Nelson System Catalouge Version 2 2017 Shear StudsMacNo ratings yet
- 16.classification of JointsDocument19 pages16.classification of JointsdenekeNo ratings yet
- Introduction To Non-Destructive TestingDocument34 pagesIntroduction To Non-Destructive Testingegy pure100% (1)
- Lecture 2 - OsteologyDocument66 pagesLecture 2 - OsteologyRubia Iftikhar100% (1)
- CartilageDocument12 pagesCartilageReycy Ruth Trivino100% (1)
- Guidelines Citopathology 2009Document7 pagesGuidelines Citopathology 2009Fabrício CamargoNo ratings yet
- Structures and Functions of Animal Tissues and Cell ModificationDocument105 pagesStructures and Functions of Animal Tissues and Cell ModificationArvie Jay Castillo100% (1)
- Connective TissueDocument14 pagesConnective TissueDr NehaNo ratings yet
- Tereos - Structure of PresentationDocument72 pagesTereos - Structure of PresentationSumitNo ratings yet
- H4L StudDocument1 pageH4L StudisracumaNo ratings yet
- AWS Weld Symbol BasicsDocument3 pagesAWS Weld Symbol Basicschairul anwarNo ratings yet
- Applicable ASTM Specifications For Structural Fasteners: Table 3.8 Anchor RodsDocument1 pageApplicable ASTM Specifications For Structural Fasteners: Table 3.8 Anchor Rodsivan bolañosNo ratings yet
- Skeletal Anatomy NotesDocument7 pagesSkeletal Anatomy NotesalchriwNo ratings yet
- Histology Practical Manual Part 1 2021Document124 pagesHistology Practical Manual Part 1 2021khushikumari1407No ratings yet
- Skeletal - System AnatomyDocument89 pagesSkeletal - System AnatomysanayaNo ratings yet
- Bone Surface MarkingsDocument2 pagesBone Surface MarkingsNurul Afiqah Fattin AmatNo ratings yet
- Care & Cleaning - Stainless Steel PDFDocument7 pagesCare & Cleaning - Stainless Steel PDFpsp710No ratings yet
- Bones of The Upper LimbDocument27 pagesBones of The Upper LimbFoday H Kalokoh100% (1)
- Lecture 2 BoneDocument22 pagesLecture 2 BoneiamkpvemuriNo ratings yet
- SteelDocument22 pagesSteels63et79jgeesdgNo ratings yet
- 2015 KOBELCO Defect PDFDocument25 pages2015 KOBELCO Defect PDFayushNo ratings yet
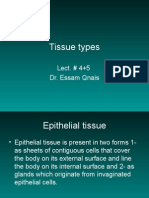
- 4+5 Tissue Types and Epithelial TissueDocument44 pages4+5 Tissue Types and Epithelial Tissueyasser100% (2)
- Bone Tissues 1Document38 pagesBone Tissues 1ms_pianist100% (1)
- 2 - Bones of The Lower LimbDocument23 pages2 - Bones of The Lower LimbHamzaNo ratings yet
- Bone TissueDocument66 pagesBone TissueFunikawati Baldiyah100% (1)
- Bone TissueDocument66 pagesBone TissueWalter Macasiano GravadorNo ratings yet
- Musculoskeletal Anatomy and Physiology 4Document67 pagesMusculoskeletal Anatomy and Physiology 4Dennis Nabor Muñoz, RN,RM100% (1)
- Histology of A BoneDocument26 pagesHistology of A BoneAmanuel MaruNo ratings yet
- Musculoskeletal System-Topic 8Document40 pagesMusculoskeletal System-Topic 8Heba TabchNo ratings yet
- 7.0 Skeletal SystemDocument45 pages7.0 Skeletal System[R2A] Khadijah Azlan100% (1)
- Dr. Sassia Lecture Bone Histology Part I June 2023Document45 pagesDr. Sassia Lecture Bone Histology Part I June 2023Ali ELKARGHALYNo ratings yet
- Biol 111-Bones and Skeletal Tissue Part 1Document58 pagesBiol 111-Bones and Skeletal Tissue Part 1Jaedon AdamsNo ratings yet
- ALVEOLAR BoneDocument72 pagesALVEOLAR BoneArchana50% (2)
- Skeletal - System AnatomyDocument130 pagesSkeletal - System Anatomyhamnafaisall8No ratings yet
- 07 Cartilage and Bone 2022Document64 pages07 Cartilage and Bone 2022A. AsadiNo ratings yet
