
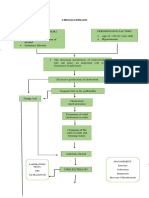
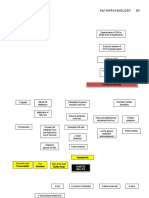
Schistosomiasis (From Anatomy To Pathophysiology)
Schistosomiasis (From Anatomy To Pathophysiology)
You might also like
- MedSurg Notes - Cancer of The LiverDocument2 pagesMedSurg Notes - Cancer of The LiverMae CeaesarNo ratings yet
- Urinary Tract Infection Anatomy and PhysiologyDocument12 pagesUrinary Tract Infection Anatomy and PhysiologyPaul Anthony Centeno PimentelNo ratings yet
- Cardiology Case 1Document2 pagesCardiology Case 1vil62650% (2)
- Patho UGIBDocument3 pagesPatho UGIBKristineBungcagNo ratings yet
- The Filipino FamilyDocument11 pagesThe Filipino FamilyTiger Knee97% (38)
- Pathophysiology of Heart FailureDocument4 pagesPathophysiology of Heart FailureTiger Knee100% (2)
- The Development of The Middle Ear Spaces and Their Surgical SignificanceDocument15 pagesThe Development of The Middle Ear Spaces and Their Surgical SignificanceDrTarek Mahmoud Abo Kammer100% (2)
- Microbiology-ELISA Testing Lab ReportDocument2 pagesMicrobiology-ELISA Testing Lab Reportsaraebo33% (3)
- ABRUPTIO PLACENTAE PathophysiologyDocument3 pagesABRUPTIO PLACENTAE PathophysiologyBarda GulanNo ratings yet
- Pathophysiology of Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar Nonketotic Syndrome EtiologyDocument2 pagesPathophysiology of Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar Nonketotic Syndrome EtiologyJaylord VerazonNo ratings yet
- Esophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNDocument20 pagesEsophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNAnn SalvatierraNo ratings yet
- Vii. Pathophysiology A. AlgorithmDocument2 pagesVii. Pathophysiology A. AlgorithmJonna Mae TurquezaNo ratings yet
- Cholelithiasis PathophysiologyDocument2 pagesCholelithiasis PathophysiologyShinrin SukehiroNo ratings yet
- Case Study AGE With Signs of DehydrationDocument27 pagesCase Study AGE With Signs of DehydrationZhenmeiNo ratings yet
- B. Pathophysiology Diagram: A Case Study On UreterolithiasisDocument5 pagesB. Pathophysiology Diagram: A Case Study On UreterolithiasisIan Mizzel A. DulfinaNo ratings yet
- Pathophysiology of Atrial Septal DefectDocument2 pagesPathophysiology of Atrial Septal Defectbobtaguba50% (2)
- Action Plan - Inadequate IncomeDocument2 pagesAction Plan - Inadequate IncomeBenedict James BermasNo ratings yet
- Blood Dyscrasia SDocument24 pagesBlood Dyscrasia SMasha FloreaNo ratings yet
- Case Study Benign Tumors of The Uterus: MyomaDocument3 pagesCase Study Benign Tumors of The Uterus: MyomaToto RyanNo ratings yet
- Pathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsDocument4 pagesPathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsLovely DaroleNo ratings yet
- Cva Concept MapDocument1 pageCva Concept MapAnn Justine OrbetaNo ratings yet
- Acute Cholecystolithiasis - G4 SB2Document125 pagesAcute Cholecystolithiasis - G4 SB2Jeofy PamaNo ratings yet
- PYOMYOSITISDocument6 pagesPYOMYOSITISChristine CoridoNo ratings yet
- DB13 - Pathophysiology of AtherosclerosisDocument2 pagesDB13 - Pathophysiology of Atherosclerosisi_vhie03No ratings yet
- Chronic PyelonephritisDocument5 pagesChronic PyelonephritisIsak ShatikaNo ratings yet
