
20twelve SnowJam PermSlip
20twelve SnowJam PermSlip
You might also like
- Statement of Marital SeparationDocument1 pageStatement of Marital Separationlapitanmaricar21No ratings yet
- SH Summer Events 2012Document2 pagesSH Summer Events 2012NMCStuMinNo ratings yet
- Kings Island Permission SlipDocument1 pageKings Island Permission SlipTanya SeibelNo ratings yet
- RLTP Institute & Audition Prep Registration Form 2013Document4 pagesRLTP Institute & Audition Prep Registration Form 2013Gina G-LoNo ratings yet
- Parental Consent FormDocument6 pagesParental Consent FormZander Alexis BonnevieNo ratings yet
- Field Trip Permission Slip FillableDocument1 pageField Trip Permission Slip Fillabletvtcf286v9No ratings yet
- Student Medial Release FormDocument3 pagesStudent Medial Release FormdanielwebmasterNo ratings yet
- Permission SlipDocument1 pagePermission Slipapi-250426898No ratings yet
- Parent Consent FormDocument1 pageParent Consent Formprakash yadavNo ratings yet
- School WaiverDocument3 pagesSchool WaiverMarlon SolanoNo ratings yet
- Parent Guardian Informed ConsentDocument1 pageParent Guardian Informed Consentapi-425900848No ratings yet
- PCS Field Trip Consent FormDocument1 pagePCS Field Trip Consent FormJaneNo ratings yet
- Camp Jeff Waiver Form - 2021Document2 pagesCamp Jeff Waiver Form - 2021Nolan HahnNo ratings yet
- HealthAndSafetyForm 170118Document2 pagesHealthAndSafetyForm 170118Bonga DubeNo ratings yet
- Blank in CampusDocument1 pageBlank in CampusZACK GEOFREE TALUSIGNo ratings yet
- 2012 An GP Risk FormsDocument5 pages2012 An GP Risk FormsRittick GuptaNo ratings yet
- Consent Form & Sponsorship Request DataDocument2 pagesConsent Form & Sponsorship Request DataJoseph BoylesNo ratings yet
- Permission Slip For Christmas Party and CarolingDocument2 pagesPermission Slip For Christmas Party and CarolingMarisol Doroin MendozaNo ratings yet
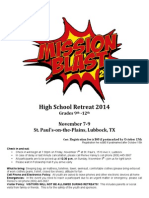
- Mission Blast 2014Document4 pagesMission Blast 2014Renee Plummer HaneyNo ratings yet
- Parents' Consent and Waiver:: Student Trip/Travel and ParticipationDocument1 pageParents' Consent and Waiver:: Student Trip/Travel and ParticipationSadhji CrossroadNo ratings yet
- Swimming PermissionDocument2 pagesSwimming PermissionRick StewartNo ratings yet
- Parental Consent FormDocument1 pageParental Consent FormMatt IrvineNo ratings yet
- REEA Membership ApplicationDocument3 pagesREEA Membership ApplicationWicondraNo ratings yet
- TRCV YouthWaiver 2017Document1 pageTRCV YouthWaiver 2017v4n931No ratings yet
- Travel and Trip Risk Acknowledgement Liability Waiver FormDocument4 pagesTravel and Trip Risk Acknowledgement Liability Waiver Formapi-357423998No ratings yet
- NYC Missions Team Application DUE BY 01/27/13Document2 pagesNYC Missions Team Application DUE BY 01/27/13flmyamNo ratings yet
- Spring Con Reg. 09Document7 pagesSpring Con Reg. 09YACNNED2869No ratings yet
- UpdatedAtlanta Public Schools - Registration FormDocument2 pagesUpdatedAtlanta Public Schools - Registration Formglobetrek@1No ratings yet
- Parental Consent & Waiver Form: Child's Name: Destination: DateDocument1 pageParental Consent & Waiver Form: Child's Name: Destination: DateDonna Guzon AlteaNo ratings yet
- Camp Highland - Adult Medical-Liability FormDocument1 pageCamp Highland - Adult Medical-Liability FormMark AdamsNo ratings yet
- Parent'S/Guardian'S Consent Form Parent'S/Guardian'S Consent FormDocument2 pagesParent'S/Guardian'S Consent Form Parent'S/Guardian'S Consent FormAimee Amor Cardines PortoNo ratings yet
- Field Day Permission SlipDocument4 pagesField Day Permission SlipCasey SchmollNo ratings yet
- Parental Consent & Waiver Form For Field TripsDocument1 pageParental Consent & Waiver Form For Field TripsClaire ElyseNo ratings yet