- Overview of The Musculoskeletal System: For Year 1 Medicine By: Zelalem.aDocument36 pagesOverview of The Musculoskeletal System: For Year 1 Medicine By: Zelalem.aAmanuel MaruNo ratings yet
- Typhoon Ulysses ImpactDocument1 pageTyphoon Ulysses ImpactDenver Tanhuan100% (1)
- Four Fundamental Elements 01Document1 pageFour Fundamental Elements 01Denver TanhuanNo ratings yet
- BiospyDocument2 pagesBiospyDenver TanhuanNo ratings yet
- Conduct and TestDocument1 pageConduct and TestDenver TanhuanNo ratings yet
- Novenas and PrayersDocument5 pagesNovenas and PrayersDenver TanhuanNo ratings yet
- Rmo 5 2012Document2 pagesRmo 5 2012Denver TanhuanNo ratings yet
- MedicineDocument1 pageMedicineDenver TanhuanNo ratings yet
- Lease Bonus Paidby The Lessee Treatment)Document2 pagesLease Bonus Paidby The Lessee Treatment)Denver TanhuanNo ratings yet
- 332-032431 MarrowMAX PDFDocument2 pages332-032431 MarrowMAX PDFMeera SainiNo ratings yet
- Flow Cytometry CD45 Gating For Immunophenotyping of Acute Myeloid LeukemiaDocument9 pagesFlow Cytometry CD45 Gating For Immunophenotyping of Acute Myeloid LeukemiaKATHERINE ALEXANDRA ESCARRAGA CORREALNo ratings yet
- Chronic Lymphocytic LeukemiaDocument6 pagesChronic Lymphocytic LeukemiaJhannNo ratings yet
- On LeukemiaDocument28 pagesOn LeukemiaMeena Koushal100% (1)
- Keganasan HematologiDocument26 pagesKeganasan HematologiRizzal Selviyana SuhardiNo ratings yet
- MUST To KNOW in HematologyDocument44 pagesMUST To KNOW in HematologyJan Joseph YbañezNo ratings yet
- Laringomalacia - Nursing CareDocument9 pagesLaringomalacia - Nursing CareRirin Muthia ZukhraNo ratings yet
- Bone Marrow FailureDocument2 pagesBone Marrow FailureGerardLum100% (1)
- Oral Path2013 14Document367 pagesOral Path2013 14Vladimir Argirovic100% (4)
- Human Histology Midterms: Blood and HemopoesisDocument3 pagesHuman Histology Midterms: Blood and Hemopoesisabi dimatulacNo ratings yet
- HEMATOPOIESIS StudentsDocument50 pagesHEMATOPOIESIS Studentskimberly abianNo ratings yet
- Hematology 1 PrelimsDocument19 pagesHematology 1 Prelimsella SyNo ratings yet
- Basic Immunology PDFDocument6 pagesBasic Immunology PDFAnastasia ENo ratings yet
- HemoblastosisDocument18 pagesHemoblastosisMechkar Katherin0% (1)
- 10 On 2020 HSCT WBDocument94 pages10 On 2020 HSCT WBabdullahNo ratings yet
- Aplastic AnemiaDocument26 pagesAplastic AnemiaIrina Moldovan100% (1)
- Pure Red Cell Aplasia PRCADocument14 pagesPure Red Cell Aplasia PRCANikkiRoxasNo ratings yet
- Module 2 CANVAS NOTES HematopoiesisDocument6 pagesModule 2 CANVAS NOTES HematopoiesisMohammad MasacalNo ratings yet
- Sead Ferizovic BrochureDocument2 pagesSead Ferizovic BrochureNedim VrtagicNo ratings yet
- Melanie - OncoDocument91 pagesMelanie - OncoDefensor Pison GringgoNo ratings yet
- Hemopoiesis PDFDocument14 pagesHemopoiesis PDFrysnawahyu13No ratings yet
- Hematological Systems - Lecture NotesDocument15 pagesHematological Systems - Lecture NotesAmiel Francisco ReyesNo ratings yet
- Clinico-Aetiological Profile of Pancytopenia in Paediatric PracticeDocument4 pagesClinico-Aetiological Profile of Pancytopenia in Paediatric PracticeDesi AdiyatiNo ratings yet
- Assisting in BMA Procedure GuideDocument2 pagesAssisting in BMA Procedure GuideKisha BethelNo ratings yet
- Karp CH 1Document17 pagesKarp CH 1mikadeguzman100% (1)
- Bone Marrow-Hypocellularity 508Document6 pagesBone Marrow-Hypocellularity 508Islam AhmedNo ratings yet