- Pathophysiology of Urinary Tract ObstructionDocument50 pagesPathophysiology of Urinary Tract ObstructionPryo UtamaNo ratings yet
- Acute PyelonephritisDocument105 pagesAcute Pyelonephritisyasira50% (2)
- Pathophysiology of Inflammatory ResponseDocument1 pagePathophysiology of Inflammatory ResponseDeo FactuarNo ratings yet
- V. Pathophysiology Modifiable: Non - ModifiableDocument2 pagesV. Pathophysiology Modifiable: Non - ModifiableMary Grace BanezNo ratings yet
- NSTEMIDocument33 pagesNSTEMIwaazalimahwahidNo ratings yet
- AGE With Pa Tho PhysiologyDocument3 pagesAGE With Pa Tho PhysiologyChichi Licuben OresacamNo ratings yet
- Pathophysiology (Client Base) :: Predisposing Factors: Precipitating FactorsDocument1 pagePathophysiology (Client Base) :: Predisposing Factors: Precipitating Factorsleslie_macasaetNo ratings yet
- Path o PhysiologyDocument9 pagesPath o PhysiologyKyle Ü D. CunanersNo ratings yet
- Tuberculosis PathophysiologyDocument1 pageTuberculosis Pathophysiologymiss RN100% (15)
- Cancer of The ColonDocument8 pagesCancer of The Colonnot your medz duranNo ratings yet
- Diabetes PathoDocument2 pagesDiabetes Pathodrewcel100% (1)
- Pathophysiology Cushing S SyndromeDocument4 pagesPathophysiology Cushing S SyndromeMaria Luisa VillalunaNo ratings yet
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyDocument3 pages"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyCarl Elexer Cuyugan Ano50% (2)
- Pyloric StenosisDocument5 pagesPyloric Stenosisensoooooooooo100% (1)
- Pathophysiology: Prince Carl P. Magluyan BSN - 2GDocument1 pagePathophysiology: Prince Carl P. Magluyan BSN - 2GPrinceNo ratings yet
- Case Presentation of Acute PyelonephritisDocument1 pageCase Presentation of Acute PyelonephritisANALYN ANUBNo ratings yet
- Pernicious AnemiaDocument7 pagesPernicious AnemiaTracy PearlNo ratings yet
- Biomedical Case StudyDocument5 pagesBiomedical Case StudyHannan AtharNo ratings yet
- Pathophysiology-Kni Ns PLZZZDocument8 pagesPathophysiology-Kni Ns PLZZZAnna Lira Manluyang MungcalNo ratings yet
- Hydronephrosis Fred LuceDocument69 pagesHydronephrosis Fred LuceKMNo ratings yet
- Anal Canal: Fissure in Ano HaemorrhoidsDocument37 pagesAnal Canal: Fissure in Ano Haemorrhoidsyash shrivastavaNo ratings yet
- NCP LeukemiaDocument5 pagesNCP LeukemiaTriciaNo ratings yet
- Abruptio PlacentaDocument3 pagesAbruptio Placentachichilovesyou100% (1)
- Venous Thromboembolism (VTE) - McMaster Pathophysiology ReviewDocument9 pagesVenous Thromboembolism (VTE) - McMaster Pathophysiology ReviewFadiyah UlfahNo ratings yet
- Pharmacology m7 Post Task CaparasDocument3 pagesPharmacology m7 Post Task CaparasGretta CaparasNo ratings yet
- Neonatal HyperbilirubinemiaDocument22 pagesNeonatal HyperbilirubinemiaAnkur WadheraNo ratings yet
- Case Study - Dengue Fever V - S UtiDocument12 pagesCase Study - Dengue Fever V - S UtiHarlene Joyce ReyNo ratings yet
- Rheumatic Heart DiseaseDocument3 pagesRheumatic Heart DiseaseDee SarajanNo ratings yet
- Anatomy and Physiology of The GallbladderDocument1 pageAnatomy and Physiology of The GallbladderRojanisa Baculi RomathoNo ratings yet
- PATHOPHYSIOLOGYDocument1 pagePATHOPHYSIOLOGYJeroham CoNo ratings yet