- Parent Consent Form Camp 2023Document1 pageParent Consent Form Camp 2023Mylykhan LucasNo ratings yet
- Form B - Event SpecificDocument1 pageForm B - Event Specificapi-261673643No ratings yet
- Parental Consent or WaiverDocument1 pageParental Consent or WaiverNikki CrystelNo ratings yet
- Parental/Guardian Permission and Liability Waiver Name of Student BirthDocument2 pagesParental/Guardian Permission and Liability Waiver Name of Student BirthlifeteenministryNo ratings yet
- High School Field Trip Permission SlipDocument2 pagesHigh School Field Trip Permission Slipmunash2kumarNo ratings yet
- What Is Deep Freeze?: Thursday, Dec. 20 - If You've Got Any Questions Call Mark or Sabrina atDocument4 pagesWhat Is Deep Freeze?: Thursday, Dec. 20 - If You've Got Any Questions Call Mark or Sabrina atMark DurksenNo ratings yet
- Registration and ConsentDocument1 pageRegistration and ConsentcbcyouthNo ratings yet
- School WaiverDocument2 pagesSchool WaiverMarlon SolanoNo ratings yet
- Category 3 Consent FormDocument1 pageCategory 3 Consent FormrelonzNo ratings yet
- 2012 Camp Superstars Registration FormDocument2 pages2012 Camp Superstars Registration FormDennis HendNo ratings yet
- Field TripDocument1 pageField Tripapi-231128403No ratings yet
- Person To Contact in Case of EmergencyDocument1 pagePerson To Contact in Case of EmergencyIrishJialGinezNo ratings yet
- JR High 2010 Registration FormDocument4 pagesJR High 2010 Registration FormryanlashleeNo ratings yet
- ASY Reg Summercamp2012Document2 pagesASY Reg Summercamp2012ASYMCA YCONo ratings yet
- Kids Fit 2016 RegistrationDocument3 pagesKids Fit 2016 RegistrationwiamNo ratings yet
- United Summer Vibe Bubble BallDocument1 pageUnited Summer Vibe Bubble BallLaceyNo ratings yet
- Consent Form and Payment Letter FOBISIA Orchestra and Choral Festival Indonesia May 2024Document4 pagesConsent Form and Payment Letter FOBISIA Orchestra and Choral Festival Indonesia May 2024sage.ebony.meadowNo ratings yet
- Amazing Jump PermissionDocument2 pagesAmazing Jump PermissionRick StewartNo ratings yet
- DS2 - Swimming Lesson and Pool Consent FormDocument1 pageDS2 - Swimming Lesson and Pool Consent Formhasoxow489No ratings yet
- Liability and Consent FormDocument2 pagesLiability and Consent Formapi-19917129No ratings yet
- Parent Consent and Waiver FormDocument5 pagesParent Consent and Waiver FormBenjie T Madayag100% (4)
- Field Trip Permission SlipDocument4 pagesField Trip Permission SlipRishi SinghNo ratings yet
- Natcon Parental Consent and WaiverDocument2 pagesNatcon Parental Consent and WaiverReyo VillanuevaNo ratings yet
- 2011 GAME Waiver FormDocument1 page2011 GAME Waiver FormBrian LaRueNo ratings yet
- Volunteer FormsDocument3 pagesVolunteer Formssholly6219No ratings yet
- PARENTS Waiver For DAYAW 2024Document1 pagePARENTS Waiver For DAYAW 2024ferdinandbarnachea09No ratings yet
- Reverse Conference InfoDocument1 pageReverse Conference InfoPhil de MartimpreyNo ratings yet
- 2013 Summer CalendarDocument1 page2013 Summer CalendarPhil de MartimpreyNo ratings yet
- Reverse Conference InfoDocument1 pageReverse Conference InfoPhil de MartimpreyNo ratings yet
- Snow Jam Info and Permission SlipDocument2 pagesSnow Jam Info and Permission SlipPhil de MartimpreyNo ratings yet
- Operation Christmas Child 2012Document2 pagesOperation Christmas Child 2012Phil de MartimpreyNo ratings yet
- Lock in Permission SlipDocument2 pagesLock in Permission SlipPhil de MartimpreyNo ratings yet
- Wildwood Permission SlipDocument1 pageWildwood Permission SlipPhil de MartimpreyNo ratings yet
- 20twelve Snow Jam Flyer InfoDocument1 page20twelve Snow Jam Flyer InfoPhil de MartimpreyNo ratings yet
- 2011 Wildwood FlyerDocument2 pages2011 Wildwood FlyerPhil de MartimpreyNo ratings yet




































