- Normal Values of CBCDocument1 pageNormal Values of CBCCherr NollNo ratings yet
- CPD Concept MapDocument1 pageCPD Concept MapShandle Dynne Baena100% (1)
- Case (Acute Gastroenteritis) Group 4Document36 pagesCase (Acute Gastroenteritis) Group 4EljhayrosNo ratings yet
- NCP CvaDocument4 pagesNCP CvaMariquita BuenafeNo ratings yet
- Malaria: Pathophysiology, Clinical Manifesta6ons and TreatmentDocument14 pagesMalaria: Pathophysiology, Clinical Manifesta6ons and TreatmentGuilhermeNo ratings yet
- CKD - For Concept MappingDocument7 pagesCKD - For Concept MappingKennette Lim0% (1)
- Assessment Nsg. Diagnosis Sci. Explanation Planning Intervention Rationale EvaluationDocument6 pagesAssessment Nsg. Diagnosis Sci. Explanation Planning Intervention Rationale EvaluationRoMarie AbainzaNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Specpro DigestsDocument9 pagesSpecpro DigestsTiger KneeNo ratings yet
- G.R. Nos. 197592 & 20262 November 27, 2013 The Province of Aklan, Petitioner, Jody King Construction and Development Corp., RespondentDocument33 pagesG.R. Nos. 197592 & 20262 November 27, 2013 The Province of Aklan, Petitioner, Jody King Construction and Development Corp., RespondentTiger KneeNo ratings yet
- Breast Cancer AssignmentDocument25 pagesBreast Cancer AssignmentTiger KneeNo ratings yet
- Logic AnswersDocument3 pagesLogic AnswersTiger KneeNo ratings yet
- Voting Number in The ConstitutionDocument2 pagesVoting Number in The ConstitutionTiger KneeNo ratings yet
- Fundamental Distinctions Among Leasehold Tenancy, Tenant Emancipation Decree and CARPDocument17 pagesFundamental Distinctions Among Leasehold Tenancy, Tenant Emancipation Decree and CARPTiger KneeNo ratings yet
- Mens MonthDocument1 pageMens MonthTiger KneeNo ratings yet
- Marriage SettlementsDocument4 pagesMarriage SettlementsTiger KneeNo ratings yet
- Rule 105 Special ProceedingDocument3 pagesRule 105 Special ProceedingTiger KneeNo ratings yet
- Amendments To The Rules of Court On Declaration of Absolute Nullity of Marriage Etc...Document10 pagesAmendments To The Rules of Court On Declaration of Absolute Nullity of Marriage Etc...Tiger KneeNo ratings yet
- Synthesis Paper On The Framework For Pathophysiology: EtiologyDocument4 pagesSynthesis Paper On The Framework For Pathophysiology: EtiologyTiger Knee100% (1)
- Substance Related DisordersDocument56 pagesSubstance Related DisordersTiger Knee100% (1)
- Sensation Seeking TheoryDocument50 pagesSensation Seeking TheoryTiger Knee100% (1)
- Pathophysiology of Alzheimer's Disease With Nursing ConsiderationsDocument10 pagesPathophysiology of Alzheimer's Disease With Nursing ConsiderationsTiger Knee100% (1)
- PathoPhysiology of Renal Failure (Overview)Document7 pagesPathoPhysiology of Renal Failure (Overview)Tiger Knee100% (3)
- Nasogastric Tube Insertion: Nursing Guidelines and ConsiderationsDocument39 pagesNasogastric Tube Insertion: Nursing Guidelines and ConsiderationsTiger KneeNo ratings yet
- Alzheimer's Disease (Mini Presentation)Document51 pagesAlzheimer's Disease (Mini Presentation)Tiger KneeNo ratings yet
- Myths and CultureDocument4 pagesMyths and CultureTiger KneeNo ratings yet
- Heart in ProgressDocument27 pagesHeart in ProgressTiger KneeNo ratings yet