Download as doc, pdf, or txt
You might also like
- Statement of Marital SeparationDocument1 pageStatement of Marital Separationlapitanmaricar21No ratings yet
- SH Summer Events 2012Document2 pagesSH Summer Events 2012NMCStuMinNo ratings yet
- Kings Island Permission SlipDocument1 pageKings Island Permission SlipTanya SeibelNo ratings yet
- RLTP Institute & Audition Prep Registration Form 2013Document4 pagesRLTP Institute & Audition Prep Registration Form 2013Gina G-LoNo ratings yet
- Parental Consent FormDocument6 pagesParental Consent FormZander Alexis BonnevieNo ratings yet
- Field Trip Permission Slip FillableDocument1 pageField Trip Permission Slip Fillabletvtcf286v9No ratings yet
- Student Medial Release FormDocument3 pagesStudent Medial Release FormdanielwebmasterNo ratings yet
- Permission SlipDocument1 pagePermission Slipapi-250426898No ratings yet
- Parent Consent FormDocument1 pageParent Consent Formprakash yadavNo ratings yet
- School WaiverDocument3 pagesSchool WaiverMarlon SolanoNo ratings yet
- Parent Guardian Informed ConsentDocument1 pageParent Guardian Informed Consentapi-425900848No ratings yet
- PCS Field Trip Consent FormDocument1 pagePCS Field Trip Consent FormJaneNo ratings yet
- Camp Jeff Waiver Form - 2021Document2 pagesCamp Jeff Waiver Form - 2021Nolan HahnNo ratings yet
- HealthAndSafetyForm 170118Document2 pagesHealthAndSafetyForm 170118Bonga DubeNo ratings yet
- Blank in CampusDocument1 pageBlank in CampusZACK GEOFREE TALUSIGNo ratings yet
- 2012 An GP Risk FormsDocument5 pages2012 An GP Risk FormsRittick GuptaNo ratings yet
- Consent Form & Sponsorship Request DataDocument2 pagesConsent Form & Sponsorship Request DataJoseph BoylesNo ratings yet
- Permission Slip For Christmas Party and CarolingDocument2 pagesPermission Slip For Christmas Party and CarolingMarisol Doroin MendozaNo ratings yet
- Mission Blast 2014Document4 pagesMission Blast 2014Renee Plummer HaneyNo ratings yet
- Parents' Consent and Waiver:: Student Trip/Travel and ParticipationDocument1 pageParents' Consent and Waiver:: Student Trip/Travel and ParticipationSadhji CrossroadNo ratings yet
- Swimming PermissionDocument2 pagesSwimming PermissionRick StewartNo ratings yet
- Parental Consent FormDocument1 pageParental Consent FormMatt IrvineNo ratings yet
- REEA Membership ApplicationDocument3 pagesREEA Membership ApplicationWicondraNo ratings yet
- TRCV YouthWaiver 2017Document1 pageTRCV YouthWaiver 2017v4n931No ratings yet
- Travel and Trip Risk Acknowledgement Liability Waiver FormDocument4 pagesTravel and Trip Risk Acknowledgement Liability Waiver Formapi-357423998No ratings yet
- NYC Missions Team Application DUE BY 01/27/13Document2 pagesNYC Missions Team Application DUE BY 01/27/13flmyamNo ratings yet
- Spring Con Reg. 09Document7 pagesSpring Con Reg. 09YACNNED2869No ratings yet
- UpdatedAtlanta Public Schools - Registration FormDocument2 pagesUpdatedAtlanta Public Schools - Registration Formglobetrek@1No ratings yet
- Parental Consent & Waiver Form: Child's Name: Destination: DateDocument1 pageParental Consent & Waiver Form: Child's Name: Destination: DateDonna Guzon AlteaNo ratings yet
- Camp Highland - Adult Medical-Liability FormDocument1 pageCamp Highland - Adult Medical-Liability FormMark AdamsNo ratings yet
- Parent'S/Guardian'S Consent Form Parent'S/Guardian'S Consent FormDocument2 pagesParent'S/Guardian'S Consent Form Parent'S/Guardian'S Consent FormAimee Amor Cardines PortoNo ratings yet
- Field Day Permission SlipDocument4 pagesField Day Permission SlipCasey SchmollNo ratings yet
- Parental Consent & Waiver Form For Field TripsDocument1 pageParental Consent & Waiver Form For Field TripsClaire ElyseNo ratings yet