- Thromboembolic Disease PDFDocument5 pagesThromboembolic Disease PDFBáĦẳá Y. Ẳl-mársǾúmiNo ratings yet
- Stelar System of PlantDocument6 pagesStelar System of Plantworlds tourNo ratings yet
- The Time Machine EssayDocument8 pagesThe Time Machine EssayNicola McCueNo ratings yet
- Section: General ObstetricsDocument15 pagesSection: General ObstetricsvarmaNo ratings yet
- Laboratory Activity 11 - Cardiovascular SystemDocument4 pagesLaboratory Activity 11 - Cardiovascular SystemMV ANo ratings yet
- Sheehan's Syndrome PathophysiologyDocument2 pagesSheehan's Syndrome PathophysiologyirismgallNo ratings yet
- Anti-HG Eng Rev04Document2 pagesAnti-HG Eng Rev04Ventas2lp IcerlabNo ratings yet
- A Fire Death With A Rare Finding: Anthracosis or Soot Embolism? Case ReportDocument5 pagesA Fire Death With A Rare Finding: Anthracosis or Soot Embolism? Case ReportV1QT0R100% (1)
- Rincian Kewenangan Spesialis BedahDocument4 pagesRincian Kewenangan Spesialis BedahAbdul Muthalib PattiihaNo ratings yet
- Gunter Von Hagens 1Document7 pagesGunter Von Hagens 1ChiaraGarbellottoNo ratings yet
- Resource Sheet of Human Organ Systems - 1.2Document3 pagesResource Sheet of Human Organ Systems - 1.2Shelley AllynNo ratings yet
- Kantor 1976, Alv Bone Regeneration After Removal of Inflammatory and Traumatic FactorsDocument9 pagesKantor 1976, Alv Bone Regeneration After Removal of Inflammatory and Traumatic Factorsshir keshalesNo ratings yet
- ReviewerDocument92 pagesReviewerpink_rp1620526No ratings yet
- Full Download Test Bank For Illustrated Anatomy of The Head and Neck 5th Edition by Fehrenbach PDF Full ChapterDocument36 pagesFull Download Test Bank For Illustrated Anatomy of The Head and Neck 5th Edition by Fehrenbach PDF Full Chapterstoredannage1uf100% (17)
- Special Senses Eye and EarDocument60 pagesSpecial Senses Eye and EarTosinNo ratings yet
- Ectopic PregnancyDocument76 pagesEctopic PregnancyVivian Jean TapayaNo ratings yet
- Frogdissectionpre LablilyDocument6 pagesFrogdissectionpre Lablilyapi-347431986No ratings yet
- Male Female Genitalia and Rectum AssessmentDocument76 pagesMale Female Genitalia and Rectum AssessmentKervin EchanoNo ratings yet
- 1st Summative Test Biology 1Document3 pages1st Summative Test Biology 1julzhaideNo ratings yet
- Class 12 Subject: Biology Chapter-2: FlowerDocument30 pagesClass 12 Subject: Biology Chapter-2: FlowerSufiyanNo ratings yet
- 11 Bio Bot - em 23 - 24Document54 pages11 Bio Bot - em 23 - 24Sk Stationary67% (3)
- GametogenesisDocument15 pagesGametogenesisPenuhTandaTanyaNo ratings yet
- Accessing The Healing Power of The Vagus Nerve Self Help Exercises For Anxiety Depression Trauma and Autism (041 050)Document10 pagesAccessing The Healing Power of The Vagus Nerve Self Help Exercises For Anxiety Depression Trauma and Autism (041 050)Fábio ReccanelloNo ratings yet
- ‘21년도 SNOMED CT 활용 현황Document71 pages‘21년도 SNOMED CT 활용 현황Reina HatoriNo ratings yet
- Anatomy Half Book 2Document10 pagesAnatomy Half Book 2Saeed khanNo ratings yet
- PhagocytosisDocument60 pagesPhagocytosisapi-273068056100% (1)
- Exergenie Circa 1970 ManualDocument34 pagesExergenie Circa 1970 ManualJosé Antonio Sánchez AménNo ratings yet
- Blood ChemistryDocument28 pagesBlood ChemistryAisha ShahfiqueeNo ratings yet













































































































Download as docx, pdf, or txt
You might also like
- MedSurg Notes - Cancer of The LiverDocument2 pagesMedSurg Notes - Cancer of The LiverMae CeaesarNo ratings yet
- Urinary Tract Infection Anatomy and PhysiologyDocument12 pagesUrinary Tract Infection Anatomy and PhysiologyPaul Anthony Centeno PimentelNo ratings yet
- Cardiology Case 1Document2 pagesCardiology Case 1vil62650% (2)
- Patho UGIBDocument3 pagesPatho UGIBKristineBungcagNo ratings yet
- The Filipino FamilyDocument11 pagesThe Filipino FamilyTiger Knee97% (38)
- Pathophysiology of Heart FailureDocument4 pagesPathophysiology of Heart FailureTiger Knee100% (2)
- The Development of The Middle Ear Spaces and Their Surgical SignificanceDocument15 pagesThe Development of The Middle Ear Spaces and Their Surgical SignificanceDrTarek Mahmoud Abo Kammer100% (2)
- Microbiology-ELISA Testing Lab ReportDocument2 pagesMicrobiology-ELISA Testing Lab Reportsaraebo33% (3)
- ABRUPTIO PLACENTAE PathophysiologyDocument3 pagesABRUPTIO PLACENTAE PathophysiologyBarda GulanNo ratings yet
- Pathophysiology of Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar Nonketotic Syndrome EtiologyDocument2 pagesPathophysiology of Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar Nonketotic Syndrome EtiologyJaylord VerazonNo ratings yet
- Esophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNDocument20 pagesEsophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNAnn SalvatierraNo ratings yet
- Vii. Pathophysiology A. AlgorithmDocument2 pagesVii. Pathophysiology A. AlgorithmJonna Mae TurquezaNo ratings yet
- Cholelithiasis PathophysiologyDocument2 pagesCholelithiasis PathophysiologyShinrin SukehiroNo ratings yet
- Case Study AGE With Signs of DehydrationDocument27 pagesCase Study AGE With Signs of DehydrationZhenmeiNo ratings yet
- B. Pathophysiology Diagram: A Case Study On UreterolithiasisDocument5 pagesB. Pathophysiology Diagram: A Case Study On UreterolithiasisIan Mizzel A. DulfinaNo ratings yet
- Pathophysiology of Atrial Septal DefectDocument2 pagesPathophysiology of Atrial Septal Defectbobtaguba50% (2)
- Action Plan - Inadequate IncomeDocument2 pagesAction Plan - Inadequate IncomeBenedict James BermasNo ratings yet
- Blood Dyscrasia SDocument24 pagesBlood Dyscrasia SMasha FloreaNo ratings yet
- Case Study Benign Tumors of The Uterus: MyomaDocument3 pagesCase Study Benign Tumors of The Uterus: MyomaToto RyanNo ratings yet
- Pathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsDocument4 pagesPathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsLovely DaroleNo ratings yet
- Cva Concept MapDocument1 pageCva Concept MapAnn Justine OrbetaNo ratings yet
- Acute Cholecystolithiasis - G4 SB2Document125 pagesAcute Cholecystolithiasis - G4 SB2Jeofy PamaNo ratings yet
- PYOMYOSITISDocument6 pagesPYOMYOSITISChristine CoridoNo ratings yet
- DB13 - Pathophysiology of AtherosclerosisDocument2 pagesDB13 - Pathophysiology of Atherosclerosisi_vhie03No ratings yet
- Chronic PyelonephritisDocument5 pagesChronic PyelonephritisIsak ShatikaNo ratings yet