- Parent Consent Form Camp 2023Document1 pageParent Consent Form Camp 2023Mylykhan LucasNo ratings yet
- Form B - Event SpecificDocument1 pageForm B - Event Specificapi-261673643No ratings yet
- Parental Consent or WaiverDocument1 pageParental Consent or WaiverNikki CrystelNo ratings yet
- Parental/Guardian Permission and Liability Waiver Name of Student BirthDocument2 pagesParental/Guardian Permission and Liability Waiver Name of Student BirthlifeteenministryNo ratings yet
- High School Field Trip Permission SlipDocument2 pagesHigh School Field Trip Permission Slipmunash2kumarNo ratings yet
- What Is Deep Freeze?: Thursday, Dec. 20 - If You've Got Any Questions Call Mark or Sabrina atDocument4 pagesWhat Is Deep Freeze?: Thursday, Dec. 20 - If You've Got Any Questions Call Mark or Sabrina atMark DurksenNo ratings yet
- Registration and ConsentDocument1 pageRegistration and ConsentcbcyouthNo ratings yet
- School WaiverDocument2 pagesSchool WaiverMarlon SolanoNo ratings yet
- Category 3 Consent FormDocument1 pageCategory 3 Consent FormrelonzNo ratings yet
- 2012 Camp Superstars Registration FormDocument2 pages2012 Camp Superstars Registration FormDennis HendNo ratings yet
- Field TripDocument1 pageField Tripapi-231128403No ratings yet
- Person To Contact in Case of EmergencyDocument1 pagePerson To Contact in Case of EmergencyIrishJialGinezNo ratings yet
- JR High 2010 Registration FormDocument4 pagesJR High 2010 Registration FormryanlashleeNo ratings yet
- ASY Reg Summercamp2012Document2 pagesASY Reg Summercamp2012ASYMCA YCONo ratings yet
- Kids Fit 2016 RegistrationDocument3 pagesKids Fit 2016 RegistrationwiamNo ratings yet
- United Summer Vibe Bubble BallDocument1 pageUnited Summer Vibe Bubble BallLaceyNo ratings yet
- Consent Form and Payment Letter FOBISIA Orchestra and Choral Festival Indonesia May 2024Document4 pagesConsent Form and Payment Letter FOBISIA Orchestra and Choral Festival Indonesia May 2024sage.ebony.meadowNo ratings yet
- Amazing Jump PermissionDocument2 pagesAmazing Jump PermissionRick StewartNo ratings yet
- DS2 - Swimming Lesson and Pool Consent FormDocument1 pageDS2 - Swimming Lesson and Pool Consent Formhasoxow489No ratings yet
- Liability and Consent FormDocument2 pagesLiability and Consent Formapi-19917129No ratings yet
- Parent Consent and Waiver FormDocument5 pagesParent Consent and Waiver FormBenjie T Madayag100% (4)
- Field Trip Permission SlipDocument4 pagesField Trip Permission SlipRishi SinghNo ratings yet
- Natcon Parental Consent and WaiverDocument2 pagesNatcon Parental Consent and WaiverReyo VillanuevaNo ratings yet
- 2011 GAME Waiver FormDocument1 page2011 GAME Waiver FormBrian LaRueNo ratings yet
- Volunteer FormsDocument3 pagesVolunteer Formssholly6219No ratings yet
- PARENTS Waiver For DAYAW 2024Document1 pagePARENTS Waiver For DAYAW 2024ferdinandbarnachea09No ratings yet
- Reverse Conference InfoDocument1 pageReverse Conference InfoPhil de MartimpreyNo ratings yet
- 2013 Summer CalendarDocument1 page2013 Summer CalendarPhil de MartimpreyNo ratings yet
- Reverse Conference InfoDocument1 pageReverse Conference InfoPhil de MartimpreyNo ratings yet
- Snow Jam Info and Permission SlipDocument2 pagesSnow Jam Info and Permission SlipPhil de MartimpreyNo ratings yet
- Operation Christmas Child 2012Document2 pagesOperation Christmas Child 2012Phil de MartimpreyNo ratings yet
- Lock in Permission SlipDocument2 pagesLock in Permission SlipPhil de MartimpreyNo ratings yet
- Wildwood Permission SlipDocument1 pageWildwood Permission SlipPhil de MartimpreyNo ratings yet
- 20twelve Snow Jam Flyer InfoDocument1 page20twelve Snow Jam Flyer InfoPhil de MartimpreyNo ratings yet
- 2011 Wildwood FlyerDocument2 pages2011 Wildwood FlyerPhil de MartimpreyNo ratings yet