- Pathophysiology of Urinary Tract ObstructionDocument50 pagesPathophysiology of Urinary Tract ObstructionPryo UtamaNo ratings yet
- Acute PyelonephritisDocument105 pagesAcute Pyelonephritisyasira50% (2)
- Pathophysiology of Inflammatory ResponseDocument1 pagePathophysiology of Inflammatory ResponseDeo FactuarNo ratings yet
- V. Pathophysiology Modifiable: Non - ModifiableDocument2 pagesV. Pathophysiology Modifiable: Non - ModifiableMary Grace BanezNo ratings yet
- NSTEMIDocument33 pagesNSTEMIwaazalimahwahidNo ratings yet
- AGE With Pa Tho PhysiologyDocument3 pagesAGE With Pa Tho PhysiologyChichi Licuben OresacamNo ratings yet
- Pathophysiology (Client Base) :: Predisposing Factors: Precipitating FactorsDocument1 pagePathophysiology (Client Base) :: Predisposing Factors: Precipitating Factorsleslie_macasaetNo ratings yet
- Path o PhysiologyDocument9 pagesPath o PhysiologyKyle Ü D. CunanersNo ratings yet
- Tuberculosis PathophysiologyDocument1 pageTuberculosis Pathophysiologymiss RN100% (15)
- Cancer of The ColonDocument8 pagesCancer of The Colonnot your medz duranNo ratings yet
- Diabetes PathoDocument2 pagesDiabetes Pathodrewcel100% (1)
- Pathophysiology Cushing S SyndromeDocument4 pagesPathophysiology Cushing S SyndromeMaria Luisa VillalunaNo ratings yet
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyDocument3 pages"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyCarl Elexer Cuyugan Ano50% (2)
- Pyloric StenosisDocument5 pagesPyloric Stenosisensoooooooooo100% (1)
- Pathophysiology: Prince Carl P. Magluyan BSN - 2GDocument1 pagePathophysiology: Prince Carl P. Magluyan BSN - 2GPrinceNo ratings yet
- Case Presentation of Acute PyelonephritisDocument1 pageCase Presentation of Acute PyelonephritisANALYN ANUBNo ratings yet
- Pernicious AnemiaDocument7 pagesPernicious AnemiaTracy PearlNo ratings yet
- Biomedical Case StudyDocument5 pagesBiomedical Case StudyHannan AtharNo ratings yet
- Pathophysiology-Kni Ns PLZZZDocument8 pagesPathophysiology-Kni Ns PLZZZAnna Lira Manluyang MungcalNo ratings yet
- Hydronephrosis Fred LuceDocument69 pagesHydronephrosis Fred LuceKMNo ratings yet
- Anal Canal: Fissure in Ano HaemorrhoidsDocument37 pagesAnal Canal: Fissure in Ano Haemorrhoidsyash shrivastavaNo ratings yet
- NCP LeukemiaDocument5 pagesNCP LeukemiaTriciaNo ratings yet
- Abruptio PlacentaDocument3 pagesAbruptio Placentachichilovesyou100% (1)
- Venous Thromboembolism (VTE) - McMaster Pathophysiology ReviewDocument9 pagesVenous Thromboembolism (VTE) - McMaster Pathophysiology ReviewFadiyah UlfahNo ratings yet
- Pharmacology m7 Post Task CaparasDocument3 pagesPharmacology m7 Post Task CaparasGretta CaparasNo ratings yet
- Neonatal HyperbilirubinemiaDocument22 pagesNeonatal HyperbilirubinemiaAnkur WadheraNo ratings yet
- Case Study - Dengue Fever V - S UtiDocument12 pagesCase Study - Dengue Fever V - S UtiHarlene Joyce ReyNo ratings yet
- Rheumatic Heart DiseaseDocument3 pagesRheumatic Heart DiseaseDee SarajanNo ratings yet
- Anatomy and Physiology of The GallbladderDocument1 pageAnatomy and Physiology of The GallbladderRojanisa Baculi RomathoNo ratings yet
- PATHOPHYSIOLOGYDocument1 pagePATHOPHYSIOLOGYJeroham CoNo ratings yet
- Normal Values of CBCDocument1 pageNormal Values of CBCCherr NollNo ratings yet
- CPD Concept MapDocument1 pageCPD Concept MapShandle Dynne Baena100% (1)
- Case (Acute Gastroenteritis) Group 4Document36 pagesCase (Acute Gastroenteritis) Group 4EljhayrosNo ratings yet
- NCP CvaDocument4 pagesNCP CvaMariquita BuenafeNo ratings yet
- Malaria: Pathophysiology, Clinical Manifesta6ons and TreatmentDocument14 pagesMalaria: Pathophysiology, Clinical Manifesta6ons and TreatmentGuilhermeNo ratings yet
- CKD - For Concept MappingDocument7 pagesCKD - For Concept MappingKennette Lim0% (1)
- Assessment Nsg. Diagnosis Sci. Explanation Planning Intervention Rationale EvaluationDocument6 pagesAssessment Nsg. Diagnosis Sci. Explanation Planning Intervention Rationale EvaluationRoMarie AbainzaNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Specpro DigestsDocument9 pagesSpecpro DigestsTiger KneeNo ratings yet
- G.R. Nos. 197592 & 20262 November 27, 2013 The Province of Aklan, Petitioner, Jody King Construction and Development Corp., RespondentDocument33 pagesG.R. Nos. 197592 & 20262 November 27, 2013 The Province of Aklan, Petitioner, Jody King Construction and Development Corp., RespondentTiger KneeNo ratings yet
- Breast Cancer AssignmentDocument25 pagesBreast Cancer AssignmentTiger KneeNo ratings yet
- Logic AnswersDocument3 pagesLogic AnswersTiger KneeNo ratings yet
- Voting Number in The ConstitutionDocument2 pagesVoting Number in The ConstitutionTiger KneeNo ratings yet
- Fundamental Distinctions Among Leasehold Tenancy, Tenant Emancipation Decree and CARPDocument17 pagesFundamental Distinctions Among Leasehold Tenancy, Tenant Emancipation Decree and CARPTiger KneeNo ratings yet
- Mens MonthDocument1 pageMens MonthTiger KneeNo ratings yet
- Marriage SettlementsDocument4 pagesMarriage SettlementsTiger KneeNo ratings yet
- Rule 105 Special ProceedingDocument3 pagesRule 105 Special ProceedingTiger KneeNo ratings yet
- Amendments To The Rules of Court On Declaration of Absolute Nullity of Marriage Etc...Document10 pagesAmendments To The Rules of Court On Declaration of Absolute Nullity of Marriage Etc...Tiger KneeNo ratings yet
- Synthesis Paper On The Framework For Pathophysiology: EtiologyDocument4 pagesSynthesis Paper On The Framework For Pathophysiology: EtiologyTiger Knee100% (1)
- Substance Related DisordersDocument56 pagesSubstance Related DisordersTiger Knee100% (1)
- Sensation Seeking TheoryDocument50 pagesSensation Seeking TheoryTiger Knee100% (1)
- Pathophysiology of Alzheimer's Disease With Nursing ConsiderationsDocument10 pagesPathophysiology of Alzheimer's Disease With Nursing ConsiderationsTiger Knee100% (1)
- PathoPhysiology of Renal Failure (Overview)Document7 pagesPathoPhysiology of Renal Failure (Overview)Tiger Knee100% (3)
- Nasogastric Tube Insertion: Nursing Guidelines and ConsiderationsDocument39 pagesNasogastric Tube Insertion: Nursing Guidelines and ConsiderationsTiger KneeNo ratings yet
- Alzheimer's Disease (Mini Presentation)Document51 pagesAlzheimer's Disease (Mini Presentation)Tiger KneeNo ratings yet
- Myths and CultureDocument4 pagesMyths and CultureTiger KneeNo ratings yet
- Heart in ProgressDocument27 pagesHeart in ProgressTiger KneeNo ratings yet
- Thromboembolic Disease PDFDocument5 pagesThromboembolic Disease PDFBáĦẳá Y. Ẳl-mársǾúmiNo ratings yet
- Stelar System of PlantDocument6 pagesStelar System of Plantworlds tourNo ratings yet
- The Time Machine EssayDocument8 pagesThe Time Machine EssayNicola McCueNo ratings yet
- Section: General ObstetricsDocument15 pagesSection: General ObstetricsvarmaNo ratings yet
- Laboratory Activity 11 - Cardiovascular SystemDocument4 pagesLaboratory Activity 11 - Cardiovascular SystemMV ANo ratings yet
- Sheehan's Syndrome PathophysiologyDocument2 pagesSheehan's Syndrome PathophysiologyirismgallNo ratings yet
- Anti-HG Eng Rev04Document2 pagesAnti-HG Eng Rev04Ventas2lp IcerlabNo ratings yet
- A Fire Death With A Rare Finding: Anthracosis or Soot Embolism? Case ReportDocument5 pagesA Fire Death With A Rare Finding: Anthracosis or Soot Embolism? Case ReportV1QT0R100% (1)
- Rincian Kewenangan Spesialis BedahDocument4 pagesRincian Kewenangan Spesialis BedahAbdul Muthalib PattiihaNo ratings yet
- Gunter Von Hagens 1Document7 pagesGunter Von Hagens 1ChiaraGarbellottoNo ratings yet
- Resource Sheet of Human Organ Systems - 1.2Document3 pagesResource Sheet of Human Organ Systems - 1.2Shelley AllynNo ratings yet
- Kantor 1976, Alv Bone Regeneration After Removal of Inflammatory and Traumatic FactorsDocument9 pagesKantor 1976, Alv Bone Regeneration After Removal of Inflammatory and Traumatic Factorsshir keshalesNo ratings yet
- ReviewerDocument92 pagesReviewerpink_rp1620526No ratings yet
- Full Download Test Bank For Illustrated Anatomy of The Head and Neck 5th Edition by Fehrenbach PDF Full ChapterDocument36 pagesFull Download Test Bank For Illustrated Anatomy of The Head and Neck 5th Edition by Fehrenbach PDF Full Chapterstoredannage1uf100% (17)
- Special Senses Eye and EarDocument60 pagesSpecial Senses Eye and EarTosinNo ratings yet
- Ectopic PregnancyDocument76 pagesEctopic PregnancyVivian Jean TapayaNo ratings yet
- Frogdissectionpre LablilyDocument6 pagesFrogdissectionpre Lablilyapi-347431986No ratings yet
- Male Female Genitalia and Rectum AssessmentDocument76 pagesMale Female Genitalia and Rectum AssessmentKervin EchanoNo ratings yet
- 1st Summative Test Biology 1Document3 pages1st Summative Test Biology 1julzhaideNo ratings yet
- Class 12 Subject: Biology Chapter-2: FlowerDocument30 pagesClass 12 Subject: Biology Chapter-2: FlowerSufiyanNo ratings yet
- 11 Bio Bot - em 23 - 24Document54 pages11 Bio Bot - em 23 - 24Sk Stationary67% (3)
- GametogenesisDocument15 pagesGametogenesisPenuhTandaTanyaNo ratings yet
- Accessing The Healing Power of The Vagus Nerve Self Help Exercises For Anxiety Depression Trauma and Autism (041 050)Document10 pagesAccessing The Healing Power of The Vagus Nerve Self Help Exercises For Anxiety Depression Trauma and Autism (041 050)Fábio ReccanelloNo ratings yet
- ‘21년도 SNOMED CT 활용 현황Document71 pages‘21년도 SNOMED CT 활용 현황Reina HatoriNo ratings yet
- Anatomy Half Book 2Document10 pagesAnatomy Half Book 2Saeed khanNo ratings yet
- PhagocytosisDocument60 pagesPhagocytosisapi-273068056100% (1)
- Exergenie Circa 1970 ManualDocument34 pagesExergenie Circa 1970 ManualJosé Antonio Sánchez AménNo ratings yet
- Blood ChemistryDocument28 pagesBlood ChemistryAisha ShahfiqueeNo ratings yet